Download de presentatie
De presentatie wordt gedownload. Even geduld aub

1
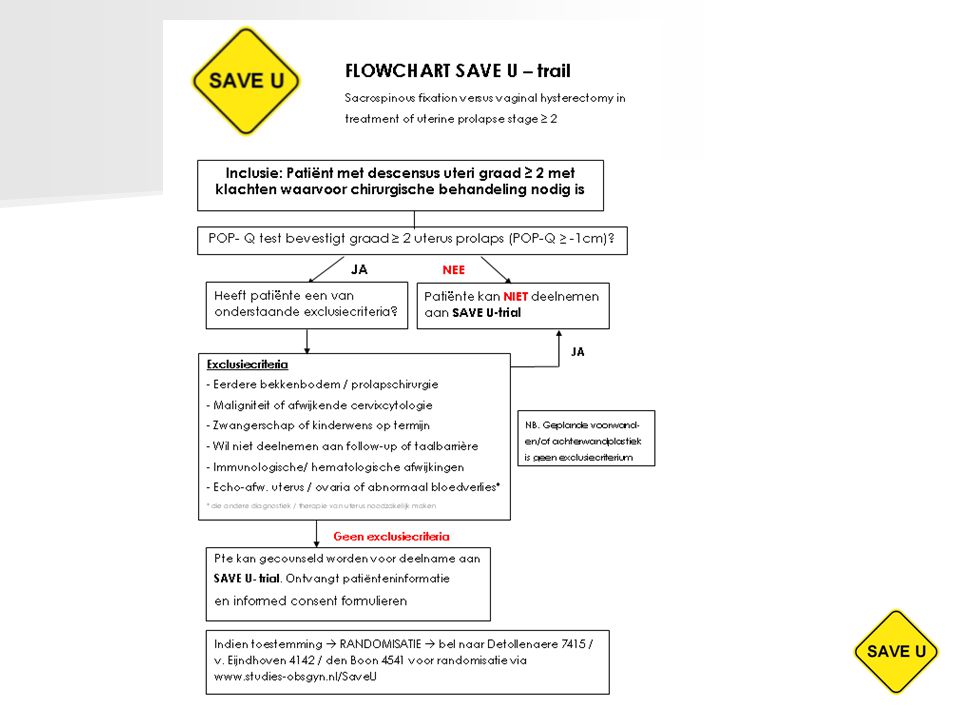
Sacrospinous Fixation Versus Vaginal Hysterectomy in Treatment of Uterine Prolapse Stage ≥ 2
SAVE U trial R.J. Detollenaere H.W.F. van Eijndhoven J. den Boon

2
Introductie 29% heroperatie ivm recidief prolaps
Life time risico prolapschirurgie 11% 29% heroperatie ivm recidief prolaps Hysterectomie wereldwijd standaardbehandeling voor descensus uteri incidentie topprolaps: 0,2-12% risico op blaasdisfunctie / incontinentie? Olsen AL, Smith VJ, Bergstrom JO, Colling JC, Clark AL. Epidemiology of surgically managed pelvic organ prolapse and urinary incontinence. Obstet Gynecol 1997;89:501-6 Marchionni M, Bracco GL, Checcucci V, Carabaneanu A, Coccia EM, Mecacci F et al (1999) True incidence of vaginal vault prolapse. Thirteen years of experience. J Reprod Med 44: 679–684 Altman D, Granath F, Cnattingius S, Falconer C. Hysterectomy and risk of stress-urinary-incontinence surgery: nationwide cohort study. Lancet 2007 Oct 27;370(9597):
 True incidence of vaginal vault prolapse. Thirteen years of experience. J Reprod Med 44: 679–684. Altman D, Granath F, Cnattingius S, Falconer C. Hysterectomy and risk of stress-urinary-incontinence surgery: nationwide cohort study. Lancet Oct 27;370(9597):")
3
Doel studie Vaststellen meest effectieve en veilige
strategie bij descensus uteri graad 2 of meer.

4
Klinisch probleem P: Descensus uteri graad 2 of meer
I: Sacrospinale fixatie C: Vaginale hysterectomie O: Recidief prolaps

5
Literatuur VUE vs SSF 2 retrospectieve, 1 prospectieve studie
geen verschil anatomisch resultaat, wel sneller herstel en kortere opnameduur na SSF Slechts 1 RCT: Dietz et al (thesis) Na 1 jaar meer recidief na SSF (27% vs 3%) Echter kleine sample size (n= 66) Maher CF, Cary MP, Slack MC, Murray CJ, Milligan M, Schluter P. Uterine preservation or hysterectomy at sacrospinous colpopexy for uterovaginal rolapse? Int Urogynecol J 2001;12: Brummen HJ, van de Pol G, Aalders CIM, Heintz APM, van der Vaart. Sacrospinous hysteropexy compared to vaginal hysterectomy as primary surgical treatment for a descensus uteri: effect on urinary symptoms . Int Urogynecol J 2003;14: Henfi MA, El-Toukhy TA. Long-term outcome of vaginal sacrospinous colpopexy for marked uterovaginal and vault prolapse. Eur J Obstet Gynecol Reprod Biol 2006; 127(2):
 Na 1 jaar meer recidief na SSF (27% vs 3%) Echter kleine sample size (n= 66) Maher CF, Cary MP, Slack MC, Murray CJ, Milligan M, Schluter P. Uterine preservation or hysterectomy at sacrospinous colpopexy for uterovaginal rolapse Int Urogynecol J 2001;12: Brummen HJ, van de Pol G, Aalders CIM, Heintz APM, van der Vaart. Sacrospinous hysteropexy compared to vaginal hysterectomy as primary surgical treatment for a descensus uteri: effect on urinary symptoms . Int Urogynecol J 2003;14: Henfi MA, El-Toukhy TA. Long-term outcome of vaginal sacrospinous colpopexy for marked uterovaginal and vault prolapse. Eur J Obstet Gynecol Reprod Biol 2006; 127(2):")
6
Hypothese Gelijk of minder recidief prolaps na SSF
Retrospectieve case study n=285 n=229 prolaps uterus n= 56 topprolaps Failure rate 7,75 (22/285) Recidief descensus uteri: 0,9% (2/229) NB. Geen complete follow up data
 Recidief descensus uteri: 0,9% (2/229) NB. Geen complete follow up data.")
7
Inclusiecriteria Alle vrouwen met een descensus uteri graad 2 of meer
Aanvullende voor- en/of achterwandplastiek of incontinentiechirurgie geen bezwaar voor deelname Informed consent

8
Exclusiecriteria Bekkenbodem / prolapschirurgie in voorgeschiedenis
Maligniteit of afwijkende PAP-smear Wens tot behoud fertiliteit Patiënte heeft problemen met langdurige follow-up of onvoldoende begrip van de Nederlandse taal Bekend met hematologische / immunologische aandoening die postoperatief herstel beinvloedt Afwijking van uterus en/of ovaria bij echografie, abnormaal vaginaal bloedverlies

10
Interventies Groep 1: VUE Groep 2: SSF

11
Primaire uitkomstmaat
Anatomisch resultaat POP-Q na 6 wkn, 6 mnd, 12 mnd en daarna jaarlijks tot 60 mnd follow-up Recidief in middelste compartiment Recidief in voorste/achterste compartiment

12
Secundaire uitkomstmaten
Kwaliteit van leven (SF-36, UDI, DDI, IIQ, EQ-5D) Complicaties Opnameduur Postoperatief herstel (VAS pijnscore, pijnstilling,RI-10) Seksueel functioneren (VSD + PISQ)
 Complicaties. Opnameduur. Postoperatief herstel (VAS pijnscore, pijnstilling,RI-10) Seksueel functioneren (VSD + PISQ)")
13
Poweranalyse Non-inferiority design
Relapse rate 3% en 80% power for a non-inferiority margin of 7%, assuming a relapse rate of 3%. Considering a 10% loss in follow-up 104 women per arm are needed and thus a total of 208 women.

14
Deelnemende centra Isala Klinieken Zwolle Medisch Centrum Leeuwarden
Sint Jan Kliniek Brussel Ziekenhuis Groep Twente, locatie Hengelo

15
Poli pte is kandidaat voor de studie
Pre-operatieve anamnese: mictie, defaecatie, seksualiteit, (gyn) VG, medicatie en intoxicatie, allergie Gynaecologisch onderzoek preoperatief inclusief een volledig POP-Q (+ echo en PAP-smear!!!) Patiënte counselen !!!! Counseling : VUE aanbieden. VUE is de standaardbehandeling, SSF de te onderzoeken interventie!!!! Meegeven patiënteninfo; vragenlijst A en formulier toestemming en antwoordenvelop Indien consent randomisatie via
 VG, medicatie en intoxicatie, allergie. Gynaecologisch onderzoek preoperatief inclusief een volledig. POP-Q (+ echo en PAP-smear!!!) Patiënte counselen. !!!! Counseling : VUE aanbieden. VUE is de standaardbehandeling, SSF de te onderzoeken interventie!!!! Meegeven patiënteninfo; vragenlijst A en formulier toestemming en antwoordenvelop. Indien consent randomisatie via")
16
OK procedure SSF op gestandaardiseerde wijze (open techniek met 3 specula en 2 prolene 1-0 hechtingen a vue door het lig SS rechts) VUE op standaard wijze lig. sacro-uterina vast op top

17
Samenvatting SAVE U = SSF vs vaginale hysterectomie in
behandeling van descensus uteri graad ≥ 2 Start inclusie november 2009, +/- 24 maanden inclusie, 208 patiënten.

18
POP-Q

19
POP-Q

Verwante presentaties




 Alhoewel veel behandelingen in de geneeskunde dagelijks worden toegepast, is er vaak geen duidelijk bewijs dat zo'n.>")











CONTINENTIE ORKEST>")


