Download de presentatie
De presentatie wordt gedownload. Even geduld aub

1
Benigne Paroxysmale Positie Duizeligheid (BBPD)
Diagnose en behandeling

2
BPPD: achtergrond Meest voorkomende oorzaak van vertigo
Binnenoor probleem dat leidt tot kortdurende, zeer hevige draaiduizeligheid. Benigne: geen ernstige of progressieve aandoening Paroxysmaal: aanvalsgewijs, plots en onvoorspelbaar begin Positie: treedt op bij verandering positie hoofd Duizeligheid: veroorzaakt draaiduizeligheid. M

3
BPPD: symptomen Aanvallen van duizeligheid met misselijkheid en een braakneiging. Aanvallen duren hooguit enkele minuten. Tussen aanvallen in helemaal goed. Uitlokbaar door plotse hoofdbewegingen en omdraaien in bed. M

4
BPPD: ‘oor’ - zaak M

5
BPPD: het binnenoor M

6
BPPD: canalolythiasis theorie
Meest geaccepteerde theorie Otolieten (calcium carbonaat deeltjes) zitten normaal vast aan de binnenmembraan in de utriculus en sacculus Utriculus is verbonden met halfcirkelvormige kanalen De otolieten verplaatsen zich uit de utriculus naar het posterieure semicirculaire kanaal (meest verticaal). Positieveranderingen van het hoofd tov zwaartekracht veroorzaken longitudinale bewegingen van deze vrije otolieten door het kanaal. Hierdoor komt de endolymphe in beweging, en dat prikkelt de haarcellen in de cupula, waardoor de sterke draaisensatie ontstaat. ** M
 zitten normaal vast aan de binnenmembraan in de utriculus en sacculus. Utriculus is verbonden met halfcirkelvormige kanalen. De otolieten verplaatsen zich uit de utriculus naar het posterieure semicirculaire kanaal (meest verticaal). Positieveranderingen van het hoofd tov zwaartekracht veroorzaken longitudinale bewegingen van deze vrije otolieten door het kanaal. Hierdoor komt de endolymphe in beweging, en dat prikkelt de haarcellen in de cupula, waardoor de sterke draaisensatie ontstaat. ** M.")
7
BPPD: canalolythiasis (hypothese)
calcium kristallen zinken in het kanaal en klonteren PC-AD liggend utriculus zittend zwaartekracht fast position change leads after a latency to vertigo and nystagmus that decreases in time and upon repetition (fatigue) M
 M.")
8
BPPD: M

9
Mogelijke oorzaken van canalolithiasis en cupulolithiasis
Verstoring in het statolith metabolisme (vasculair, veroudering, Ca2+ metabolisme/ osteoporose) Hoofdtrauma (statolith loslating door schok) Bed rust (klontering van statolieten in kanalen) Ontsteking (neuritis vestibularis, labyrinthitis, ooroperaties) Idiopathisch M
 Hoofdtrauma (statolith loslating door schok) Bed rust (klontering van statolieten in kanalen) Ontsteking (neuritis vestibularis, labyrinthitis, ooroperaties) Idiopathisch. M.")
10
BPPD: Hallpike maneuvre

11
BPPD: Hallpike maneuvre

12
BPPD: M

13
BPPD: M

14
BPPD: epley maneuvre M

15
BPPD: Epley bevrijdingsmaneuvre

16
BPPD: M

17
BPPD: M

18
Clinical Trial Ruckenstein (2001) Therapeutic efficacy of the Epley canalith repositioning maneuver. Laryngoscope Eighty-six patients 74% of cases that were treated with one or two canalith repositioning maneuvers had a resolution of vertigo as a direct result of the maneuver. A resolution attributable to the first intervention was obtained in 70% of cases within 48 hours of the maneuver. An additional 14% of cases that were treated had a resolution of vertigo. Only 4% of cases (three patients) manifested BPV that persisted after four treatments.
 manifested BPV that persisted after four treatments.")
19
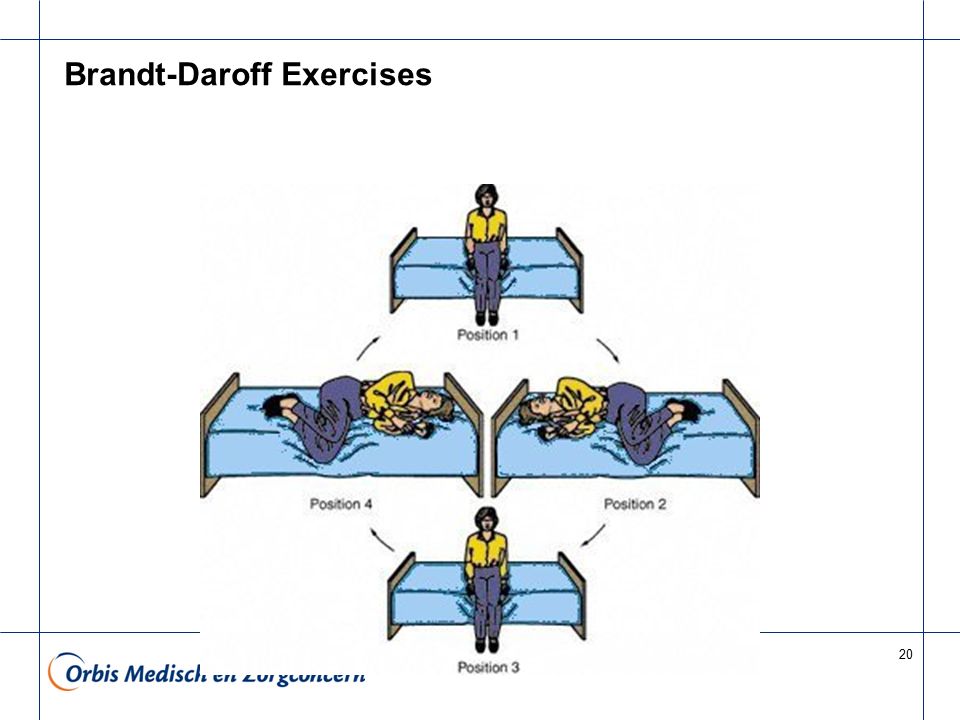
Brandt-Daroff Exercises
method of treating BPPV, usually used when the office treatment fails. These exercises should be performed for two weeks, three times per day for three weeks, twice per day. In each time, one performs the maneuver as shown five times. 1 repetition = maneuver done to each side in turn (takes 2 minutes)
")
20
Brandt-Daroff Exercises
21
Clinical Trial Radtke et al (1999) A modified Epley's procedure for self-treatment of benign paroxysmal positional vertigo. Neurology Compared the efficacy of a modified Epley's procedure (MEP) and Brandt-Daroff exercises (BDE) for self-treatment of (PC-BPPV) 54 patients. PC-BPPV resolved within 1 week in 18 of 28 patients (64%) using the MEP 6 of 26 patients (23%) performing BDE The MEP is more suitable for self-treatment of PC-BPPV than conventional BDE
 and Brandt-Daroff exercises (BDE) for self-treatment of (PC-BPPV) 54 patients. PC-BPPV resolved within 1 week in. 18 of 28 patients (64%) using the MEP. 6 of 26 patients (23%) performing BDE. The MEP is more suitable for self-treatment of PC-BPPV than conventional BDE.")
Verwante presentaties





 He had slept/had been sleeping for 3 hours when I woke him. Hij had al 3 uur geslapen toen ik hem.>")



>")




>")
![Deltion College Engels B1 Lezen [no. 001] can-do : 2 products compared.](/10/2836380/big_thumb.jpg "Deltion College Engels B1 Lezen [no. 001] can-do : 2 products compared.>")
![Deltion College Engels B1 Gesprekken voeren [Edu/008] theme: ‘I have to arrest you, you’ve stolen my heart’ … can-do : kan een eenvoudig face-to-face gesprek.](/10/2836745/big_thumb.jpg "Deltion College Engels B1 Gesprekken voeren [Edu/008] theme: ‘I have to arrest you, you’ve stolen my heart’ … can-do : kan een eenvoudig face-to-face gesprek.>")


