Download de presentatie
De presentatie wordt gedownload. Even geduld aub

1
Haematologische problemen bij de bejaarde
D.Selleslag Haematologie AZ Sint-Jan 18 december 2008

2
Anemie bij de bejaarde Haematologische maligniteiten Myelodysplasie en AML CLL en CML NHL Plasmacelaandoeningen (Myeloproliferatieve ziekten)
")
4
Prevalentie van anemie bij ambulante bejaarde
Prevalentie van anemie vgls WHO criteria: Hgb < 13 g/dl (man) en Hgb < 12 g/dl (vrouw) Bron: NHANES III = 3rd US National Health and Nutrition Examination Survey Populatie: ambulante personen
 en Hgb < 12 g/dl (vrouw) Bron: NHANES III = 3rd US National Health and Nutrition Examination Survey. Populatie: ambulante personen.")
5
Distribution of hemoglobin in persons > 65 years according to sex
Guralnik, J. M. et al. Blood 2004;104:

6
Anemie bij bejaarde impact op mortaliteit
Hgb < (M) Hgb < (V) Populatie: 5888 , > 65 jaar FU prospectief ged 11.2 jr Bron: Cardiovascular Health Study , Arch Int Med 2005
 Hgb < 12.6 (V) Populatie: 5888 , > 65 jaar. FU prospectief ged 11.2 jr. Bron: Cardiovascular Health Study , Arch Int Med")
7
Andere effecten van anemie bij bejaarde
Hogere mortaliteit bij hartfalen Verminderde mobiliteit Meer vallen Meer cognitief verval Meer depressie Meer hospitalisatie Meer delirium Prospectieve interventionele studies ontbreken …

8
Oorzaken van anemie bij personen > 65 jaar
Type anemie Percentage Bloedverlies +/- Nutritionele deficientie 34 % Ijzer B12 en/of foliumzuur 20 % 14 % Chronische ziekte 32 % Chronische nierziekte ACD Combinatie 8 % 4 % Onuitgelegde anemie Hoog MCV (MDS ?) 5 % Bron: NHANES III, 2096 personen > 65 jr
 5 % Bron: NHANES III, 2096 personen > 65 jr.")
9
Anemia of “aging” ? Mogelijke mechanismen
Ontregeling van inflammatoire respons Langdurige verhoging van inflammatoire cytokines Afgezwakte hypoxie – EPO sensor in nieren Relatieve EPO deficientie Sarcopenie Stamceluitputting Beenmergcellulariteit daalt met leeftijd Verminderde produktie van geslachtshormonen Polyfarmacie Vele medicaties onderdukken bloedaanmaak

10
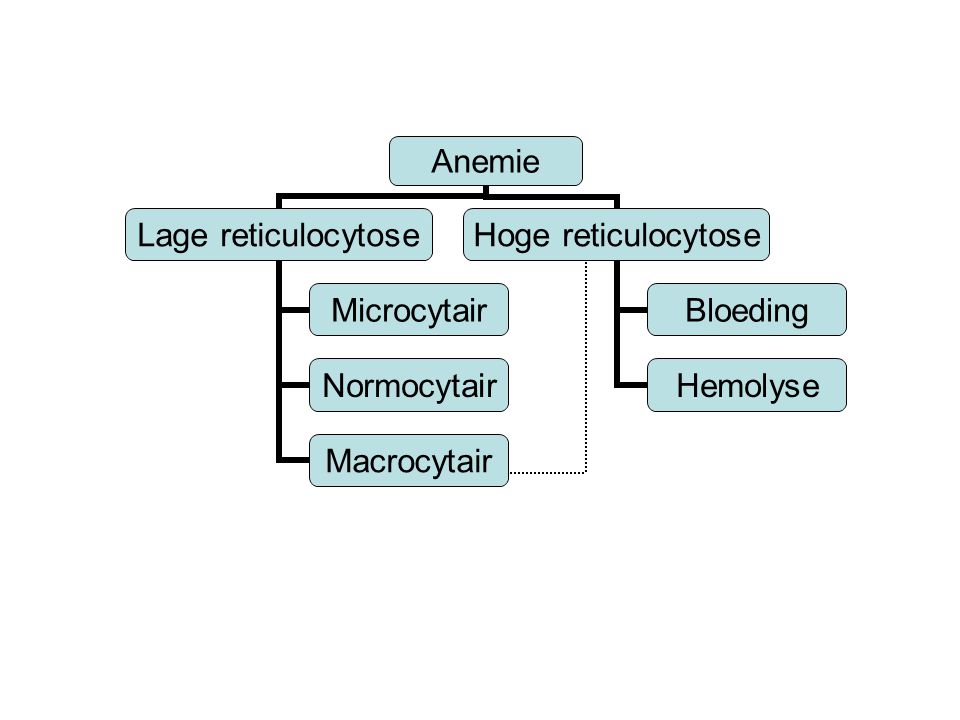
anemie: indeling morfologie kinetiek - uitstrijkje reticulocytose
- RBC indices: MCV macrocytair microcytair normocytair < 0.5 % > 1.5 % > 100 fl < 80 fl fl < > /mm3 Absolute reticulocytose : aantal RBC x % reticulocyten Gecorrigeerde reticulocytose: aantal reticulocyten x Hct / 45

12
Microcytaire anemie saturatie laag saturatie normaal/hoog
ferritine laag ferritine normaal/hoog ijzergebreks anemie van thalassemie sideroblastische anemie chronische ziekte hemoglobino- anemie (ACD) pathie fout in ijzer fout in globine- fout in haem- inbouw synthese synthese
 pathie. fout in ijzer- fout in globine- fout in haem- inbouw synthese synthese.")
13
Normaal ijzer ijzerdeficiente ferriprieve
depletie erythropoiese anemie ijzerdepots ijzer in RBC Serum ferritine /-60 (ng/ml) Serumijzer 115 +/ nl (mg/ 100 ml) Saturatie (%) 35 +/ nl RBC nl nl nl MCV, MCH Hb (g%) nl nl MCV, MCH
 Serumijzer 115 +/- 50 nl. (mg/ 100 ml) Saturatie (%) 35 +/- 15 nl. RBC nl nl nl MCV, MCH. Hb (g%) nl nl. MCV, MCH.")
14
Ferriprieve anemie bij bejaarde : oorzaken
Verlies: gastrointestinaal maag-of colonca hernia diafragmatica angiodysplasie - CT enteroclysma dubbel ballon enteroscopie Malabsorptie: Glutenenteropathie: antiweefsel transglutaminase Achlorhydrie : gastrine Atrofische gastritis Helicobacter pylori

15
Ijzersubstitutie buiten maaltijd (1/2 uur voor) indien mogelijk
geen antacida, geen thee geen slow release preparaat Fe2+ , met vitamine C dosis: in begin mg ijzer in 2-3 x nadien mg in 1x respons: reticulocytose na 3-5 dagen max na 8-10 dagen Hb + 2 g/dl na 3 weken duur: na correctie Hb nog 3-6 maand, + 1 g ijzer tot ferritine 50 mg/l zo geen respons: Venofer IV (ijzersaccharaat/sucrose)
")
16
Ijzerpreparaten Naam Samenstelling Resorptie Elementair ijzer / tabl
Losferron ijzergluconaat, vit C > 10% 80 mg Ferograd 500 ijzersulfaat,vit C > 10% 105 mg Ferogradumet ijzersulfaat 10 % 105 mg Fer-in-sol ijzersulfaat 10 % 25 mg/ml Ferumat ijzerfumaraat < 10% 6.5 mg/ml Ferricure ijzerpolysaccharaat < 1% 150 mg Fe3+

17
Microcytaire anemie saturatie laag saturatie normaal/hoog
ferritine laag ferritine normaal/hoog ijzergebreks anemie van thalassemie sideroblastische anemie chronische ziekte hemoglobino- anemie (ACD) pathie fout in ijzer fout in globine- fout in haem- inbouw synthese synthese
 pathie. fout in ijzer- fout in globine- fout in haem- inbouw synthese synthese.")
18
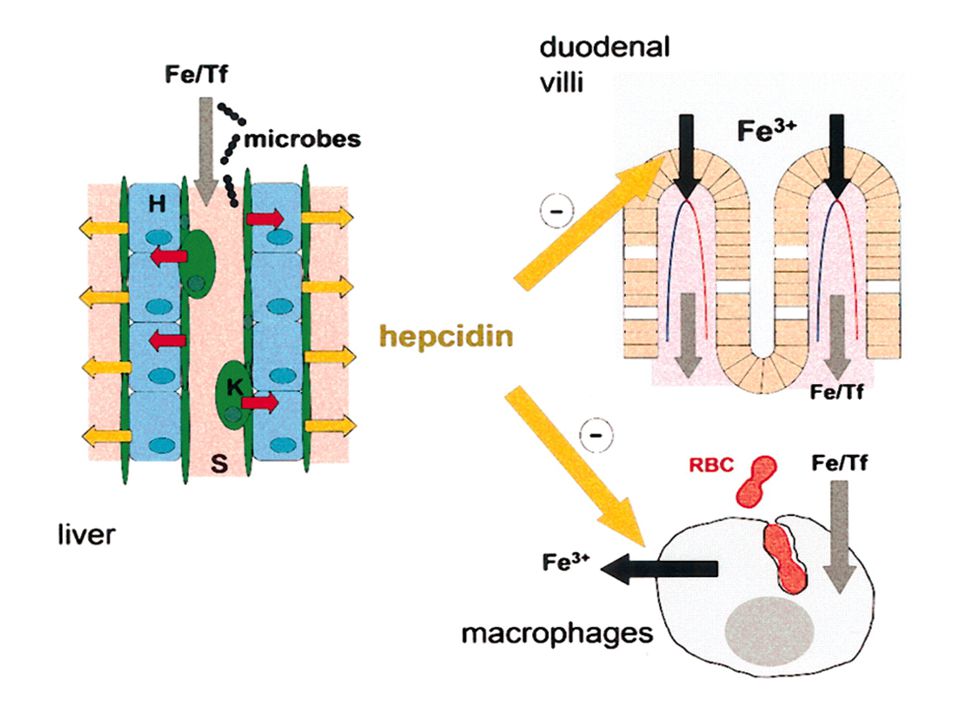
Anemia of chronic disease
Chronische inflammatie Tumoren Cytokine vrijzetting (IL1, TNF) EPO productie daalt Minder vrijzetting van ijzer uit RES Minder absorptie van ijzer in darm Anemie Hepcidine
 EPO productie daalt. Minder vrijzetting van ijzer uit RES. Minder absorptie van ijzer in darm. Anemie. Hepcidine.")
20
Normocytaire anemie saturatie laag normaal
begin ijzertekort endocrien: bijnier sec anemie (ACD) schildklier nier lever beenmerg: invasie fibrose aplasie Meestal beenmerg/botbiopt nodig
 schildklier. nier. lever. beenmerg: invasie. fibrose. aplasie. Meestal beenmerg/botbiopt nodig.")
21
Macrocytaire anemie Megaloblastaire Niet-megaloblastaire
vit B myelodysplasie lever foliumzuur alkohol medicatie hypothyroidie COPD dosage B12, FZ bloedbeeld bloedbeeld beenmerg soms enkel beenmerg chromosomen hoog MCV LDH valse macrocytose: koude agglutinatie, hyperglycemie reticulocytose

22
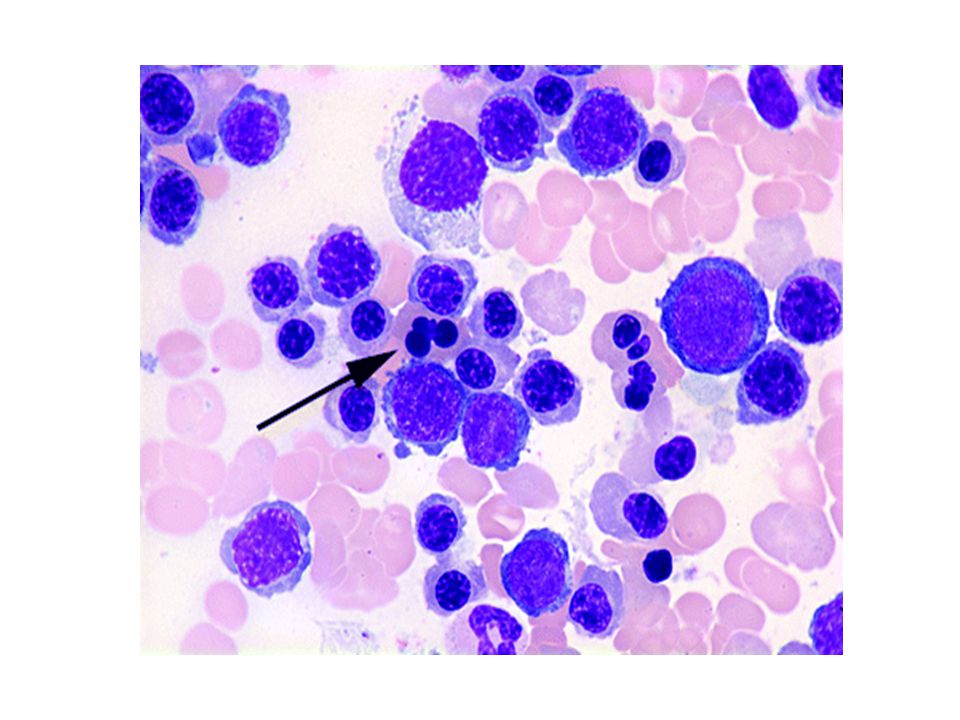
Megaloblastaire anemie

23
Megaloblastaire anemie
Vitamine B12 tekort Foliumzuur tekort nood: 5 mg/d nood: 400 mg/d voorraad: 3-5 jaar voorraad: 3 maand achterstrengsyndroom geen neurologische stoornissen - (dieet: vegetariers) - dieet, alkoholisme - malabsorptie: - malabsorptie: (HP) gastritis perniciosa gluten-enteropathie gastrectomie dundarmziekten Crohn, blind loop anticonvulsiva pancreasinsufficientie (fenytoine) - antagonist: N2O - verhoogde nood (zwangerschap, DD: anti - IF 60% hemolyse, tumoren, psoriasis) Schillingtest - antagonisten: MTX, trimethoprim
 - dieet, alkoholisme. - malabsorptie: - malabsorptie: (HP) gastritis. perniciosa gluten-enteropathie gastrectomie dundarmziekten. Crohn, blind loop anticonvulsiva. pancreasinsufficientie (fenytoine) - antagonist: N2O - verhoogde nood (zwangerschap, DD: anti - IF 60% + hemolyse, tumoren, psoriasis) Schillingtest - antagonisten: MTX, trimethoprim.")
24
Oorzaak van vit B12 deficientie ? Schilling test
Correctie met IF Geen correctie met IF Oorzaak van vit B12 deficientie ? Schilling test

25
Niet iedere verlaging van B12 is klinisch belangrijk
Vaak valse verlaging B12 zonder anemie Belang van MCV en hypersegmentatie Weefselspiegel B12 ~ Meting van homocysteine ? Behandeling: Begin: onafhankelijk vd oorzaak Vit B12 1 mg IM 1 x per week (8 X) , dan 1 X per maand Vit B12 oraal 1 mg alle dagen Onderhoud: afhankelijk vd oorzaak
 , dan 1 X per maand. Vit B12 oraal 1 mg alle dagen. Onderhoud: afhankelijk vd oorzaak.")
26
Macrocytaire anemie Megaloblastaire Niet-megaloblastaire
vit B myelodysplasie lever foliumzuur alkohol medicatie hypothyroidie COPD dosage B12, FZ bloedbeeld bloedbeeld beenmerg soms enkel beenmerg chromosomen hoog MCV LDH valse macrocytose: koude agglutinatie, hyperglycemie reticulocytose

27
Myelodysplasie (MDS) ziekte van de pluripotente stamcel
beenmerg: uitrijpingsstoornis (dysplasie) blastenexces perifeer bloed: (pan)cytopenie hoog MCV, soms geisoleerd evolutie naar acute myeloiede leukemie chromosoomafwijkingen prognose: zeer variabel: laag >< hoog risico behandeling: supportief >< stamceltransplant
 blastenexces. perifeer bloed: (pan)cytopenie. hoog MCV, soms geisoleerd. evolutie naar acute myeloiede leukemie. chromosoomafwijkingen. prognose: zeer variabel: laag >< hoog risico. behandeling: supportief >< stamceltransplant.")
29
Incidence of MDS Increases with Age
2 1 4 9 16 26 52 59 61 10 20 30 40 50 60 70 30- 35- 40- 45- 50- 55- 60- 65- 70- 75- 80- 80 90 80+ 89 Age-specific incidence rates (per 100,000) Less than 80 and over 89 The disease becomes more common as we grow older. On this slide you can see that over the age of 70 the incidence of the disease increases markedly. In patients who are less than 50 years old the overall incidence is 0.5 per 100,000 of the population, whereas for patients over the age of 70 the overall incidence is nearly 50 cases per 100,000 of the population, rising to approximately 90 cases per 100,000 of the population over the age of 80. Age (years) Adapted from Williamson PJ, et al. Br J Haematol :743–5.
 Less than and over 89. The disease becomes more common as we grow older. On this slide you can see that over the age of 70 the incidence of the disease increases markedly. In patients who are less than 50 years old the overall incidence is 0.5 per 100,000 of the population, whereas for patients over the age of 70 the overall incidence is nearly 50 cases per 100,000 of the population, rising to approximately 90 cases per 100,000 of the population over the age of 80. Age (years) Adapted from Williamson PJ, et al. Br J Haematol :743–5.")
30
MDS: natural history % blasts MDS clone time

31
Survival time (months)
WHO Classification Survival RA/RARS RCMD/RCMD-RS RAEB-1 RAEB-2 AML 1.0 0.9 0.8 0.7 0.6 Cumulative proportion surviving 0.5 0.4 0.3 Just like the FAB classification, the prognostic value of the WHO classification has also been confirmed, as is shown in this slide. Patients with refractory anaemia, and refractory anaemia with ringed sideroblasts have a better survival than patients with refractory anaemia with excess blasts. 0.2 0.1 Survival time (months) From Malcovati L, et al. J Clin Oncol :7594–603.
 From Malcovati L, et al. J Clin Oncol :7594–603.")
32
Survival and AML Progression IPSS MDS Risk Classification
Score : % blasten, cytopenie, karyotype Low 267 pts Int-1 314 pts Int-2 179 pts High 56 pts 100 90 80 70 60 50 40 30 20 10 A 1 2 3 4 5 6 7 8 9 11 12 13 14 15 16 17 18 years percent Survival B AML Evolution 100 90 80 70 60 50 40 30 20 10 Low 235 pts Int-1 295 pts Int-2 171 pts High 58 pts percent The overall survival as well as evolution to acute myeloid leukaemia and the time it takes for the acute myeloid leukaemia to develop is very different between the IPSS subgroups, as is shown on this slide. On the left-hand side, the survival of patients is clearly shown to be better in subgroups with low-risk IPSS scores, in marked contrast to those who are in the high-risk IPSS score. Similarly, the evolution to AML in the high-risk category is extremely high compared to those with low-risk IPSS scores. 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 years From Greenberg P, et al. Blood :2079–88. Copyright American Society of Hematology, used with permission.

33
Low / int 1 risk MDS Int 2 / high risk MDS Verbetering overleving
Vertraging evolutie naar AML Verbetering van QOL en van cytopenia AlloSCT Intensive chemotherapy Hypomethylerende Agentia Thalidomide Lenalidomide ATG, CsA Epo / GCSF TPO receptor agonists Supportive care Treatment intensity Oral iron chelators

34
Park S et al, Blood, Oct 2007 (E-pub)
French EPO cohort P < IPSS/IMRAW Park S et al, Blood, Oct 2007 (E-pub)
")
35
Transfusion

37
Survival disadvantage for transfusion-dependent MDS patients

38
Deferasirox: Exjade Tridentate* iron chelator Oral, dispersible tablet
Oral biovalailability 70 % Administered once daily Half life 8-16 hrs Chelated iron excreted mainly in feces (<10% in urine) Starting dose 20 mg/kg on empty stomach Well tolerated O OH HO N Fe * Deferasirox is a novel, orally active tridentate iron chelator with a high affinity and specificity for iron *3 polar interaction sites in the binding pocket
 Starting dose 20 mg/kg on empty stomach. Well tolerated. O. OH. HO. N. Fe. * Deferasirox is a novel, orally active tridentate iron chelator with a high affinity and specificity for iron. *3 polar interaction sites in the binding pocket.")
39
Iron Chelation Therapy and Survival in MDS
170 transfusion dependent MDS patients included during a 1 month period in 2005, prospectively followed and reanalyzed 2 yrs later 1.00 Median survival: 63 months (whole group) 115 vs 51 months (P < .0001) 0.75 Survival Distribution Function 0.50 Chelation 0.25 No chelation CT, chelation therapy; IPSS, International Prognostic Scoring System; OS, overall survival Permission to use these graphics provided courtesy of Christian Rose, MD, and on behalf of Groupe Francophone des Myélodysplasies 0.00 50 100 150 200 250 Diagnosis to Death Time (Mos) Rose C, et al. ASH Abstract 249.
 115 vs 51 months (P < .0001) Survival Distribution Function Chelation No chelation. CT, chelation therapy; IPSS, International Prognostic Scoring System; OS, overall survival. Permission to use these graphics provided courtesy of Christian Rose, MD, and on behalf of Groupe Francophone des Myélodysplasies Diagnosis to Death Time (Mos) Rose C, et al. ASH Abstract 249.")
40
Low / int 1 risk MDS Int 2 / high risk MDS Verbetering overleving
Vertraging evolutie naar AML Verbetering van QOL en van cytopenia AlloSCT Intensive chemotherapy Hypomethylerende Agentia Thalidomide Lenalidomide ATG, CsA Epo / GCSF TPO receptor agonists Supportive care Treatment intensity Oral iron chelators

41
Hypermethylation and Silencing
Normal M M M Expressed DNA methyl transferase Methyltransferase inhibitors This slides shows the involvement of DNA methylation in gene silencing. Cytosine bases in regulatory areas of genes are normally free of methylation (shown in white on the top graph). Rarely, these sites become hypermethylated (bottom) and this leads to gene silencing. This switch, which is physiologically irreversible, occurs on the inactive X-chromosome in women and is frequent in cancer where it affects tumor-suppressor genes. M M M M M M M M M Cancer Silencing of regulatory genes (e.g. tumor suppressor genes) Courtesy of Issa, JP
. Rarely, these sites become hypermethylated (bottom) and this leads to gene silencing. This switch, which is physiologically irreversible, occurs on the inactive X-chromosome in women and is frequent in cancer where it affects tumor-suppressor genes. M. M. M. M. M. M. M. M. M. Cancer. Silencing of regulatory genes. (e.g. tumor suppressor genes) Courtesy of Issa, JP.")
42
Hypomethylating Cytosine Analogs
NH2 NH2 NH2 NH2 CH3 N N N N N N N O N O N O N O Ribose Deoxyribose Cytosine 5-methyl-cytosine 5-aza-cytidine 5-aza-2’-deoxycytidine The cytidine analogs modified in position 5 of the pyrimidine ring are potent inhibitors of DNA methylation. The 5 carbon of the pyrimidine ring has been replaced by a nitrogen in these compounds. Cytidine agents such as ara-C, which do not possess this change in the pyrimidine ring, do not inhibit methylation. These analogs include 5-aza-cytidine (azacitidine) and azacitidine-2’-deoxycytidine (decitabine). (azacitidine) (decitabine) Vidaza Dacogen (Celgene) (J&J) Santini V, et al. Ann Intern Med. 2001;134(7): FDA approved
 and azacitidine-2’-deoxycytidine (decitabine). (azacitidine) (decitabine) Vidaza Dacogen. (Celgene) (J&J) Santini V, et al. Ann Intern Med. 2001;134(7): FDA approved.")
43
Vidaza (5 azacitidine) is enige medicatie die overleving van hoog risico MDS verlengt
9.4 months

44
EORTC-LG (and HOVON* or GIMEMA**) Survival in AML trials (age > 60)
100 90 Betere supportieve therapie 80 70 60 50 AML-13** ( ) 40 30 AML-11* ( ) 20 AML-7 ( ) AML-9 ( ) 10 (years) 1 2 3 4 5 6 7 8 9
 AML-11* ( ) 20. AML-7. ( ) AML-9 ( ) 10. (years)")
45
Intensieve inductie versus palliatieve therapie bij oudere AML
Intensieve chemotherapie Palliatieve therapie Complete remissie 58 % 0 % Vroege dood 3/31 18/29 Mediane overleving 21 weken 11 weken Overleving na 2,5 jaar 17 % Dagen in ziekenhuis 55 % 50 % Lowenberg et al, JCO, 1989 ; 7, 1268

46
Rol van Minitransplantatie bij AMLin CR1 :
Donor vs geen donor Transplant vs Geen transplant Mohty et al, Leukemia, 2005, 19, 916

47
Philadelphia chromosoom
CD5 + monoclonale B celpopulatie Chronische myeloiede leukemie Chronische lymfatische leukemie

48
The Ph Chromosome and the bcr-abl Gene
9 q+ 9 Ph (or 22q-) Imatinib 22 bcr bcr-abl abl FUSION PROTEIN WITH TYROSINE KINASE ACTIVITY t(9;22) translocation
 Imatinib. 22. bcr. bcr-abl. abl. FUSION PROTEIN WITH TYROSINE KINASE ACTIVITY. t(9;22) translocation.")
49
Behandeling CML CLL Tyrosine kinase inhibitor
Imatinib (glivec) Dasatininb (sprycel) Nilotinib (Tasigna) Allogene stamceltransplantatie Wanneer behandelen ? Altijd Therapie vertraagt evolutie naar blastencrisis
 Dasatininb (sprycel) Nilotinib (Tasigna) Allogene stamceltransplantatie. Wanneer behandelen Altijd. Therapie vertraagt evolutie naar blastencrisis.")
50
Behandeling van CML imatinib transplant hydroxyurea of IFN
IBMTR-German CML Study Group Comparative study Gale et al, Blood, 1998, 91, 1810

51
Behandeling CML CLL Tyrosine kinase inhibitor
Imatinib (glivec) Dasatininb (sprycel) Nilotinib (Tasigna) Allogene stamceltransplantatie Wanneer behandelen ? Altijd Therapie vertraagt evolutie naar blastencrisis Afwachten Chlorambucil = Leukeran Fludarabine Wanneer behandelen ? Verdubbeling WBC < 6 md Anemie, trombopenie Adenopathieen Splenomegalie Constitutionele klachten Therapie in beginstadium verbetert NIET prognose
 Dasatininb (sprycel) Nilotinib (Tasigna) Allogene stamceltransplantatie. Wanneer behandelen Altijd. Therapie vertraagt evolutie naar blastencrisis. Afwachten. Chlorambucil = Leukeran. Fludarabine. Wanneer behandelen Verdubbeling WBC < 6 md. Anemie, trombopenie. Adenopathieen. Splenomegalie. Constitutionele klachten. Therapie in beginstadium verbetert NIET prognose.")
52
Overall Survival in the First Trial
Dighiero, G. et al. N Engl J Med 1998;338:

53
Overall Survival According to Treatment Group
Figure 3. Overall Survival According to Treatment Group. Shown are the proportions of 178 patients assigned to fludarabine, 193 assigned to chlorambucil, and 136 assigned to fludarabine plus chlorambucil who were still alive during follow-up. Forty-seven percent, 57 percent, and 56 percent of the patients in the three groups, respectively, died. There was no statistically significant difference in overall survival among the three groups (median, 66 months, 56 months, and 55 months, respectively; P=0.21). Rai K et al. N Engl J Med 2000;343:
. Rai K et al. N Engl J Med 2000;343:")
54
Non-Hodgkin lymfoma Laaggradig of indolent Hooggradig of aggressief
Niet curabel Frequente recidieven Therapie Wait and see Radiotherapie Leukeran Rituximab + chemotherapie Stamceltransplantatie autoloog of allogeen Curabel Genezingskans > 50 % Standaardtherapie: Ritiximab + CHOP om 14 of 21 dagen 6-8 cycli

55
Specific binding to CD20: Mode of action
binding region Malignant B cell MabThera Killer cell Complement Adapted from: Male et al. Adv Immunol 1996 Depletion of B-cells NHL: 85% pre-B and B-cells MabThera does not affect other cell types

56
CHOP vs R-CHOP in DLBCL 60-80 years Event-free survival: 4-year update
1.0 0.8 0.6 51% MabThera + CHOP Probability of event-free survival 0.4 0.2 29% CHOP p= Years Coiffier et al 2004.

57
CHOP vs R-CHOP in DLBCL 60-80 years Overall survival: 4-year update
1.0 0.8 0.6 0.4 0.2 59% MabThera + CHOP P=0.01 Probability of overall survival 47% CHOP Years Coiffier et al.2004

58
Plasmacel aandoeningen
MGUS SLUIMEREND MYELOOM MULTIPEL MYELOOM PLASMACEL LEUKEMIE

59
Myeloma: definities (WHO)
MGUS Smouldering Myeloma Multipel myeloma Plasmacellen In beenmerg < 10 % Geen aggregaten 10-30 % > 10 % M component IgG < 3.5 g/dl IgA < 2.0 g/dl LC urine < 1 g IgG > 3.5 g/dl IgA > 2 g/dl LC > 1 g Myeloma-related orgaan dysfunctie afwezig 1 of meer Calcium Renal Anemia Bone lesions Therapie geen ja

60
MGUS Voorkomen: < 50 jaar: 0.2 % > 50 jaar: 1 %
IgG of IgA > myeloma IgM > laaggradig B-cel lymfoma ziekte van Waldenstrom

61
Initiele onderzoeken bij monoclonale gammopathie
complet, nierfunctie, calcium IgA - IgG – IgM serum: vrije lichte ketens urine 24 uur: eiwit, lichte ketens IgG of IgA: RX axiaal skelet en lange beenderen indien RX negatief: MRI wervelzuil niet : botscintigrafie of botdensitometrie IgM: echo abdomen Beenmergpunctie en botbiopsie

62
Evolutie van MGUS 1 % per jaar
Kyle R et al, N Engl J Med 2002, 346, 564

63
n = 1324 Gregersen et al, Br J Haematol, 2001, 112, 353

65
Risico van progressie van MGUS naar myeloom of verwante aandoening
Risicofactoren M piek > 1.5 g/dl IgA of IgM FLC ratio < 0.26 of > 1. 65 Rajkumar, S. V. et al. Blood 2005;106: Copyright ©2005 American Society of Hematology. Copyright restrictions may apply.

66
MGUS: follow-up Eerste jaar: IgA,G,M om de 3 maanden
Daarna : om de 6 maanden Beenmergpunctie om de 1 tot 2 jaar RX skelet bij progressie

68
Osteoporose of indeukingsfracuren
Op eender welke leeftijd Electroforese en lichte ketens op serum Bence Jones of lichte ketens op urine Myeloom en vooral Lichte ketenziekte is vaak gemiste diagnose

69
Period estimates of 10-year survival of patients with MM by major age groups in defined calendar periods from 1984–1986 to 2002–2004 10-year relative survival (%) 1984–1986 1987–1989 1990–1992 1993–1995 1996–1998 1999–2001 2002–2004 5 10 15 20 25 30 35 40 45 50 Calendar period <50 50–59 60–69 70–79 80+ Brenner et al. Blood 2008;111:2521–26
 1984– – – – – – – Calendar period. <50. 50–59. 60–69. 70– Brenner et al. Blood 2008;111:2521–26.")
70
Nieuwe medicatie voor myeloma
Thalidomide Bortezomib Lenalidomide Handels naam Velcade Revlimid Groep Imid Proteasoominhibitor Werking Plasmacellen en beenmerg microenvironment Neven werkingen DVT PNP Constipatie Sedatie Diarrhee Trombopenie Myelosuppressie Terugbetaling Eerste lijn Tweede lijn Derde lijn

71
Palumbo, A. et al. Blood 2008;112:3107-3114
Melphalan-Prednisone +/- Thalidomide eerste lijn bij MM jaar Palumbo, A. et al. Blood 2008;112:

72
Melphalan-prednisone +/- Velcade in eerste lijn :VISTA trial
San Miguel, NEJM 2008; 359:906

73
Supportieve therapie Kyphoplastie IV immuunglobulines ESA
Bisfosfonaten om de 4 weken Zometa = zoledronaat Bewezen reductie van “skeletal events” Osteonecrose mandibula (ONJ) Kyphoplastie
 Kyphoplastie.")
74
ONJ : kaakbeen necrose (

75
ONJ : kaakbeen necrose

76
Ballonkyphoplastie

77
Myeloproliferatieve ziekten
Polycythemia vera (ziekte van Vaquez) Primaire trombocytose Primaire myelofibrose
 Primaire trombocytose. Primaire myelofibrose.")
78
Erythrocytose of polyglobulie
Hct > 0.56 (V) Hct > 0.60 (M) JAK2 mutatie In 90 % JAK2 mutatie afwezig
 Hct > 0.60 (M) JAK2 mutatie. In 90 % JAK2 mutatie. afwezig.")
79
Trombocytose JAK2 mutatie aanwezig bij 50 % JAK2 mutatie afwezig
Bloedplaatjes > PRIMAIRE TROMBOCYTOSE SECUNDAIRE Bloedverlies Ijzergebrek Infectie Inflammatie Tumor Trauma Chirurgie Splenectomie Trombose, arterieel of veneus Bloeding Vasomotorische symptomen: - Hoofdpijn - Erytromelalgie - Angor - Amaurosis fugax Ferritine CRP Trombocytose JAK2 mutatie aanwezig bij 50 % JAK2 mutatie afwezig

80
Kliniek: PV en ET Erythromelalgie Digitale ischemie

81
Wild type JAK2 * JAK2 V617F mutatie * *

82
JAK2 mutatie: implicaties voor diagnose en therapie
JAK2 mutatie bekend sinds 2005 Aanwezigheid van JAK2 mutatie is diagnostisch voor myeloproliferatieve ziekte en maakt bijkomende investigatie overbodig JAK2 positieve trombocytose en polycythemie worden beschouwd als één myeloproliferatieve aandoening JAK2 mutatie: target voor specifieke therapie ?

83
Polycythemia vera Primaire trombocytose Behandeling
Waarom: wegens verhoogde tromboseneiging Volgens CV risico, leeftijd, tromboseneiging Flebotomie Hct < 0.45 (M) < 0.40 (V) Hydroxyurea BP < 600 x 109/l Anagrelide Aspirine lage dosis
 < 0.40 (V) Hydroxyurea BP < 600 x 109/l. Anagrelide. Aspirine lage dosis.")
84
Cortelazzo et al, N Eng J Med, 1995

Verwante presentaties



>")





>")




 Quiz Night !>")






