Download de presentatie
De presentatie wordt gedownload. Even geduld aub

1
HIV-infecties wereldwijd
Clemens Richter

2
Overzicht Besmetting, natuurlijk beloop Epidemiologie Behandeling
Preventie Risico voor reiziger

3
Hoe raak je besmet? Sexuele transmissie
Bloed- bloed (BT, i.v.drug gebruik, prik-accident) Perinatale transmissie
 Perinatale transmissie.")
5
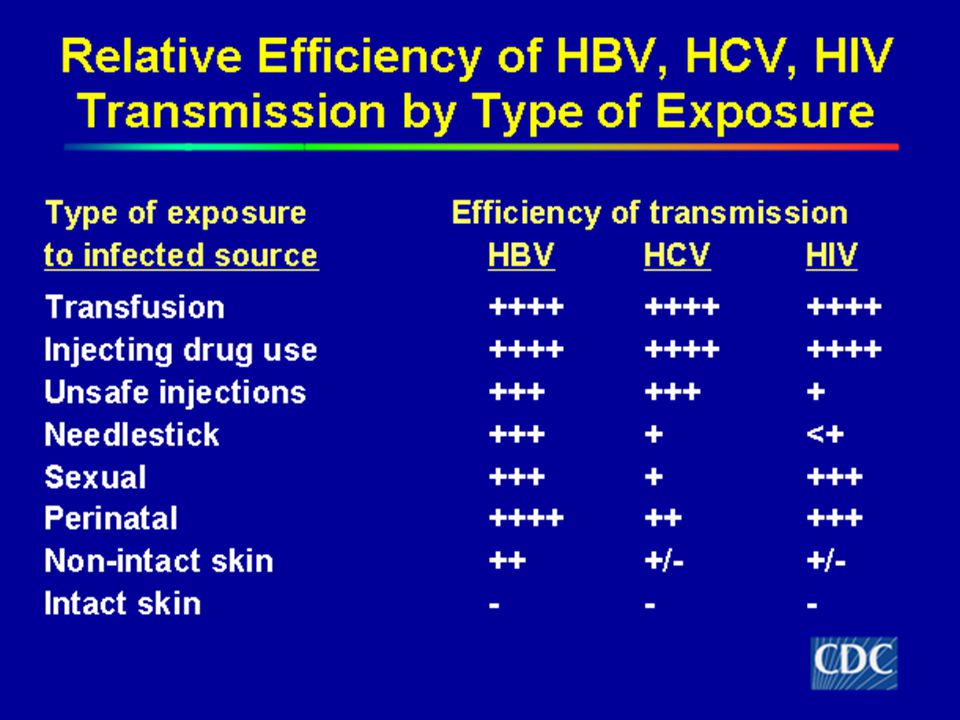
Gemiddeld risico op HIV besmetting bij incidenten
Percutaan 0,3% (HBV 30%, HCV 3%) Slijmvlies 0.1% Niet intacte huid <0.1%
 Slijmvlies 0.1% Niet intacte huid <0.1%")
6
Sexuele transmissie van HIV
Bij eenmalig contact Receptief anaal: % Vaginaal: M to V = %, V to M = % Oraal ~ 10x lager dan vaginaal Cofactor : STDs, geen circumcisie, menstruatie, viral load But many people are surprised to hear how low the per-exposure risk of contracting HIV is, that is, how likely am I to catch HIV from a single sexual contact with an HIV-positive partner? The best estimates are that the riskiest exposures, that is receptive anal intercourse, carries a per-exposure risk of around 1-3%. The risk of HIV transmission from vaginal intercourse is considerably lower, less than 1%. And oral sex carries a much lower risk, so low in fact that the per-contact risk is difficult to calculate from available data. So why is HIV spreading? Surely cofactors are important in transmission, and STDs are known to be one such cofactor.

7
Virale load en transmissie risiko
Studie uit Uganda Virale load Transmissie rate elk jaar < % % 10,000-49, % 50, % Quinn et al, NEJM 2000:342:

8
HIV interaction with CD4 cell
Co-receptor Interaction HIV HIV gp41 Anchorage gp120 HIV CD4 Attachment CXCR4 CCR5 CD4 gp41 Cell Fusion Complete HIV HR1-HR2 Interaction 8

9
HIV-RNA , Steady State Replic.
Rapid (>105) HIV-1 RNA Intermediate Acute infection Slow (<104) Stabilization over 2-3 mos 9
 HIV-1 RNA. Intermediate. Acute. infection. Slow (<104) Stabilization. over 2-3 mos. 9.")
10
Rol van het intestinale immuun system
destructieve fase in darm mucosa vroeg na infectie gevolgd door microbiële translocatie, immuun activatie en uitgebreid verlies van CD4 cellen

11
Acute HIV infection is characterized by a rapid and massive loss of the body’s CD4+ T cells
Plasma viremia Blood CD4+ T cells Body CD4+ T cells Primary infection Death ±Acute HIV syndrome Wide dissemination of virus Seeding of lymphoid organs Opportunistic diseases Clinical latency Constitutional symptoms Relative magnitude Acute HIV is characterized by rapid loss of CD4+ T-cells. This schematic depicts the typical course of HIV infection over time, showing changes in CD4+ T-cell counts through the different stages. The acute phase of HIV infection is associated with a rapid loss of more than 50% of the body’s ‘resting’ effector memory CD4+ T-cells (blue line), mostly occurring in gut-associated lymphoid tissue (GALT), the region of the body where most of the host’s T cells are found.1-3 By targeting CD4+ T cells, the virus can access a widely available and renewable target cell population, allowing massive viral replication early on in infection (green line).4 Later, it may be a combination of HIV-specific cellular and humoral responses and the extreme viral destruction of the majority of CD4+ T cells that decreases viral load to a lower level that may persist for several years, this period marking the onset of the second, chronic phase of infection.5,6 The increased turnover of T-cells due to both direct viral infection and chronic immune activation, leads to dysregulation of T-cell homeostasis, with reduced CD4+ T-cell numbers in peripheral blood (red line).7,8 The chronic phase is characterized by constant high levels of T-cell activation, which is widely considered to be a key driver of HIV disease progression.6 1. Hunt PW. Curr HIV/AIDS Rep 2007; 4:42–47. 2. Brenchley JM, et al. J Exp Med 2004; 200:749–759. 3. Veazey RS, Lackner AA. PLoS Med 2006; 3:e515 4. Picker LJ. Curr Opin Immunol 2006; 18:399–405. 5. Koup RA, et al. J Virol 1994; 68:4650–4655. 6. Derdeyn CA, Silvestri G. Curr Opin Immunol 2005; 17:366–373. 7. Munier ML, Kelleher AD. Immunol Cell Biol 2007; 85:6–15. 8. Sousa AE, et al. J Immunol 2002; 169:3400–3406. 3 6 9 12 1 2 3 4 5 6 7 8 9 10 11+ Weeks Years Time after initial infection 11
, mostly occurring in gut-associated lymphoid tissue (GALT), the region of the body where most of the host’s T cells are found.1-3. By targeting CD4+ T cells, the virus can access a widely available and renewable target cell population, allowing massive viral replication early on in infection (green line).4 Later, it may be a combination of HIV-specific cellular and humoral responses and the extreme viral destruction of the majority of CD4+ T cells that decreases viral load to a lower level that may persist for several years, this period marking the onset of the second, chronic phase of infection.5,6. The increased turnover of T-cells due to both direct viral infection and chronic immune activation, leads to dysregulation of T-cell homeostasis, with reduced CD4+ T-cell numbers in peripheral blood (red line).7,8. The chronic phase is characterized by constant high levels of T-cell activation, which is widely considered to be a key driver of HIV disease progression Hunt PW. Curr HIV/AIDS Rep 2007; 4:42– Brenchley JM, et al. J Exp Med 2004; 200:749– Veazey RS, Lackner AA. PLoS Med 2006; 3:e Picker LJ. Curr Opin Immunol 2006; 18:399– Koup RA, et al. J Virol 1994; 68:4650– Derdeyn CA, Silvestri G. Curr Opin Immunol 2005; 17:366– Munier ML, Kelleher AD. Immunol Cell Biol 2007; 85:6– Sousa AE, et al. J Immunol 2002; 169:3400– Weeks. Years. Time after initial infection. 11.")
12
HIV-epidemie 1990 – 2008

13
Global summary of the AIDS epidemic2013
Number of people living with HIV in 2013 Total Adults Women Children (<15 years) 35.0 million [33.1 million – 37.2 million] 31.8 million [30.1 million – 33.7 million] 16.0 million [15.2 million – 16.9 million] 3.2 million [2.9 million – 3.5 million] 2.1 million [1.9 million – 2.4 million] 1.9 million [1.7 million – 2.1 million] [ – ] 1.5 million [1.4 million – 1.7 million] 1.3 million [1.2 million – 1.5 million] [ – ] People newly infected with HIV in 2013 AIDS deaths in 2013
 35.0 million [33.1 million – 37.2 million] 31.8 million [30.1 million – 33.7 million] 16.0 million [15.2 million – 16.9 million] 3.2 million [2.9 million – 3.5 million] 2.1 million [1.9 million – 2.4 million] 1.9 million [1.7 million – 2.1 million] [ – ] 1.5 million [1.4 million – 1.7 million] 1.3 million [1.2 million – 1.5 million] [ – ] People newly infected. with HIV in AIDS deaths in")
14
Adults and children estimated to be living with HIV2013
Eastern Europe & Central Asia 1.1 million [ – 1.3 million] North America and Western and Central Europe 2.3 million [2.0 million – 3.0 million] Middle East & North Africa [ – ] Caribbean [ – ] Asia and the Pacific 4.8 million [4.1 million – 5.5 million] Sub-Saharan Africa 24.7 million [23.5 million – 26.1 million] Latin America 1.6 million [1.4 million – 2.1 million] Total dec 2013: 35.0 million [33.2 million – 37.2 million]

16
Tot 2015: 78 miljoen mensen geïnfecteerd, 40 miljoen overleden, situatie 2015:
1. Zuid Afrika Nigeria India Kenya, Mozambique, Uganda Tanzania, Zimbabwe Zambia

17
CDC definitie Stage A: asymptomatic Stage B: minor complications
Stage C: AIDS indicator diseases 1: >500 CD4 cells 2: CD4 cells 3: <200 CD4 cells

18
Viral load en CD4 bepalen de uitkomst

19
Behandeling Grote doorbraak 1996!, in arme landen pas zeer geleidelijk vanaf 2001

20
Mortality in patients with CD4<100 of antiretroviral (ARV) therapy including a protease inhibitor among those patients, USA, 1994–1997 40 100 80 30 Deaths per 100 person years 60 inhibitors (% of patient days) 20 ARV therapy including protease 40 Deaths ARV 10 20 1994 1995 1996 1997 Source: Palella et al., New England Journal of Medicine, 1998 Mar, 26:338–60 98036-E-35 – 15 July 1998
 20. ARV therapy including protease. 40. Deaths. ARV Source: Palella et al., New England Journal of Medicine, 1998 Mar, 26:338– E-35 – 15 July")
21
Nieuw richtlijnen voor gebruikl ARVs voor behandeling en preventie HIV-infectie
“rijke landen”: c-ART should be offered to all patients with HIV-infection, even with CD4 > 500 “Resource limited countries”: new WHO guideline from June 2013 is getting close to that of high income countries

22
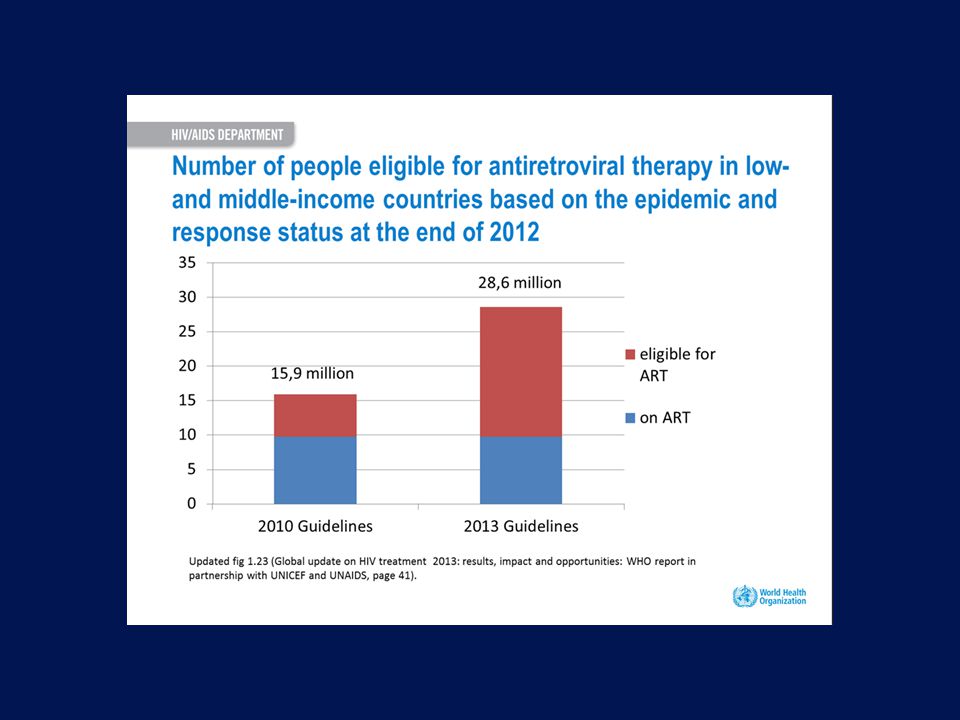
Verandering WHO richtlijnen tussen 2006 en 2013: gebaseerd op CD4
2006: < 200 2010: < 350 2013: < 500 (prioriteit < 350 en stadium 3 / 4)
")
23
Verandering richtlijnen voor zwangere vrouwen en tijdens borstvoeding
2010: start ART with CD4 < 350 or stage 3 / 4 disease 2013: initiate ART regardless of CD4 and clinical stage

24
2013 –initiate ART regardless of WHO clinical stage and CD4 cell count adults and adolescents> 10 years Active TB disease HBV coinfection with severe chronic liver disease Pregnant and breastfeeding women with HIV HIV-positive individual in a serodiscordant partnership

25
Cohen, NEJM 2011; 365: Behandeling is ook preventie! Een van de belangrijkste studies van de laatste 10 jaar 1763 “disconcordant” couples from US, Africa, India, Brazil 886 start c-ART immediately (CD ) 870 delayed arm: <250 CD4 and/or complaints In early arm: 4 transmissions In delayed arm: 35 transmissions Early c-ART: 96% reduction of transmissions!!
 870 delayed arm: <250 CD4 and/or complaints. In early arm: 4 transmissions. In delayed arm: 35 transmissions. Early c-ART: 96% reduction of transmissions!!")
26
Preventie Preventie moeder-kind overdracht: alle zwangere vrouwen behandelen met volledige HIV- behandeling Vroege start HIV-behandeling Sexuele overdracht - condoom - circumcisie - systemisch Prep ? Verschil man/vrouw - vaginale gel met tenofovir?

27
Aandachtspunten voor reizigers naar de tropen
Vermijd onbeschermde seks in HIV-endemische landen Gezondheidswerkers werkend in HIV-endemische landen: wees alert voor prikaccidenten en vraag advies betr. PEP (HIV-remmers mee) indien locaal niet aanwezig Hoog risico groep: MSM Waarschuw voor last minute reis zonder vaccinatie en zonder malaria profylaxe
 indien locaal niet aanwezig. Hoog risico groep: MSM. Waarschuw voor last minute reis zonder vaccinatie en zonder malaria profylaxe.")
29
29

30
Children (<15 years) estimated to be living with HIV2013
Eastern Europe & Central Asia 14 000 [ – ] North America and Western and Central Europe 2800 [2300 – 3600] Middle East & North Africa 16 000 [ – ] Caribbean 17 000 [ – ] Asia and the Pacific [ – ] Sub-Saharan Africa 2.9 million [2.6 million – 3.2 million] Latin America 35 000 [ – ] Total: 3.2 million [2.9 million – 3.5 million]

31
Estimated adult and child deaths from AIDS2013
Eastern Europe & Central Asia 53 000 [ – ] North America and Western and Central Europe 27 000 [ – ] Middle East & North Africa 15 000 [ – ] Caribbean 11 000 [8300 – ] Asia and the Pacific [ – ] Sub-Saharan Africa 1.1 million [1.0 million – 1.3 million] Latin America 47 000 [ – ] Total: 1.5 million [1.4 million – 1.7 million]

32
Estimated number of adults and children newly infected with HIV2013
Eastern Europe & Central Asia [ – ] North America and Western and Central Europe 88 000 [ – ] Middle East & North Africa 25 000 [ – ] Caribbean 12 000 [9400 – ] Asia and the Pacific [ – ] Sub-Saharan Africa 1.5 million [1.3 million – 1.6 million] Latin America 94 000 [ – ] Total: 2.1 million [1.9 million – 2.4 million]

33
About 6 000 new HIV infections a day in 2013
About 68% are in Sub Saharan Africa About 700 are in children under 15 years of age About are in adults aged 15 years and older, of whom: ─ almost 47% are among women ─ about 33% are among young people (15-24)
")
34
2013 global HIV and AIDS estimates Children (<15 years)
Children living with HIV 3.2 million [2.9 million – 3.5 million] New HIV infections in [ – ] Deaths due to AIDS in [ – ]

35
2 million people newly enrolled on antiretroviral treatment in 2013 – the largest ever annual increase

37
23% of children in need received treatment in 2013 as compared to 37% for adults, pointing to a larger gap between services for adults and children living with HIV

Verwante presentaties








>")










