Download de presentatie
De presentatie wordt gedownload. Even geduld aub

1
HIV en de lever Het monitoren van leverproblemen door de SHM
c.richter, rijnstate ziekenhuis

2
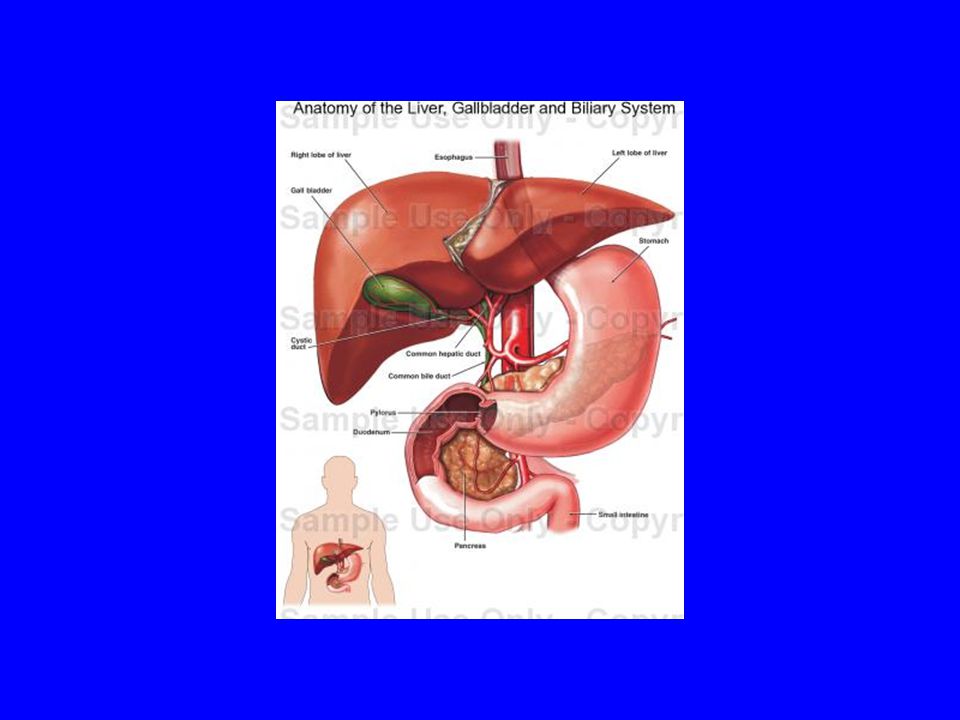
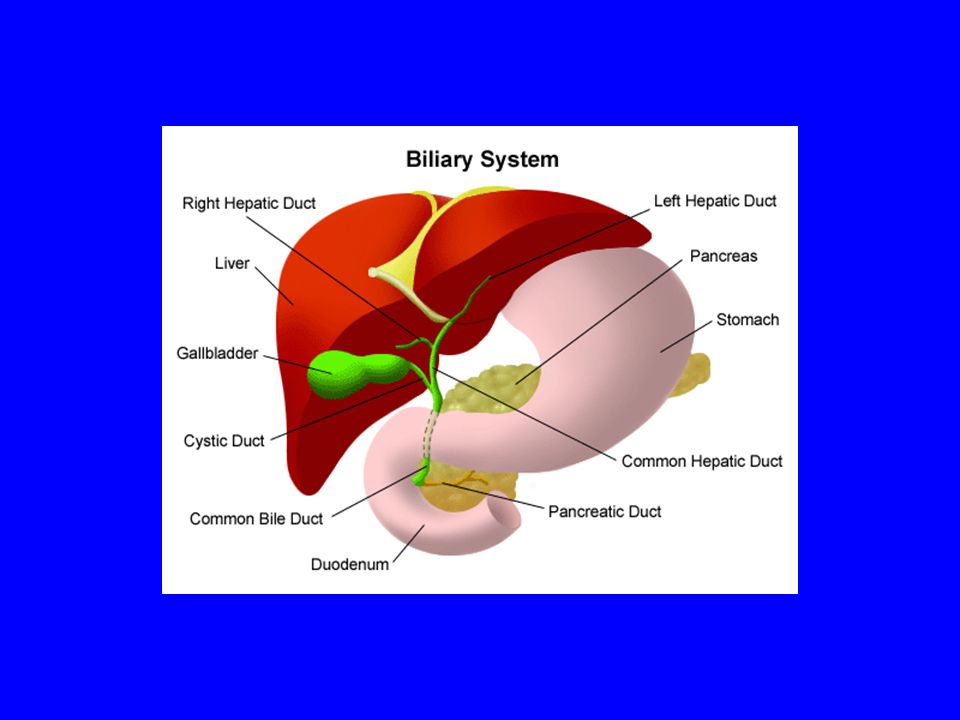
overzicht De anatomie en functie van de lever
Symptomen, lichamelijk onderzoek Oorzaken van leverproblemen Diagnostiek, markers van leverproblemen Ontsteking, fibrose, cirrhose, HCC Hepatitis B en C

6
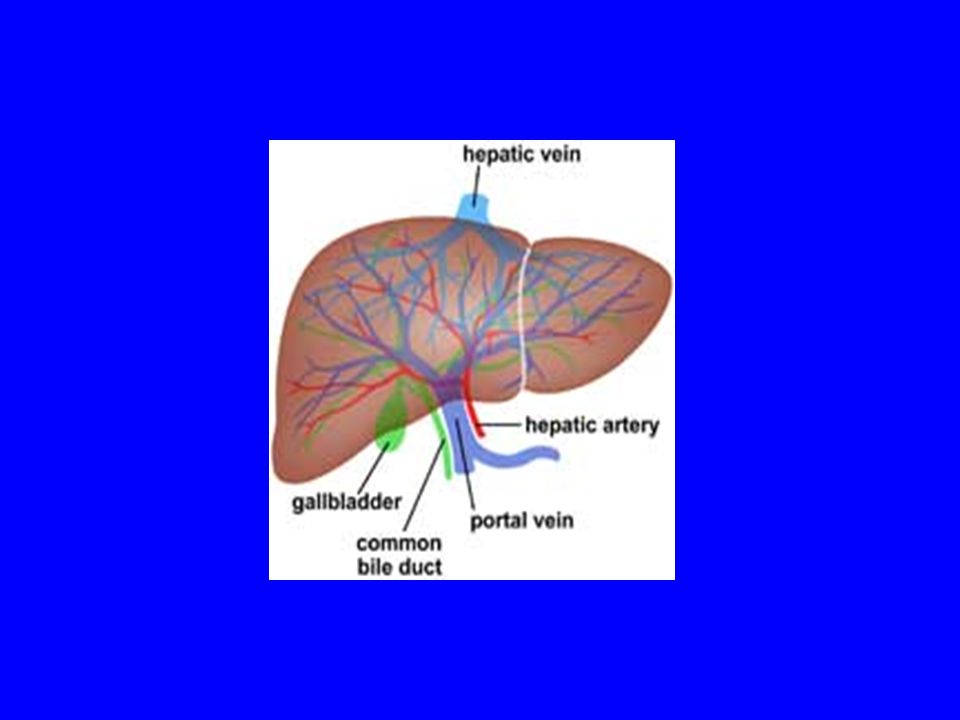
De lever is het grootste orgaan, 1-1.5kg
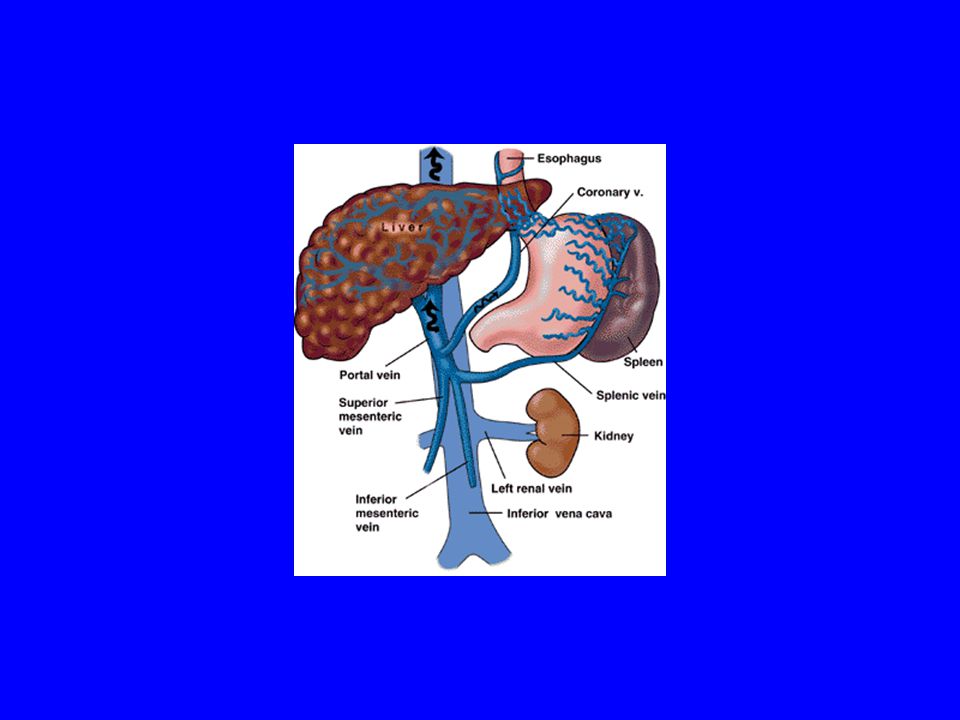
Dubbele bloedtoevoer: zuurstofrijk bloed via de leverarterie (20%) - en voedingsstofrijk bloed via de vena porta afkomstig van maag, darmen, alvleesklier en milt (80%) Enterohepatische kringloop via uitscheiding van gal naar de dunne darm
 - en voedingsstofrijk bloed via de vena porta afkomstig van maag, darmen, alvleesklier en milt (80%) Enterohepatische kringloop via uitscheiding van gal naar de dunne darm.")
7
Functie van de lever Verwerking/regulatie van voedingsstoffen (glucose, aminozuren etc) en vitaminen Verwerking (metaboliseren) en binding van bilirubine en geneesmiddelen Aanmaak van albumine en stollingsfactoren nog vele andere functies
 en binding van bilirubine en geneesmiddelen. Aanmaak van albumine en stollingsfactoren. nog vele andere functies.")
8
Basic functions of the liver
Digestion (bile production) by absorption of fat and certain vitamins, including vitamins A, D, E, and K Absorption of nutrients Metabolism regulation of glucose Detoxifying medications and toxins Storage Produces important proteins including haemostatic factors Production of cholesterol Immunological functions Hepatobiliary disease Assessment of liver disease includes hepatobiliary pancreatic disease 8
 by absorption of fat and certain vitamins, including vitamins A, D, E, and K. Absorption of nutrients. Metabolism regulation of glucose. Detoxifying medications and toxins. Storage. Produces important proteins including haemostatic factors. Production of cholesterol. Immunological functions. Hepatobiliary disease. Assessment of liver disease includes hepatobiliary pancreatic disease. 8.")
9
Symptomen van leverziekte/ galwegsprobleem
Moeheid Verminderde eetlust, gewichtsverlies Jeuk (vooral bij “cholestasis”=galstuwing Geelzucht Stopverfontlasting/donkere urine (bij belemmering galafvloed)
")
11
Lichamelijk onderzoek, mogelijke afwijkingen
Ikterus Prurigo nodularis, lichen planus (bij hepatitis C) Spider naevi Palmaar erytheem Ascites Caput medusae Grote milt Oedeem Testisatrofie, gynaecomastie –bij mannen
 Spider naevi. Palmaar erytheem. Ascites. Caput medusae. Grote milt. Oedeem. Testisatrofie, gynaecomastie –bij mannen.")
13
Prurigo nodularis bij hepatitis C

14
Lichen planus bij hepatitis C

15
A en B normale lever, C en D cirrhosis

17
Symptomen bij levercirrhose
Hematemesis (bloedbraken), melaena (zwarte brijige ontlasting) Sexuele dysfunctie en gynaecomastie en testisatrofie bij mannen Nachtelijke spierkrampen Opgezet abdomen door ascites, oedeem benen Veranderd bewustzijn, gedrag, verwardheid, desorientatie, coma (tgv encephalopathie)
, melaena (zwarte brijige ontlasting) Sexuele dysfunctie en gynaecomastie en testisatrofie bij mannen. Nachtelijke spierkrampen. Opgezet abdomen door ascites, oedeem benen. Veranderd bewustzijn, gedrag, verwardheid, desorientatie, coma (tgv encephalopathie)")
18
Common signs of advanced liver disease
ascites Palmar erythema Spider naevi with blanching

19
Palmaar erytheem

20
ascites

21
Pitting oedeem

22
Probleem van leverprobleem bij HIV- patiënten
Er zijn vele oorzaken!

23
Liver disease in HIV: raised aminotransferases
HCV or HBV Immune Restoration Disease Direct Cytotoxicity Chronic Hepatitis Alcohol Drugs Medications Drug-related Hepatotoxicity NASH HIV HAART

24
Causes of liver disease in HIV infection
There are numerous possible causes of liver disease in the context of HIV infection including hepatitis viruses, other opportunistic infections, drugs, and immune reconstitution inflammatory responses. The end-result is often hepatic fibrosis.

25
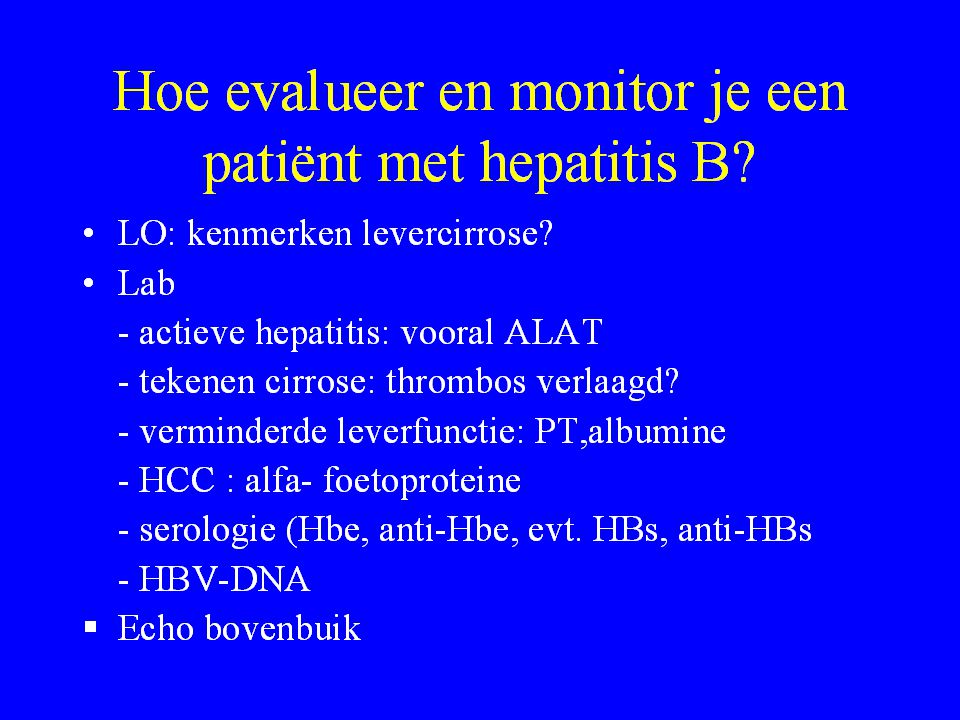
Laboratorium-afwijkingen
Hoe kan ik deze interpreteren?

26
het volledig bloedbeeld
Hb, leucos, thrombocyten- thrombocytopenie en leucopenie kan een uiting zijn van levercirrhose door verhoogde afbraak bij vergrote milt , maar thrombopenie kan ook HIV-gerelateerd zijn!

27
ASAT, ALAT ALAT hoger dan ASAT: past bij hepatitis B en C
ASAT hoger dan ALAT: levercirrhose ? Bij alhoholische hepatitis vooral hoge y-GT en ASAT Bij vele andere leveraandoeningen geen duidelijk patroon

28
Cholestatische hepatitis
Vooral Y-GT en alkalische fosfatase, evt. ook bilirubine verhoogd Tgv geneesmiddelen, alcohol Specifieke lever- en galwegsaandoeningen

29
Alkalische fosfatase Als uitsluitend alkalische fosfatase verhoogd is en alle andere leverenzymen normaal zijn: zeer waarschijnlijk botprobleem (of darmprobleem)
")
30
Verhoogd Bilirubine Aangeboren syndroom van Gilbert (wisselnde indirect bilirubine verhoging (bij voorkeeur geen atazanavir geven!) Bij acute hepatitis, levercelverval Bij voortgeschreden leverziekte, leverfalen Vaak ook aspecifieke lichte verhoging bij diverse aandoeningen Verschil:direct/indirect, voorbeeld: bij hemolyse vooral indirect door bloedafbraak

31
Alfa foetoproteine Marker voor HCC- hepatocellulair carcinoom
HCC = complicatie van hepatitis B en C als > 200 = zeer verdacht voor HCC, echter: normale waarde sluit HCC niet uit Vaak om de 6 maanden bepaald bij bestaande levercirrhose Alleen zinvol in combinatie met echo bovenbuik/lever controle

32
Leverfunctie testen als maat voor verminderde functie
Strikt genomen zegt alleen prothrombinetijd (PTT), albumine en bilirubine iets over de echte functie van de lever! Abnormaal PTT: > 2 seconden verlengd Abnormaal albumine: indien duidelijk verlaagd zoals <30 of zelfs < 20 Bilirubine: indien duidelijk verhoogd
, albumine en bilirubine iets over de echte functie van de lever! Abnormaal PTT: > 2 seconden verlengd. Abnormaal albumine: indien duidelijk verlaagd zoals <30 of zelfs < 20. Bilirubine: indien duidelijk verhoogd.")
33
Child Pugh Score A: 5-6, B:7-9, C: 10-15 Group A = 1 point
B = 2 points C = 3 points Serum bilirubin <35 35-50 >50 Serum albumin (g/dl) > 35 28-35 < 28 Prothrombin time 1-4 4-6 >6 Ascites None Easily controlled Poorly controlled Encephalopathy Grade 1-2 Grade 3-4 A: 5-6, B:7-9, C: 10-15
 > < 28. Prothrombin time >6. Ascites. None. Easily controlled. Poorly controlled. Encephalopathy. Grade 1-2. Grade 3-4. A: 5-6, B:7-9, C:")
34
Beeldvorming bij leverziekte
Echo, CT, MRI, fibroscan

35
Echografie bovenbuik Lever grote (bij cirrose kleine lever), structuur (homogeen, echorijk, steatose-veel vet), oppervlakte glad of hobbelig (cirrose) Verdenking op HCC ? Portale flow – normaal of niet (past bij gedecompenseerde cirrhose) Vergrote milt ? Ascites ? Normale echo sluit cirrhose niet uit!
, structuur (homogeen, echorijk, steatose-veel vet), oppervlakte glad of hobbelig (cirrose) Verdenking op HCC Portale flow – normaal of niet (past bij gedecompenseerde cirrhose) Vergrote milt Ascites Normale echo sluit cirrhose niet uit!")
36
CT/MRI lever Verricht indien echografisch de lever niet is te beoordelen (voorbeeld adipositas++) Indien er verdenking op HCC bestaat
 Indien er verdenking op HCC bestaat.")
37
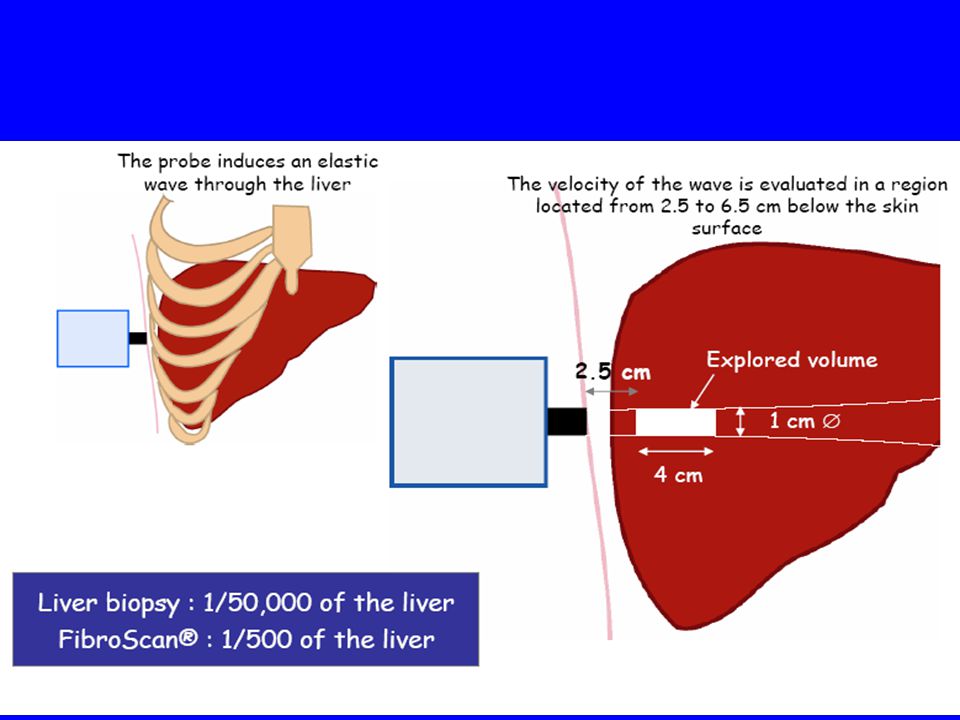
Transient elastography (Fibroscan®, Echosens, Paris)
")
39
Liver biopsy

40
Betrouwbaarheid van leverbiopt
Hangt direct af van lengte van biopt Het biopt moet minimaal 1.5 cm lang zijn, anders grote kans op onderschatting leverschade!

41
Length of liver biopsy Biopsy length
Liver biopsy is the gold standard for evaluating liver fibrosis but it has some limitations. A shown by bedossa et al using virtual biopsy from liver explants, a 25 mm long biopsy correctly staged in 75% of the cases and 40 mm were necessary to obtain a 100%reliability. Sampling variability of liver fibrosis in chronic hepatitis C Pierre Bedossa, M.D. 1 2 *, Delphine Dargère 2, Valerie Paradis 2 3 Biopsy length Bedossa, P. et al., (2003) Sapling variability of liver fibrosis in chronic hepatitis C. Hepatology
 Sapling variability of liver fibrosis in chronic hepatitis C. Hepatology")
42
Limitations of liver biopsy
Acceptability Cost £1000 per biopsy Morbidity Significant haemorrhage up to 0.7% Mortality up to 0.03% Reliability Length of biopsy Inter- and intra-observer variability Assumes uniform disease process

43
Beoordeling leverbiopt
Maat van ontsteking: graad 1-4 Maat van fibrose: graad 1-4, graad 4= cirrhose

44
Inflammatory Grading of Liver Biopsies
GRADE 1 <25% interface hepatitis GRADE 0 no inflammation GRADE 4 bridging necrosis GRADE 3 >75% interface hepatitis GRADE 2 25-75% interface hepatitis Inflammation involves three processes histologically: periportal or interface hepatitis, portal inflammation, and intralobular necrosis. This slide is an example of grading by interface hepatitis.

45
Fibrosis Staging of Liver Biopsies
no fibrosis portal fibrosis extraportal fibrosis Progression of fibrosis in viral hepatitis. Fibrosis normally starts in the portal tracts and extends outwards. This then progresses to bridging fibrosis (i.e. portal tracts linked by fibrous tissue) and extends inwards to involve central tracts resulting in nodule formation. Cirrhosis replacement of most of the liver by nodules. bridging fibrosis cirrhosis
 and extends inwards to involve central tracts resulting in nodule formation. Cirrhosis replacement of most of the liver by nodules. bridging fibrosis. cirrhosis.")
46
For patients with viral hepatitis, need to consider staging.
This graph illustrates serum aminotransferases do not always accurately predict the amount of liver damage as assessed by histology. This study by Shiffman et al in 95 hep C patients showed that in more than 1/3 of patients with persistently normal ALTs there was at least some degree of fibrosis, with 6% having cirrhosis. For patients with viral hepatitis, need to consider staging. Chronic infection with hepatitis C virus in patients with elevated or persistently normal serum alanine aminotransferase levels: comparison of hepatic histology and response to interferon therapy. Shiffman ML, Stewart CA, Hofmann CM, Contos MJ, Luketic VA, Sterling RK, Sanyal AJ. Shifman, M.L. et al., (2000) Chronic infection with hepatitis C virus in patients with elevated or persistently normal serum alanine aminotransferase levels: Comparison of hepatic histology and response to interferon therapy, The Journal of Infectious Diseases 182:
 Chronic infection with hepatitis C virus in patients with elevated or persistently normal serum alanine aminotransferase levels: Comparison of hepatic histology and response to interferon therapy, The Journal of Infectious Diseases 182:")
49
Invloed van HIV op natuurlijk beloop hepatitis C
HIV verhoogd HCV viraemie Kans op verticale transmissie en seksuele overdracht stijgt 5x hogere kans op ontstaan van levercirrhose binnen jaar (van 5% naar 25%) Toename ernst leverziekte: >40 jaar: 50% met ernstige fibrose/cirrhose HCC op jongere leeftijd
 Toename ernst leverziekte: >40 jaar: 50% met ernstige fibrose/cirrhose. HCC op jongere leeftijd.")
50
Progression to cirrhosis
1.00 4682 patients 0.83 180 HIV-HCV 701 Alcohol 812 HBV 382 Hemochromatosis 2313 HCV 93 Steatosis BMI>25 200 PBC 0.67 0.50 Hazard function 0.33 Fibrosis progression to cirrhosis varies by cause and population. This large retrospective analysis shows that in this cohort of over4500 patients progression to cirrhosis was fastest in HIV/HCV co-infected patients. Not only did progression vary by disease, but also there was acceleration of fibrosis progression by aging. Therefore, staging helps identify level of fibrosis and helps in prognosis and individual treatment decision-making in patients with HIV/HCV. 0.17 0.00 20 40 60 80 Age in years Poynard, T. et al., (2003) A comparison of fibrosis progression in chronic liver disease. Journal of Hepatology 38:
 A comparison of fibrosis progression in chronic liver disease. Journal of Hepatology 38:")
51
Cirrhosis has functional and structural consequences

52
Gevolgen van lever cirrhosis
SBP = spont bacteriele peritonitis, HRS= hep ren syndr

53
Acute hepatitis C bij HIV patiënten
sinds enkele jaren enorme toename onder homoseksuele mannen met hoog risicogedrag 20% kan spontaan genezen Meestal geen klachten! Verdenking ontstaat bij onverklaarde stijging ASAT/ALAT (vooral ALAT) Geen immuniteit na genezing! Diagnose: HCV RNA positief!, positieve antistoffen alleen geen bewijs (blijven levenslang positief ook na genezing)
 Geen immuniteit na genezing! Diagnose: HCV RNA positief!, positieve antistoffen alleen geen bewijs (blijven levenslang positief ook na genezing)")
54
Behandeling acute hepatitis C
In het algemeen iedereen behandelen rond week 12 (eerste 12 weken evt. spontane genezing afwachten) Peginterferon/ribavirine gedurende 24 weken, enkele centra behandelen alleen met Peginterferon Monitoren: vastleggen van genotype en HCV-RNA uitslagen!
 Peginterferon/ribavirine gedurende 24 weken, enkele centra behandelen alleen met Peginterferon. Monitoren: vastleggen van genotype en HCV-RNA uitslagen!")
55
Chronische hepatitis C bij HIV - patiënten
Hoelang bestaat de infectie al- wanneer voor het eerst vastgesteld? Hoe opgelopen? Genotype? Hoogte HCV-RNA? Beeldvorming-echo- verricht – uitslag? Leverbiopt verricht, uitslag? Eerdere behandeling? Falen tijdens therapie of relapse (terugkomen van infectie 24 of 48 weken na behandeling? Hepatitis B status? Antistoffen hepatitis A?

56
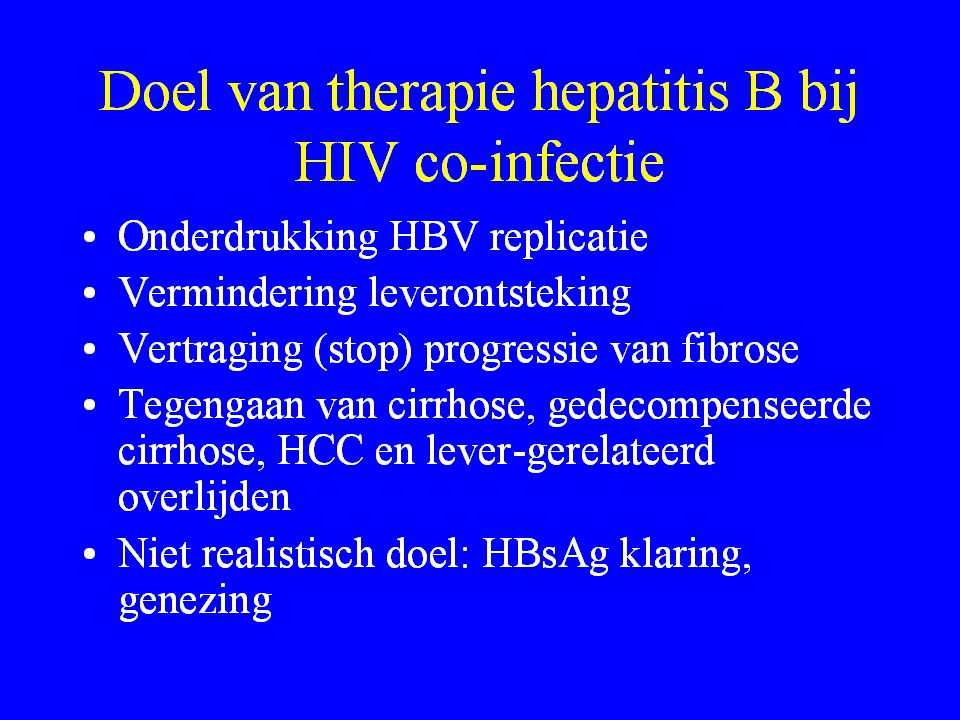
Behandeling chronische hepatitis C bij HIV
Alle patiënten met chronische hepatitis C komen in aanmerking voor behandeling! Genotype 2,3 beter te behandelen dan genotype 1,4 Ook bij levercirrhose behandeling mogelijk! Duur: weken Peginterferon/ribavirine (in toekomst ook protease remmers voor HCV!) Lab bijwerkingen: verlaging HB, leucos, thrombos, ontregeling schildklierfunctie (TSH/fT4), .. Evt. toevoeging psychiatrische medicatie
 Lab bijwerkingen: verlaging HB, leucos, thrombos, ontregeling schildklierfunctie (TSH/fT4), .. Evt. toevoeging psychiatrische medicatie.")
63
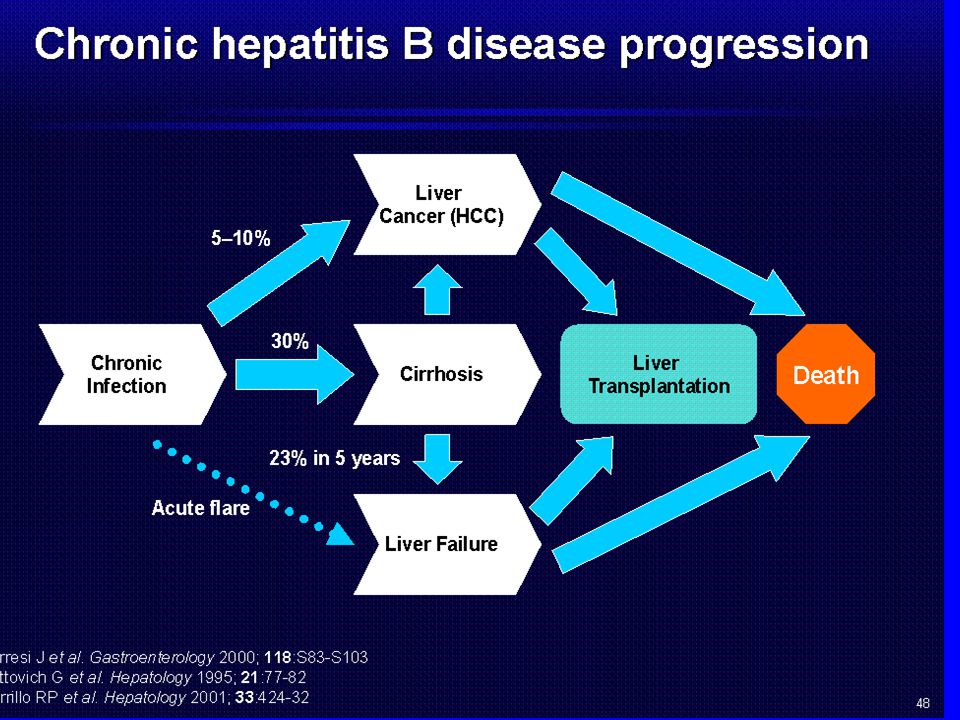
Progression to Cirrhosis and HBVDNA
Taiwan n=3851 Iloeje, gastroen.2006

68
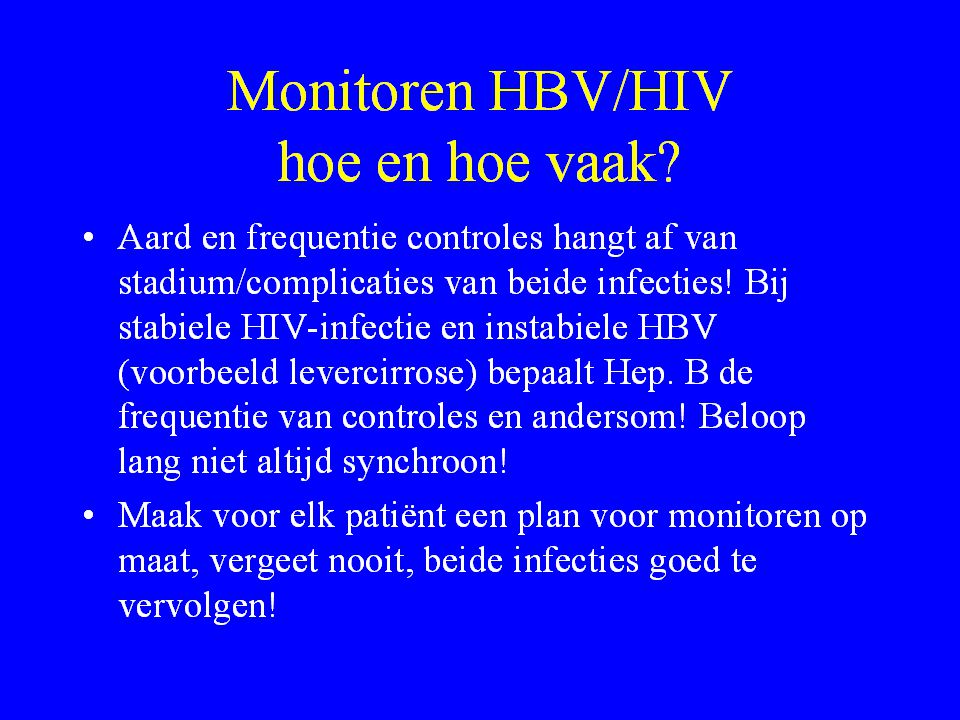
Het monitoren van leverproblemen bij HIV
Vele oorzaken voor leverafwijking, lang niet altijd is duidelijk, waardoor een leverafwijking wordt veroorzaakt, soms meerdere oorzaken! Zo goed mogelijk vastleggen van leverproblematiek bij HIV wel van essentieel belang

Verwante presentaties




>")


 bij ROW>")




>")




 overgewicht.>")



 Afvoer bloed Afvoer>")