Download de presentatie
De presentatie wordt gedownload. Even geduld aub

1
Moji Aghajani, Juriena de Vries,
Is er onderscheid (eerste) depressie in kader van een unipolaire of bipolaire stoornis? Moji Aghajani, Juriena de Vries, Allison Jones,Mimi Nuijens, Charlotte van Schie Erik Hoencamp , Marc Blom
 depressie in kader van een unipolaire of bipolaire stoornis Moji Aghajani, Juriena de Vries, Allison Jones,Mimi Nuijens, Charlotte van Schie. Erik Hoencamp , Marc Blom.")
2
Waarom is de vraag klinisch relevant? Consequenties voor :
Diagnostiek Missen diagnose bipolair in primary care.(Smith 2011,BrJP) %! Verkeerde diagnose: BD als depressie duiden BD als schizofrenie duiden (paranoide psychotische manie) Behandeling Niet gebruiken stemmingsstabilisator Onnodig gebruik antipsychotica
 %! Verkeerde diagnose: BD als depressie duiden. BD als schizofrenie duiden (paranoide psychotische manie) Behandeling. Niet gebruiken stemmingsstabilisator. Onnodig gebruik antipsychotica.")
3
Vragen Is niet elke depressie in het kader van een bipolaire stoornis (Akishkal). Spelen twee seperate dimensies een rol stemming wisselingen en psychotische symptomen. Kwetsbaarheid stemmingswisseling? Bi.Po 1 Tijd verloop depressie BiPo nao Kwetsbaarheid psychose ? BiPo 2

4
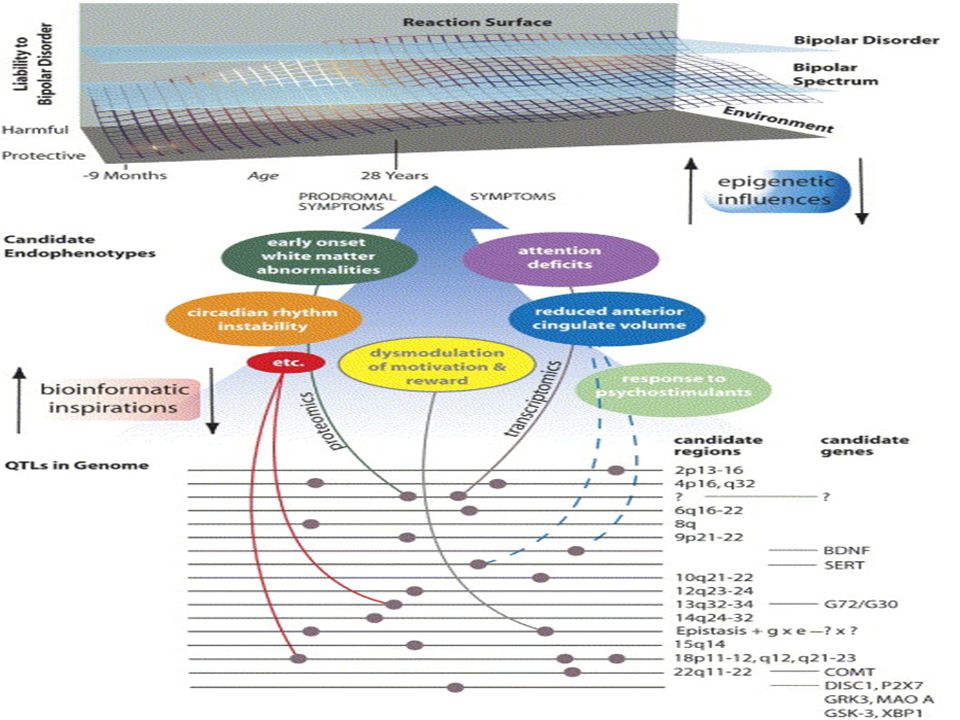
Literatuur onderzoek verschil unipolaire versus bipolaire stoornis op niveau van
Phenotype Endophenotype Omgeving Genotype Ordening van resultaten volgens het heuristisch model van Hassler (2004). Met proximale en distale factoren die uiteindelijk kunnen leiden tot een stoornis
. Met proximale en distale factoren die uiteindelijk kunnen leiden tot een stoornis.")
5
++ Sterk bewijs ondersteunt verschil
Methode Keywords, laatste 10 jaar, meeste gewicht aan onderzoeken die in een populatie uni-versus bipolair hebben onderzocht . ++ Sterk bewijs ondersteunt verschil - - Sterk bewijs ondersteunt geen verschil + Zwak bewijs ondersteunt verschil - Zwak bewijs ondersteunt geen verschil In deze presentatie alleen ++ resultaten besproken

6
Verschillen op phenotype niveau (++)
UD. Anhedonie, emotioneel vlak Gewichtsverlies Angst Langere duur depressieve episode Later age of onset. Insomnia Somatische klachten BD. Psychomotore retardatie (leaden paralysis) Suicidaliteit Woede Stemmings reactivteit Dagschommeling Hypersomnia Psychose
 Suicidaliteit. Woede. Stemmings reactivteit. Dagschommeling. Hypersomnia. Psychose.")
7
Verschillen op omgevings niveau (++)
UD. Geen gevonden Childhood adversity komt in beide voor en lijkt niet onderscheidend. BD. Verstoringen sociaal rhythm. Parental suicide

8
Verschillen op endophenotype niveau (++).
UD Tyramine Excretie test verlaagd. Slechtere strategy gebruik. EEG grotere gamma activatie BD Meer HPA as pathalogie. Slechtere executive functioning , verbal fluency and attention. EEG hoger alpha –beta ritme Total sleep Deprivation responder.

9
Verschillen op genotype niveau (++)
UD CRY 1 BD Clock VIP

10
Een mogelijk model waarin BD zich onderscheid van UD (invalshoek circadische ritme).
Psychomotore retardatie (leaden paralysis) Suicidaliteit Woede, Psychose. Stemmings reactivteit Dagschommeling Hypersomnia Verstoringen sociaal rhythm. Parental suicide Meer HPA as pathalogie. Reactie Total sleep Deprivation Slechtere executive functioning , verbal fluency and attention. EEG hoger alpha –beta ritme Clock gene , VIP gene
 Suicidaliteit. Woede, Psychose. Stemmings reactivteit. Dagschommeling. Hypersomnia. Verstoringen sociaal rhythm. Parental suicide. Meer HPA as pathalogie. Reactie Total sleep Deprivation. Slechtere executive functioning , verbal fluency and attention. EEG hoger alpha –beta ritme. Clock gene , VIP gene.")
11
Wat heeft dit voor gevolg in de kliniek?
Gebruik van een checklist die proximale (symptomen) en distale factoren (familie en voor geschiedenis) van een depressieve fase tussen UD of BD onderscheid. Quick and dirty? De HCL 23 of BSDS? Nee die kijken met name naar de (hypo)mane symptomen en hebben een lage predictieve waarde in onderzoek bij patienten met een UD volgens Smith(2011). Of te wel de(hypo)mane symptomen zijn niet onderscheidend doch andere factoren.
 en distale factoren (familie en voor geschiedenis) van een depressieve fase tussen UD of BD onderscheid. Quick and dirty De HCL 23 of BSDS Nee die kijken met name naar de (hypo)mane symptomen en hebben een lage predictieve waarde in onderzoek bij patienten met een UD volgens Smith(2011). Of te wel de(hypo)mane symptomen zijn niet onderscheidend doch andere factoren.")
12
Hypomania/Mania Symptom Checklist (HCL-32)
The HCL-32 is a screening tool for researchers trying to find people with bipolar disorder. This is one of the better "complete but simple" lists of manic-side symptoms. It's a good "fine-tooth comb" when people want to inventory all possible hypomanic symptoms, usually in the context of asking "do I really have bipolar disorder?” Remember, however, that this is not exactly the right question. As at the Harvard bipolar clinic, we should instead be asking "how much bipolarity might you have?" In that clinic's Bipolarity Index, you'll note that hypomania or mania only account for up to 1/5th of the possible score; the other 4/5th's of the total 100 points possible come from other factors such as family history, age of onset of depression, course of the depressions since, and response to medications.

13
Totale plaatje is wat gecompliceerder

14
Dank voor uw aandacht en tijd voor reacties ??

16
Social Zeitgeber theory, life events lead to affective episodes caused by social and biological rhythm disruptions. Grandin, Alloy, and Abramson (76).
..")
Verwante presentaties










manische ontwikkeling bij olanzapine gebruik>")




![Deltion College Engels B1 Gesprekken voeren [Edu/005] thema: applying for a job can-do : kan een eenvoudig sollicitatiegesprek voeren © Anne Beeker Alle.](/9/2250293/big_thumb.jpg "Deltion College Engels B1 Gesprekken voeren [Edu/005] thema: applying for a job can-do : kan een eenvoudig sollicitatiegesprek voeren © Anne Beeker Alle.>")



![Deltion College Engels B1 Schrijven [Edu/003] thema: what have I done wrong…? can-do : kan e-mails/ brieven schrijven over persoonlijke zaken © Anne Beeker.](/10/2837503/big_thumb.jpg "Deltion College Engels B1 Schrijven [Edu/003] thema: what have I done wrong…? can-do : kan e-mails/ brieven schrijven over persoonlijke zaken © Anne Beeker.>")