Download de presentatie
De presentatie wordt gedownload. Even geduld aub

1
Integrated disease management COPD: rol van zelfmanagement, training en eHealth
Niels Chavannes MD PhD Associate Professor Department of Public Health and Primary Care Leiden University Medical Center The Netherlands

2
ERS/ATS Standards for COPD ERJ 2004

4
Patiënten perspectief
Patients with COPD want active involvement in decisionmaking; are more compliant when involved1 Fear of hospitalisation and passive behaviour hampers detection exacerbations2 Recognition personal coping style leads to more effective treatment3 1 Booker Eur Respir Rev 2006 2 Adams et al Prim Care Resp J 2006 3 Osman et al Eur Respir Rev 2006

5
Evidence voor zelfmanagement
Cochrane Review; Effing (2009): self-management education leads to reduction in hospital admissions (OR 0.64, NNT 10-24) significant improvements on SGRQ (-2.58 [-5.1, -0.02]) and small effect BORG-scale (-0.53 [-0.96, -0.1]) Inconclusive effects on exacerbations, ED visits, lung function and medication
: self-management education leads to reduction in hospital admissions (OR 0.64, NNT 10-24) significant improvements on SGRQ (-2.58 [-5.1, -0.02]) and small effect BORG-scale (-0.53 [-0.96, -0.1]) Inconclusive effects on exacerbations, ED visits, lung function and medication.")
6
Evidence voor zelfmanagement
Cochrane Review; Walters (2010): exacerbation action plans with limited patient education lead to better recognition (MD 2.5 [1.04, 3.96]) and self initiating action in severe exacerbations (MD 1.5 [ 0.62, 2.38]) No evidence for reduced healthcare utilisation or improved HRQoL; => should be part of multi-faceted self-management program or ongoing case management
: exacerbation action plans with limited patient education lead to better recognition (MD 2.5 [1.04, 3.96]) and self initiating action in severe exacerbations (MD 1.5 [ 0.62, 2.38]) No evidence for reduced healthcare utilisation or improved HRQoL; => should be part of multi-faceted self-management program or ongoing case management.")
7
Minder ziekenhuisopnames bij ernstig COPD
Bourbeau (Arch Int Med 2003): self-management in severe COPD leads to 40% reduction in hospital admissions Rice (AJRCCM 2010): relatively simple DM program for severe COPD reduces hospitalizations and ED visits after one year by 41% (MD 0.34 [0.15, 0.52], p<0.001) 1-1.5hr education, exacerbation action plan, case manager
: self-management in severe COPD leads to 40% reduction in hospital admissions. Rice (AJRCCM 2010): relatively simple DM program for severe COPD reduces hospitalizations and ED visits after one year by 41% (MD 0.34 [0.15, 0.52], p<0.001) 1-1.5hr education, exacerbation action plan, case manager.")
8
Recente ontwikkelingen
Bisschoff (Thorax 2011): In severe COPD, adherence to written exacerbation action plan (40%) is associated with reduction in recovery time (-5.8 days, p=0.0001) No effect on unscheduled healthcare utilisation Trappenburg (Thorax 2011): Individualised action plan in moderate-severe COPD decreases impact of exacerbations on health status (HR 1.58 [0.96, 2.6]) and tends to accelerate recovery (-3.7 days [-7.3, -0.04]) Action plan plus ongoing support by case manager
: In severe COPD, adherence to written exacerbation action plan (40%) is associated with reduction in recovery time (-5.8 days, p=0.0001) No effect on unscheduled healthcare utilisation. Trappenburg (Thorax 2011): Individualised action plan in moderate-severe COPD decreases impact of exacerbations on health status (HR 1.58 [0.96, 2.6]) and tends to accelerate recovery (-3.7 days [-7.3, -0.04]) Action plan plus ongoing support by case manager.")
9
Nut van eHealth? Trappenburg (Telemed J E Health 2008): Telemonitoring in severe COPD decreases hospitalisations ( / vs. control /- 1.0, p = 0.02) and exacerbations ( /- 1.4 vs. control /- 1.2, p = 0.004) No effect on HRQoL, but baseline differences flawed study Bartoli (Telemed J E Health 2009): rethinking of organization structure mandatory to maximize technological benefits Pinnock (PCRJ 2011): patients perceive telemonitoring as improving access to professional care, but clinicians concerned about over-treatment and how best to organise
: Telemonitoring in severe COPD decreases hospitalisations ( / vs. control /- 1.0, p = 0.02) and exacerbations ( /- 1.4 vs. control /- 1.2, p = 0.004) No effect on HRQoL, but baseline differences flawed study. Bartoli (Telemed J E Health 2009): rethinking of organization structure mandatory to maximize technological benefits. Pinnock (PCRJ 2011): patients perceive telemonitoring as improving access to professional care, but clinicians concerned about over-treatment and how best to organise.")
10
Internet-support In participants with a history of admission for exacerbations of COPD, telemonitoring was not effective in postponing admissions and did not improve quality of life. The positive effect of telemonitoring seen in previous trials could be due to enhancement of the underpinning clinical service rather than the telemonitoring communication.

12
Methode Participants: COPD (GOLD criteria) patiënten Interventie:
Integrated Disease Management Controle: Usual care Outcome: Primair: Kwaliteit van leven, inspanningstolerantie, exacerbatie gerelateerde uitkomsten

13
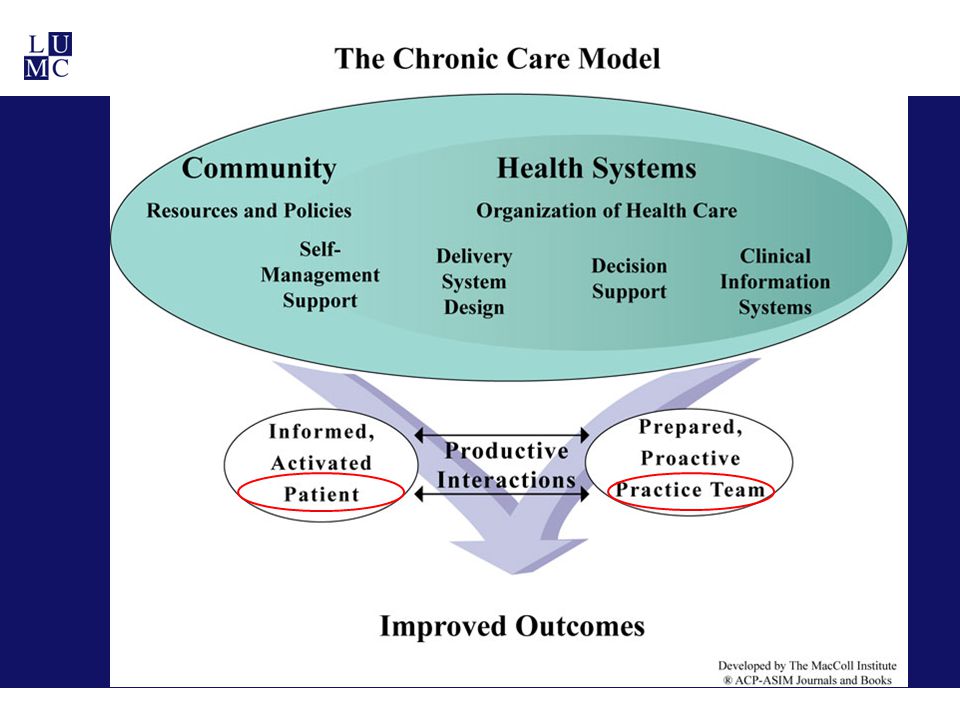
Integrated disease management?
Interventie Integrated disease management? Multidisciplinair (≥ 2 zorgverleners) Multi treatment (≥ 2 componenten) Duur ≥ 3 maanden
 Multi treatment (≥ 2 componenten) Duur ≥ 3 maanden.")
14
Multi treatment (≥ 2 componenten)
Educatie/zelf-management Trainen Psychosociaal Stoppen met roken Medicatie Dietetiek Follow-up en/of communicatie Multidisciplinair team (i.e. meetings) Financiele interventies (fees for providing) EPOC 2008
 Financiele interventies (fees for providing) EPOC")
15
Geincludeerde studies (N=26)
")
16
Kwaliteit van leven

17
Inspanningstolerantie
MCID = 35 meter

18
Exacerbatie uitkomsten
Aantal exacerbaties: geen statistisch sign verschil

19
Exacerbatie uitkomsten
Aantal ziekenhuisopnames, long gerelateerd:

20
Number needed to treat = 15
Long gerelateerde opnames

21
Exacerbatie uitkomsten
Aantal dagen in ziekenhuis: gemiddeld 4 dagen korter

22
Subgroep analyses Géén verschil in effectiviteit tussen eerste of tweede lijn Programma’s met trainingselement lieten grotere verbeteringen zien dan zelfmanagementprogramma’s Indien controlegroep ook één onderdeel van zorg bevatte (ipv usual care) was het effect minder groot
 was het effect minder groot.")
24
Meta-analysis (1) I will no go on with the results of the meta-analysis of our review. The meta-analysis showed an overall health care utilzations savings of almost 900 euros. The pooled results lay in the left side of the 0 line, indicating a significant cost saving of the DM group.

25
Meta-analysis (2) These savings are largely due to the hospitalization costs, which were about 1060 euros.
 These savings are largely due to the hospitalization costs, which were about 1060 euros.")
26
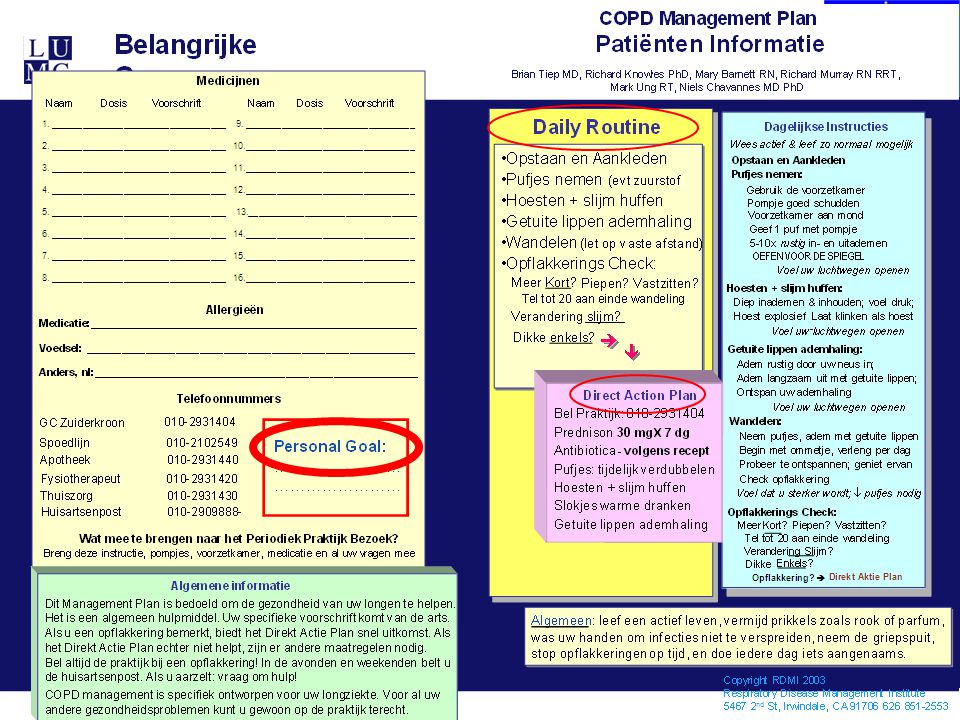
Planner voor hulpverlener
26

27
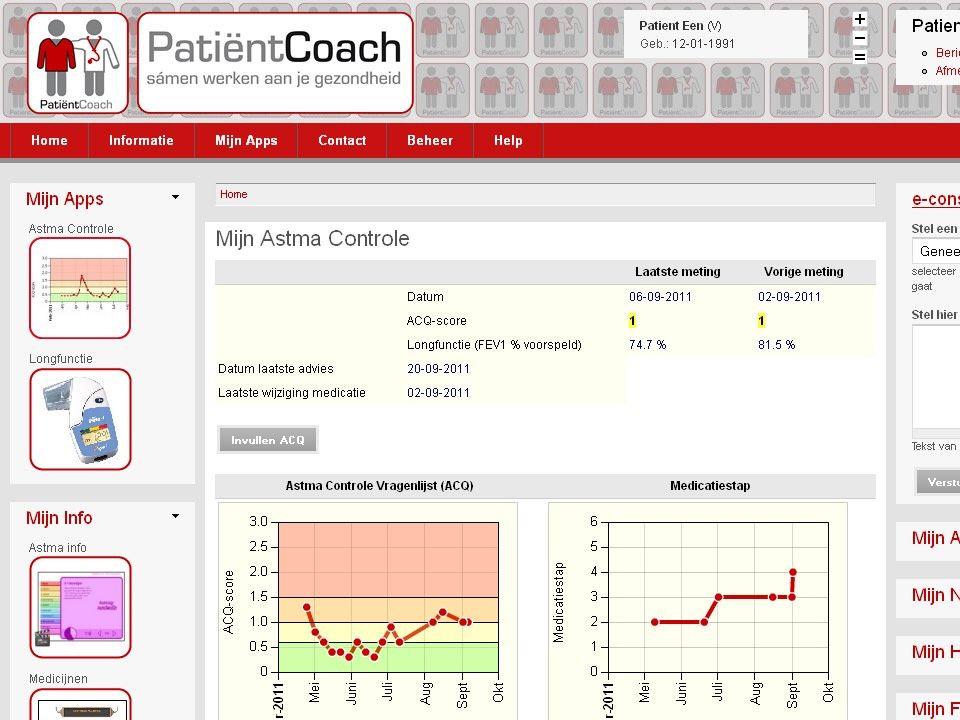
Web-based dossier 27

28
Toegankelijk voor patiënt
28

29
Empowerment van participerende patiënten
29

32
Op maat gesneden interventie, ondersteund door eHealth
Koff (ERJ 2009): A proactive integrated care program in (very) severe COPD improves SGRQ by units [-17.4, -3.1] vs units [-6.5, 5.3] p=0.018) in usual care Health buddy system identifying all exacerbations correctly Chavannes (PCRJ 2009): Integrated disease management in mild to moderate COPD with MRC Dyspnoea score >2 improved SGRQ by units ([-20.8, -6.1] p=0.002) vs units [-5.5, 4.9] p=0.9) in usual care Tailored intervention: personal goals, capabilities & needs, aimed at improving and sustaining health status
: A proactive integrated care program in (very) severe COPD improves SGRQ by units [-17.4, -3.1] vs units [-6.5, 5.3] p=0.018) in usual care. Health buddy system identifying all exacerbations correctly. Chavannes (PCRJ 2009): Integrated disease management in mild to moderate COPD with MRC Dyspnoea score >2 improved SGRQ by units ([-20.8, -6.1] p=0.002) vs units [-5.5, 4.9] p=0.9) in usual care. Tailored intervention: personal goals, capabilities & needs, aimed at improving and sustaining health status.")
34
Sustained effects of Integrated Disease Management on Health Status in primary care COPD-patients (Kruis IJCOPD 2010)* Intervention group CCQ difference** / 95% CI p-value Control group At 12 months -0.4 [-0.6, -0.2] 0.001 +0.01 [-0.2, 0.2] 0.9 At 24 months [-0.7, -0.1] 0.004 +.02 [-0.4, 0.5] *paired samples T-test; p is considered significant at values<0.05; **MCID CCQ = -0.4 CCQ, Clinical COPD Questionnaire

35
Longterm effects of Integrated Disease Management in Bocholtz Study on Health Status in primary care COPD-patients with baseline CCQ>1* Intervention group CCQ difference** / 95% CI p-value Control group At 12 months -0.8 [-1.1, -0.4] 0.001 -0.1 [-0.3, 0.08] 0.2 At 24 months -0.9 [-1.2, -0.5] -0.03 [-0.5, 0.5] 0.9 *paired samples T-test; p is considered significant at values<0.05; **MCID CCQ = -0.4 CCQ, Clinical COPD Questionnaire

36
Longterm effects of Integrated Disease Management in Bocholtz Study on Health Status in primary care COPD-patients with baseline MRC>2* Intervention group CCQ difference** / 95% CI p-value Control group At 12 months -0.9 [-1.4, -0.4] 0.002 +0.01 [-0.3, 0.3] 1 At 24 months -1.2 [-1.8, -0.5] 0.004 -0.02 [-0.8, 0.8] *paired samples T-test; p is considered significant at values<0.05; **MCID CCQ = -0.4 CCQ, Clinical COPD Questionnaire

37
RECODE trial @ LUMC & EMC Netherlands
Large RCT in primary care COPD patients (1100+) with two-year follow-up Assessing effectiveness of integrated disease management on health status (CCQ, SGRQ) and cost-effectiveness Powered to assess differential effects in subgroup (MRC>2) Supported by patient portal aimed at case management First results expected beginning of 2014
 with two-year follow-up. Assessing effectiveness of integrated disease management on health status (CCQ, SGRQ) and cost-effectiveness. Powered to assess differential effects in subgroup (MRC>2) Supported by patient portal aimed at case management. First results expected beginning of")
38
RECODE model

39
Concluderend: -Zelfmanagement vermindert ziekenhuisopnames bij ernstig COPD -Actieplannen bevorderen herkenning en herstel van exacerbaties -Integrated disease management verbetert KvL en inspanningstolerantie; training >>zelfmanagement -Integrated disease management vermindert aantal en duur van ziekenhuisopnames=> minder ziektekosten! -Behandeling op maat is de toekomst -eHealth is een middel, niet het doel

Verwante presentaties








 Current Baseline (Version 6 – 27 Sept ’02) Endcap A/C.>")










