Download de presentatie
De presentatie wordt gedownload. Even geduld aub

1
Critical Review FANC, mei 2009 Christophe de Brouwer, MD, MIH, PhD Ecole de Santé publique Université libre de Bruxelles http://www.ulb.ac.be/esp/lsttm

2
André Aurengo1 (Rapporteur), Dietrich Averbeck, André Bonnin (†), Bernard Le Guen, Roland Masse, Roger Monier, Maurice Tubiana (Chairman), Alain-Jacques Valleron, Florent de Vathaire. Dose-effect relationships and estimation of the carcinogenic effects of low doses of ionizing radiation. Académie des Sciences - Académie nationale de Médecine (Frankrijk). 30/3/2005 De lineaire veronderstelling zonder drempel in kwestie
. 30/3/2005 De lineaire veronderstelling zonder drempel in kwestie.")
3
Het antwoord van EPA Radiogenic cancer risk models and projections for the U.S. Population. Environmental Protection Agency (EPA). Draft. December 2008 (USA).
. Draft. December 2008 (USA)..")
4
Conclusie... ?

5
Wat is een lineair model zonder drempel ? Gevolgen Blootstelling EPA norm blootst = 10 -5 kankers 0 « Norm » = aantal gevolgen / blootstellingseenheid

6
Effective dosis Sv (physio-pathologishe eenheid) Som van [equivalente dosis per weefsel x weefselweegfactor Wt] Weefsel of orgaan Oud Wt Nieuwe Wt Geslachtsorgaan0,200,08 Beendermerg0,12idem Dikke darm0,12idem Long0,12idem Maag0,12idem Blaas0,50,04 Borsten0,050,12 Lever0,050,04 Slokdarm0,050,04 Schildklier0,050,04 Huid0,01idem Been opervlakte 0,01idem Hersenen0,01 Speekselklieren0,01 Anderen0,050,12
![Effective dosis Sv (physio-pathologishe eenheid) Som van [equivalente dosis per weefsel x weefselweegfactor Wt] Weefsel of orgaan Oud Wt Nieuwe Wt Geslachtsorgaan0,200,08 Beendermerg0,12idem Dikke darm0,12idem Long0,12idem Maag0,12idem Blaas0,50,04 Borsten0,050,12 Lever0,050,04 Slokdarm0,050,04 Schildklier0,050,04 Huid0,01idem Been opervlakte 0,01idem Hersenen0,01 Speekselklieren0,01 Anderen0,050,12](http://images.slideplayer.nl/8/2129880/slides/slide_6.jpg "Effective dosis Sv (physio-pathologishe eenheid) Som van [equivalente dosis per weefsel x weefselweegfactor Wt] Weefsel of orgaan Oud Wt Nieuwe Wt Geslachtsorgaan0,200,08 Beendermerg0,12idem Dikke darm0,12idem Long0,12idem Maag0,12idem Blaas0,50,04 Borsten0,050,12 Lever0,050,04 Slokdarm0,050,04 Schildklier0,050,04 Huid0,01idem Been opervlakte 0,01idem Hersenen0,01 Speekselklieren0,01 Anderen0,050,12")
7
De lineaire veronderstelling zonder drempel Collectieve dosis Collectieve dosis = M-Sv = som van individuele dosis Gevolgen Blootstelling Gevolgen Blootstelling Gevolgen Blootstelling Gevolgen Blootstelling + + + + + + Gevolgen Blootstelling

8
Totaal stochastisch risico (bijvoorbeeld het aantal verwachte kankers ) = Collective dosis (M-Sv) x schatting van het risico (aantal gevallen / Sv) ! Deze logica is niet aanvaardbaar door ICRP 103 ! De collectieve effectieve dosis wordt alleen gebruikt voor het optimaliseren.

9
Effectieve dosis en weegfactoren. De blootstelling (Bq & eV) De geabsorbeerde dosis (Gy) De equivalente dosis (Sv) : Stralingsweegfactor Wr De effectieve dosis (Sv) : weefselweegfactor Wt De collectieve dosis (M-Sv) De schatting van het bevolkingsrisico (kankers aantal,... / bevolking)
 De geabsorbeerde dosis (Gy) De equivalente dosis (Sv) : Stralingsweegfactor Wr De effectieve dosis (Sv) : weefselweegfactor Wt De collectieve dosis (M-Sv) De schatting van het bevolkingsrisico (kankers aantal,... / bevolking).")
10
De lineaire veronderstelling zonder drempel (NTLH) en het DDREF <0,2 Gy ? 1990 DDREF=2 DDREF=dose/dose rate effectiveness factor Dosis 0,2 Gy Gevolgen USA (1990) BEIR5: DDREF =1 behalve leukemia DDREF =4 « Norm x2 » = aant. gevolgen / blootst. eenheid ICRP 60 (1960)
 BEIR5: DDREF =1 behalve leukemia DDREF =4 « Norm x2 » = aant. gevolgen / blootst. eenheid ICRP 60 (1960).")
11
De lineaire veronderstelling zonder drempel (NTLH) en het DDREF <0,2 Gy... nu ( 2007 )? DDREF=2 DDREF=dose/dose rate effectiveness factor Dosis 0,2 Gy Gevolgen USA BEIR7 (2006): DDREF =1,5 ICRP 103 (2007)
. DDREF=2 DDREF=dose/dose rate effectiveness factor Dosis 0,2 Gy Gevolgen USA BEIR7 (2006): DDREF =1,5 ICRP 103 (2007).")
12
ICRP 60 ICRP 103 ICRP 60 ICRP 103 ICRP 60 ICRP103 5,64,20,80,14,84,1 Volwassenen 7,35,71,30,26,05,5 Iedereen TotaalHerediteitKanker Blootgestelde bevolking Nominaal risico : 10 -2 Sv -1 of 10 000 man-Sv Absoluut (of additief) model …. ? Bron BEIR (1972) 1,17 - 6,2 UNSCEAR (1977) 0,7 - 1,7 ICRP (1977) 1,25 BEIR (1980) 1,5 - 5 Charles et al. (1983) 1,0 - 4,4 Preston + Pearce (1987) 5,8 - 18 UNSCEAR (1988) 4,2 - 11 BEIR V (1990) 5,4 – 12,4 Nussbaum + Köhnlein (1990) 25
 1,17 - 6,2 UNSCEAR (1977) 0,7 - 1,7 ICRP (1977) 1,25 BEIR (1980) 1,5 - 5 Charles et al. (1983) 1,0 - 4,4 Preston + Pearce (1987) 5, UNSCEAR (1988) 4, BEIR V (1990) 5,4 – 12,4 Nussbaum + Köhnlein (1990) 25.")
13
Welke realiteit? Ten nadele van...

14
Momenteel geobserveerd « drempels » : 200 mSv: niet betwist 20 mSv: RERF (Brenner et al, 2003) 10 mSv: In utero blootstelling (Stewart et al, 1952) en bepaalde waarnemingen van leukemie-risico bij kernenergie werknemers (Wilkinson et al, 1991). 1,5 mSv/jaar : Radon blottstellingsgemiddelde: veronderstelling van 10% longkankers en verenigbaarheid met NTLH ? ? 0,1 à 0,2 mSv /jaar : gevolgen van Chernobyl op Berlijn en Schotland ( Down syndroom ) of Beieren (perinataal sterftecijfer)... Heeft het onderzoek van dergelijke drempels een nut?
 of Beieren (perinataal sterftecijfer)... Heeft het onderzoek van dergelijke drempels een nut .")
15
Preston et al. Solid cancer incidence in atomic bomb survivors: 1958-1998. Rad Res 2007 LSS : 105 427 bestraalden17 448 primaire kankers. (LIFE span study: overlevenden van de Japanse nucleaire bommen)
.")
16
Preston et al. Solid cancer incidence in atomic bomb survivors: 1958-1998. Rad Res 2007

17
Estimated excess relative risk (±1 SE) of mortality (1950–97) from solid cancers among groups of survivors in the Life-Span Study cohort of atomic-bomb survivors, who were exposed to low doses (<500 mSv) of radiation (2). The groups, correspond to progressively larger maximum doses, with the mean doses in each group indicated above each data point. The first two data points (in blue) are not statistically significant (p=0.15 and 0.3, respectively) compared to the comparison population who were exposed to less than 5 mSv, while the remaining 4 higher-dose points (in red) are statistically significant (p<0.05). The dashed straight line represents the results of a linear fit (2) to all the data from 5 to 4,000 mSv (higher dose points not shown). David J. Brenner et al, 2003.
 are not statistically significant (p=0.15 and 0.3, respectively) compared to the comparison population who were exposed to less than 5 mSv, while the remaining 4 higher-dose points (in red) are statistically significant (p<0.05). The dashed straight line represents the results of a linear fit (2) to all the data from 5 to 4,000 mSv (higher dose points not shown). David J. Brenner et al,")
18
Alice Stewart: A-bomb data: detection of bias in the Live Span Study Cohort. Env Health Persp 1997;105:1519-21.

19
Zou er een probleem van onderschatting van de gevolgen in LSS bestaan?

20
Waarom een D/DREF ? Impliciet een heroverweging van LSS („Japanse“ Bommen) Overdracht Japanse gegevens andere bevolkingen? Kanker maag/borsten Jap:3134/100 000 mensen USA390 Gebruik ∋ jap: ERREAR Jap > USA !!! Chromosomen studies, cellulair, diertesten. Andere epidemiologische studies… Eenmalige dosis ↔ herhaalde dosissen UNSCEAR 2006 report vol1
 Overdracht Japanse gegevens andere bevolkingen. Kanker maag/borsten Jap:3134/ mensen USA390 Gebruik ∋ jap: ERREAR Jap > USA !!. Chromosomen studies, cellulair, diertesten. Andere epidemiologische studies… Eenmalige dosis ↔ herhaalde dosissen UNSCEAR 2006 report vol1.")
21
Waarom een D/DREF (2) ? * Gebruikt een ratio tussen een lineair model en een kwadratisch model. UNSCEAR 2006 report vol1 BronSchattingbasisD/DREF ICRP (1960, 2007)LSS en andere epidemiologishe data2 UNSCEAR (1993)Dieren data en andere biologishe data<3 BEIR VII (2006)Dieren data, aberraties op menselijke lymphocyten en incidencie LSS data1,5 (1,1 - 2,3) Pierce en Veith (1991)LSS leukemie en sterftecijfers data1,8 (1,0 – 6,0) LSS massieve tumoren1,2 (<1 – 3,1) Little en Muirhead (2000)*LSS leukemie, incidencie: 0-4 Gy2,47 (1,21 - >1000) LSS leukemie, incidencie: 0-2 Gy1,73 (<1 – 117,67) LSS massieve tumoren, incidencie: 0-4 Gy1,06 (<1 – 1,62) LSS massieve tumoren, incidencie: 0-4 Gy1,21 (<1 – 2,15)
LSS en andere epidemiologishe data2 UNSCEAR (1993)Dieren data en andere biologishe data<3 BEIR VII (2006)Dieren data, aberraties op menselijke lymphocyten en incidencie LSS data1,5 (1,1 - 2,3) Pierce en Veith (1991)LSS leukemie en sterftecijfers data1,8 (1,0 – 6,0) LSS massieve tumoren1,2 (<1 – 3,1) Little en Muirhead (2000)*LSS leukemie, incidencie: 0-4 Gy2,47 (1,21 - >1000) LSS leukemie, incidencie: 0-2 Gy1,73 (<1 – 117,67) LSS massieve tumoren, incidencie: 0-4 Gy1,06 (<1 – 1,62) LSS massieve tumoren, incidencie: 0-4 Gy1,21 (<1 – 2,15).")
22
Waarom een D/DREF (3) ? Eenmalige dosis ⇔ herhaalde dosissen UNSCEAR 2006 report vol1 B.v. borstkanker StudieBlootstelling aardGemid. DosisOverledenERR schat.LSS ERR schat Storm et al (1986)Herhaalde borst RX0,27 (0-2,74890,00 (-0,43-0,94)0,90 (0,47-1,48) Tuberculosis (Dan)(90Kv; dose ~10mGy /Rx) Griem et al (1994)Rx therapie? (0-0,17)166,07 (-3,7-39,29)0,74 (0,08-1,87) Ulcere therapie200-250 Kv opgesplitst Howe et al(1994)Herhaalde borst RX0,89 (0-18,4)6880,90 (0,55-1,39)1,56 (0,41-3,53) Tuberculosis(Can)(90Kv; dose ~10mGy /Rx) Doody et al(2000)Herhaalde Rx dosissen0,11 (0-1,7)772,7 (-0,2-9,3)2,62 (1,09-3,53) Scoliosis(USA) <10mGy/Rx
Herhaalde borst RX0,27 (0-2,74890,00 (-0,43-0,94)0,90 (0,47-1,48) Tuberculosis (Dan)(90Kv; dose ~10mGy /Rx) Griem et al (1994)Rx therapie. (0-0,17)166,07 (-3,7-39,29)0,74 (0,08-1,87) Ulcere therapie Kv opgesplitst Howe et al(1994)Herhaalde borst RX0,89 (0-18,4)6880,90 (0,55-1,39)1,56 (0,41-3,53) Tuberculosis(Can)(90Kv; dose ~10mGy /Rx) Doody et al(2000)Herhaalde Rx dosissen0,11 (0-1,7)772,7 (-0,2-9,3)2,62 (1,09-3,53) Scoliosis(USA) <10mGy/Rx.")
23
Eugenio Picano. Sustainability of medical imaging. BMJ 2004;328:578-580 UNSCEAR 2006 : 1,88 mSv (Rx ) + 0,13 mSv (nucleaire geneesk.)
 + 0,13 mSv (nucleaire geneesk.).")
24
Verhouding degenen die „High School“ in Zweden bereiken : BMJ 2004;328:1-5 CT scan telt voor ongeveer 75% van de bestraling door Rx (Picano, 2004) en gaat van 100 mSv (CT kind hoofd) tot 2000 mSv (CT neonat buik ) - dosis equivalent - Het gaat om Rx of beta behandelingen voor aangezichts-hemangiomes
 en gaat van 100 mSv (CT kind hoofd) tot 2000 mSv (CT neonat buik ) - dosis equivalent - Het gaat om Rx of beta behandelingen voor aangezichts-hemangiomes")
25
Results The proportion of boys who attended high school decreased with increasing doses of radiation to both the frontal and the posterior parts of the brain from about 32% among those not exposed to around 17% in those who received > 250 mGy. For the frontal dose, the multivariate odds ratio was 0.47 (95% confidence interval 0.26 to 0.85, P for trend 0.0003) and for the posterior dose it was 0.59 (0.23 to 1.47, 0.0005). A negative dose-response relation was also evident for the three cognitive tests for learning ability and logical reasoning but not for the test of spatial recognition. Conclusions Low doses of ionising radiation to the brain in infancy influence cognitive abilities in adulthood. Per Hall, Hans-Olov Adami, Dimitrios Trichopoulos, Nancy L Pedersen, Pagona Lagiou, Anders Ekbom, Martin Ingvar, Marie Lundell, Fredrik Granath; 2004
 and for the posterior dose it was 0.59 (0.23 to 1.47, ). A negative dose-response relation was also evident for the three cognitive tests for learning ability and logical reasoning but not for the test of spatial recognition. Conclusions Low doses of ionising radiation to the brain in infancy influence cognitive abilities in adulthood. Per Hall, Hans-Olov Adami, Dimitrios Trichopoulos, Nancy L Pedersen, Pagona Lagiou, Anders Ekbom, Martin Ingvar, Marie Lundell, Fredrik Granath;")
26
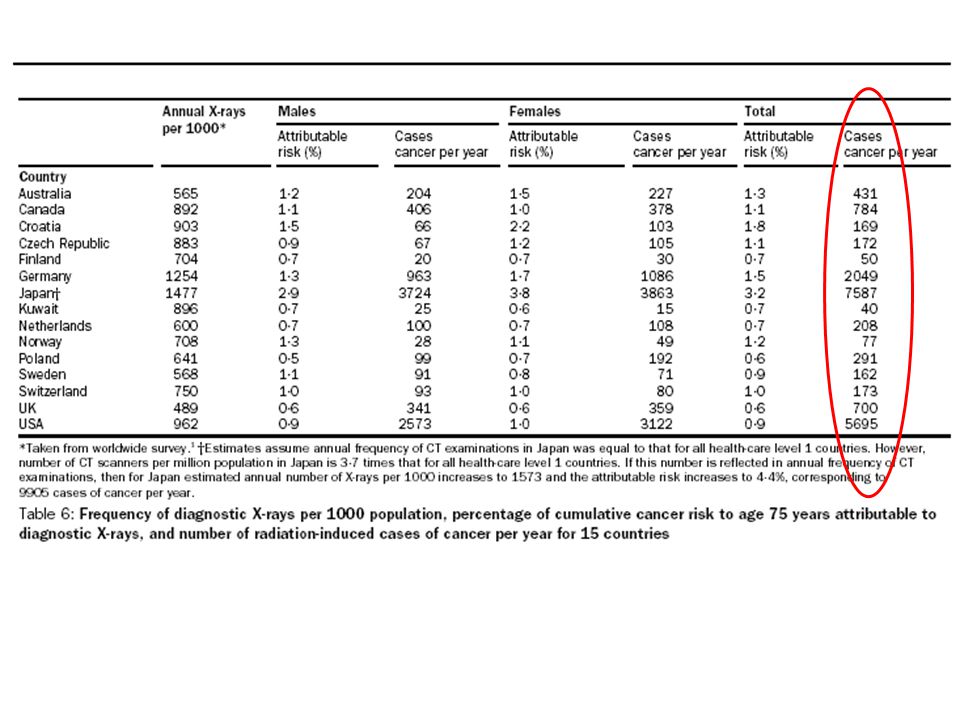
Our results indicate that in the UK about 0.6% of the cumulative risk of cancer to age 75 years could be attributable to diagnostic X-rays. This percentage is equivalent to about 700 cases of cancer per year. In 13 other developed countries, estimates of the attributable risk ranged from 0.6% to 1.8%, whereas in Japan, which had the highest estimated annual exposure frequency in the world, it was more than 3%. Berrington de Gonzalez A, Darby S. Risk of cancer from diagnostic X-rays: estimates for the UK and 14 other countries. Lancet 2004; 363: 345-351. Modellering van medische beeldvorming door RX

28
Cardis et al, BMJ, 2005;331:77 % bijdrage = 49%

29
Solid cancer incidence: Techa River Krestinina LY, Davis F, Ostroumova EV et al. Solid cancer incidence and low-dose- rate radiation exposures in the Techa River cohort: 1956-2002. Int J Epidemiol 2007;36:1038-46. Commentary: E Cardis.

30
ERR / Sv : herhaalde dosissen Estimates of excess relative risk per Sv (95% confidence interval) for all cancers (solid cancers) excluding leukaemia. 15 country study Techa riverAtomic bomb survivors No.CcancersRiskNo.CancersRisk No.Cancers Risk 47000,87 (0,03 - 1,88)18361,00 (0,3 - 1,9)32460,32 (0,01 - 0,50) NB: « Strong healthy worker survivor effect » (Cardis 2007) als het selectief gevolg voor de N-H overlevenden ? Techa river en borst kanker: ERR 5,00 /Sv (0,80 - 12,76) (Ostroumova E et al, Br J Cancer 2008) Canadian nuclear power, solid cancer: ERR 2,80 (-0,038 – 7,13) (mean cumul equiv. dose: 13,5 mSv). Zablotska LB et al, Radiat Res 2004)
18361,00 (0,3 - 1,9)32460,32 (0,01 - 0,50) NB: « Strong healthy worker survivor effect » (Cardis 2007) als het selectief gevolg voor de N-H overlevenden . Techa river en borst kanker: ERR 5,00 /Sv (0, ,76) (Ostroumova E et al, Br J Cancer 2008) Canadian nuclear power, solid cancer: ERR 2,80 (-0,038 – 7,13) (mean cumul equiv. dose: 13,5 mSv). Zablotska LB et al, Radiat Res 2004).")
31
10 - 3 10 -4 10 - 5 10 -2 15 countries study Clarke R. Control of low-level radiation exposure: time for a change ? J Radiol Prot 1999;19:107-15.

32
Table 5 Comparison of ERR estimates per Sv between nuclear workers and atomic bomb survivors 15-Country StudyAtomic bomb survivors (men exposed between the ages of 20 and 60)a Cause of death N ERR/Sv (95% CI) N ERR/Sv (95% CI) Non-cancer diseases 11 255 0.24 (–0.23, 0.78) 4563 0.12 (0.01, 0.24) Circulatory diseases 8412 0.09 (–0.43, 0.70) 2571b 0.16 (0.02, 0.32) Respiratory diseases 792 1.16 (–0.53, 3.84) 911 0.04 (–0.17, 0.30) Digestive diseases 620 0.96 (<0, 4.52) 370 –0.03 (–0.35, 0.40) Liver cirrhosis 263 1.54 (<0, 9.67) 167 0.02 (<0, 0.73) aAnalyses of non-cancer disease mortality of A-bomb survivor data carried-out at IARC, using an excess relative risk model stratified for attained age, calendar period and city. Analyses were restricted to men, exposed between the ages of 20 and 60, the group most comparable to the nuclear workers in the 15-Country study. Analyses were restricted to follow-up data 1968–97 and to survivors proximal to the hypocenter (<3 km) as described in Report 13 by Preston et al11. bCategories heart disease and stroke from Report 1311 combined. Mortality from diseases other than cancer following low doses of ionizing radiation: results from the 15-Country Study of nuclear industry workers Vreiheid, Cardis et al 2007.
 as described in Report 13 by Preston et al11. bCategories heart disease and stroke from Report 1311 combined. Mortality from diseases other than cancer following low doses of ionizing radiation: results from the 15-Country Study of nuclear industry workers Vreiheid, Cardis et al")
33
Spix et al. EJC 2008;44:275-84 Blootstelling door kerncentrales in Duitsland <0,3 mSv/jaar

34
Is het gebruik van D/DREF in de realiteit belangkrijk ? Het voorbeeld van opsporing van borstkanker... Heyes GJ, Mill AJ Charles MW. Enhanced biological effectiveness of low energy X- rays and implications for the UK breast screening programme. Br J Radiol 2006;79:195-200.

35
Correspondance. (Br J Radiol 2007;80:141-142). « The discussions presented in the october edition of the BJR, although scientifically relevant, are obviously somewhat esoteric in relation to the existing practicalities of radiation protection within the UKBSP. However, the points raised above are, I believe, of direct practical relevance and concern to over 50% of the patient population who undergo radiological procedures as well as the scientific community that supports these activities. » BM Moores.

36
D/DREF = 1 for breast cancer risk (EPA: Puskin JS, Nelson CB. Estimation radiogenic cancer risks, report 402-R-93-076. EPA 1994. RBE 1 – 6 mean 4,42 mammography compared with N-H atomic bomb spectrum (Heyes Gj, Mill AJ. Rad Res 2004;162:120-7.) Two-view screening:Normal dose = 4,5 mGy High dose = 21,4 mGy
 Two-view screening:Normal dose = 4,5 mGy High dose = 21,4 mGy.")
37
*(a) and (b) Patient index = mother, sister, daughter with family history and *age of the screened woman
 and (b) Patient index = mother, sister, daughter with family history and *age of the screened woman")
38
Welke norm voor A-T heterozygotes ? (AT = ataxia telangiectasia) of hoe het voorzorgsprincipe toepassen 0,6 à 1% van de bevolking Anti-tumor gen 5-6x meer gevoelig aan ioniserende stralingen ? (Swift M et al. NEJM 1991;325:1831-6.) * heterozygotie voor A-T, borstkanker en cigaretten : Jaarlijkse incidencie: AT+ 1,4%AT- 0,20% Gecumuleerde incidencie (80 j. oud) : AT+ 43%AT- 17% Gecumuleerde incidencie (80 j. oud):AT+&Cig 80%AT+ 21% (Swift M & Lukin JL, Cancer Epidemiol Biomarkers Prev 2008;17:1-4.)
 of hoe het voorzorgsprincipe toepassen 0,6 à 1% van de bevolking Anti-tumor gen 5-6x meer gevoelig aan ioniserende stralingen . (Swift M et al. NEJM 1991;325: ) * heterozygotie voor A-T, borstkanker en cigaretten : Jaarlijkse incidencie: AT+ 1,4%AT- 0,20% Gecumuleerde incidencie (80 j. oud) : AT+ 43%AT- 17% Gecumuleerde incidencie (80 j. oud):AT+&Cig 80%AT+ 21% (Swift M & Lukin JL, Cancer Epidemiol Biomarkers Prev 2008;17:1-4.).")
39
Risico analyse Wat is de onderliggende inzet? Arbeidsgezondheid ? Publieke gezondheid ? & Onzekerheden Justificatie Optimisatie

40
Het voorzorg principe « Het beleid van de Gemmeschap beoogt een hoog niveau van bescherming. Zij is gebaseerd op het principe van voorzorg en preventieve actie, op het principe van correctie prioritair aan de bron van de aanslagen op het milieu en het principe van de vervuiler betaalt. » Verdrag van Maastricht 1992. Beginsel 15 (Conferentie van Rio van 1992) « Teneinde het milieu te beschermen zullen staten naar hun vermogen op grote schaal de voorzorgsbenadering moeten toepassen. Daar waar ernstige of onomkeerbare schade dreigt, dient het ontbreken van volledige wetenschappelijke zekerheid niet als argument te worden gebruikt voor het uitstellen van kosten- effectieve maatregelen om milieuaantasting te voorkomen. »
 « Teneinde het milieu te beschermen zullen staten naar hun vermogen op grote schaal de voorzorgsbenadering moeten toepassen. Daar waar ernstige of onomkeerbare schade dreigt, dient het ontbreken van volledige wetenschappelijke zekerheid niet als argument te worden gebruikt voor het uitstellen van kosten- effectieve maatregelen om milieuaantasting te voorkomen. ».")
41
Dank U voor uw geduld …

Verwante presentaties










 Current Baseline (Version 6 – 27 Sept ’02) Endcap A/C.>")







>")
