Download de presentatie
De presentatie wordt gedownload. Even geduld aub

1
Probleemgedrag, richtlijn NVVA 2008
Jos Mol, Sociaal geriater

2
Definitie Alle gedrag van de patiënt dat door deze patiënt en/of zijn omgeving als moeilijk hanteerbaar wordt ervaren

3
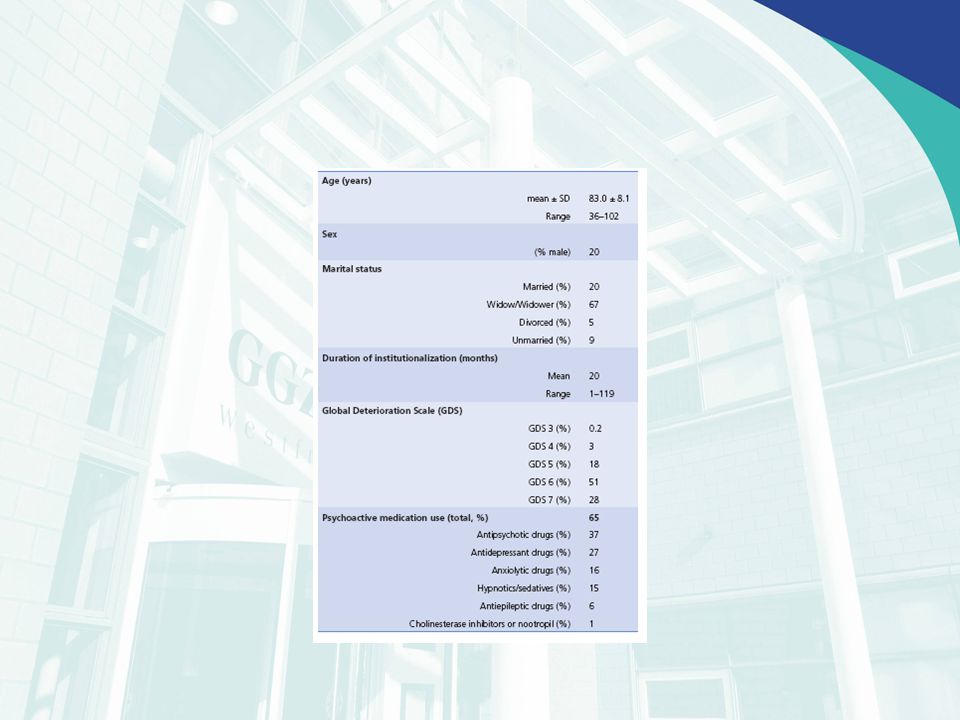
Prevalentie

4
Probleembeschrijving (p7)
Duur en frequentie Plaats en omstandigheden Determinanten Gevolgen Verklaring

5
Aanvullend onderzoek De verpleeghuisarts heeft de regie!
Schakelt zo nodig anderen in Psycholoog Verpleegkundigen Observatieschalen Verpleeghuisarts heeft globale kennis van deze schalen

6
Oorzaken probleemgedrag (p8)
Lichamelijke factoren Pyschische factoren Persoonlijke factoren Omgevingsfactoren

7
Risocofactoren Persoonlijke Psychische Cerebrale beschadigingen
Lichamelijke Sociale factoren Omgevingsfactoren

8
Profiel Persoonlijke Psychische Lichamelijke Cerebrale beschadigingen
Omgevingsfactoren Sociale factoren

9
Profiel Psychische Persoonlijke Cerebrale beschadigingen Lichamelijke
Omgevingsfactoren Sociale factoren

10
Behandeldoelen Probleemgedrag verdwijnt Probleemgedrag vermindert
Probleemgedrag wordt geaccepteerd Probleemgedrag wordt voorkomen Verpleeghuisarts heeft de regie?

11
Behandelbeleid Lichamelijke factoren
Psychosociale gehandeling/begeleiding Psychofarmaca, middelen of maatregelen Niet medische interventies???

13
Evaluatie en beleid Er wordt een duidelijk tijdspad afgesproken voor de evaluatiemomenten

14
Preventie P15 Autonomie en welbevinden
Privacy belevingswereld Veiligheid, woon-/leefomstandigheden Fysieke omgeving Aansluitend aan de behoefte vd patiënt Communicatie Ondersteuning personeel Voldoende bekwaam personeel (taak verpleeghuisarts!!!)
")
15
Medicamenteuze behandeling p22
Opmerking bij delier Clozapine versus riavastigmine bij parkinson Psychosen 1e keus Rsiperdal? Depressie Indicatie Eerst andere interventies Cipramil/Nortrilen Angst

16
Antipsychotica People with Alzheimer’s disease, vascular dementia or mixed dementias with mild-to-moderate non-cognitive symptoms should not be prescribed antipsychotic drugs because of the possible increased risk of cerebrovascular adverse events and death.

17
Literatuur More recently found Schneeweis et all in a large database (n=37241) that atypical antipsychotics have less risc for death than typical antipsychotics (14,1% verus 9.6%).schneeweis There was no difference in the in the group with dementia. Kleijer et all found that people admitted to the hospital with a CVA had more risc to get a CVA when they had used antipsychotic medication. Kleijer This risc was highest within te first 30 days after starting the medication with a peak in the first week (10 fold) . After 30 days this risico decrease an after 3 month is comparable to no users. The also found that user of typical antipsychotics have an increased risc than the users of a typical antispsychotic medication. Douglas and Smeeth imvestigated a gpoup of CVA patients that used antipsychotics befor CVA and concluded at basics of self controlled case studys that all of the antipsychotics have an increased risk for CVA.Douglas The risc for atypical antipsychotics is higher than for typical antipsychotics. They also found that patients with dementia were at higher risc than patient without dementia.
 that atypical antipsychotics have less risc for death than typical antipsychotics (14,1% verus 9.6%).schneeweis There was no difference in the in the group with dementia. Kleijer et all found that people admitted to the hospital with a CVA had more risc to get a CVA when they had used antipsychotic medication. Kleijer This risc was highest within te first 30 days after starting the medication with a peak in the first week (10 fold) . After 30 days this risico decrease an after 3 month is comparable to no users. The also found that user of typical antipsychotics have an increased risc than the users of a typical antispsychotic medication. Douglas and Smeeth imvestigated a gpoup of CVA patients that used antipsychotics befor CVA and concluded at basics of self controlled case studys that all of the antipsychotics have an increased risk for CVA.Douglas The risc for atypical antipsychotics is higher than for typical antipsychotics. They also found that patients with dementia were at higher risc than patient without dementia.")
18
Literatuur Clive Ballard
Ook op langere termijn zijn er behoorlijke risico’s op overlijden Literatuur verzonden aan jullie

Verwante presentaties