Download de presentatie
De presentatie wordt gedownload. Even geduld aub

1
Vroeg versus laat ontstane vorm van de ziekte van Alzheimer
Piet Eikelenboom Psychiatrie, VUMC, Amsterdam Neurologie, AMC, Amsterdam Apeldoorn, 5 juli 2012

3
Clinical symptoms of Auguste D
51 years old woman with paranoid symptoms and memory disturbances During hospitalisation desorientation in time and space, severe impairment to learn new information, language problems, apraxia. Terrific crying for hours, hallucinations, delirious episodes. Progressive dementia and death 4,5 years after admission

5
Neuro

6
USA: Veranderde zienswijze NIA omstreeks 1978.
Ziekte van Alzheimer van een neuropathologische diagnose tot een klinische label Britse bijdrage: Roth, Tomlinson Blessed jaren vijftig en zestig vorige eeuw USA: Veranderde zienswijze NIA omstreeks 1978.

7
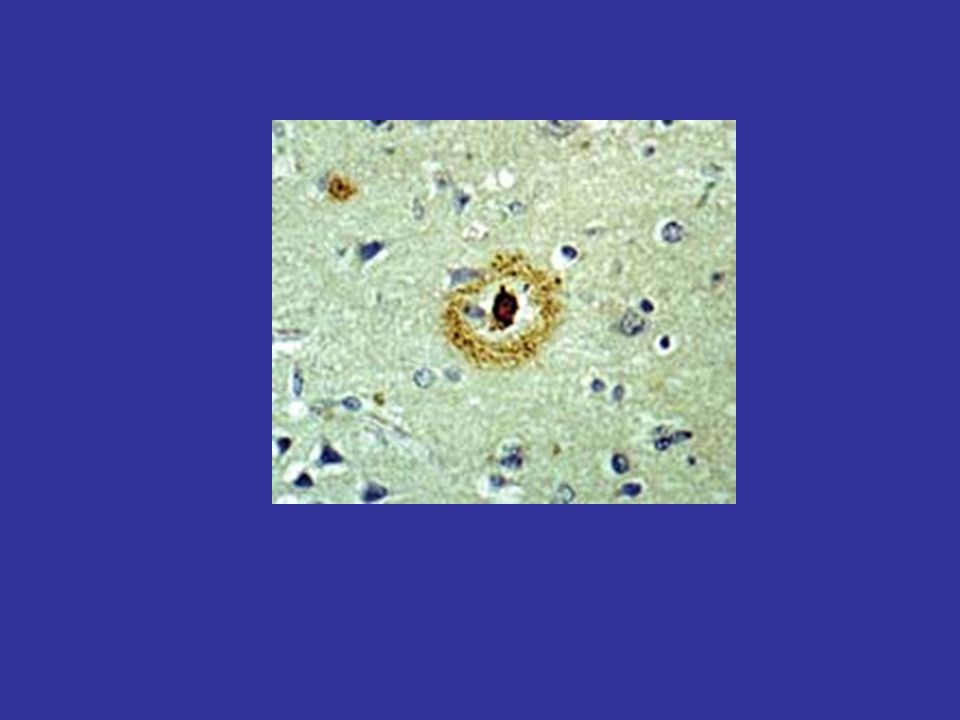
ALZHEIMER’S DISEASE NEUROPATHOLOGICAL HALLMARKS
Links : immuno met polyclonaal (konijn) anti- Aß Linksboven: verschillende elementen kleuren aan met anti – Aß: “klassieke”neuritische plaque met core en corona; rechtsonder (hoogstwaarschijnlijk congofiel) vat verdeer wat primitieve Aß plaques. rechts : AT 8 immuno Dystrofe neurieten in twee plaques zijn AT 8 positief; verder veel neuropil draden en (rechtsboven het midden) een tangle Beide immuno’s op vriescoupe van Temporale schors (T2) van AD geval Extracellular Aß deposits Hyperfosforylated tau
 anti- Aß. Linksboven: verschillende elementen kleuren aan met anti – Aß: klassieke neuritische plaque met core en corona; rechtsonder (hoogstwaarschijnlijk congofiel) vat verdeer wat primitieve Aß plaques. rechts : AT 8 immuno. Dystrofe neurieten in twee plaques zijn AT 8 positief; verder veel neuropil draden en (rechtsboven het midden) een tangle. Beide immuno’s op vriescoupe van Temporale schors (T2) van AD geval. Extracellular Aß deposits. Hyperfosforylated tau.")
8
Doulestaining Congo red and A-beta
AD: Abeta/Congo-red

9
diffuse plaques

10
Cleavage of Amyloid Precursor Protein (APP)
Plasma membrane APP β-secretase γ-secretase α-secretase Aβ40/42

11
Proteinaggregation and fibril formation
monomer low n-oligomer fibrils fibril intermediates

12
Alzheimer’s disease: Amyloid cascade hypothesis
Neurons Amyloid precursor protein Neurofibrillary Tangles Neuronal loss Amyloid Glial cells Diffuse plaque Neuritic plaque bloodvessel 12

13
Amyloid β deposits and Neurofibrillary pathology
Aβ deposits Neurofibrillary tangles Cognitive impairment Clinical diagnosis- death (8 years) Relative occurence Clinicopathological studies suggest that disease duration can be as long as 30 years, while cognitive decline occurs in the last decade. This is a hypothetical scheme based on different pathological studies. Amyloid deposits are observed before the occurence of tangles. When tangles occur also cognitive impairment occurs. This is in line with the amyloid cascade hypothesis, where Abeta precedes the formation of tangles and neuronal loss. 5 10 15 20 25 30 Disease duration (years) I II III IV V VI Neuropathological staging Adapted from Nelson et al., JNEN 2008 13
 Relative occurence. Clinicopathological studies suggest that disease duration can be as long as 30 years, while cognitive decline occurs in the last decade. This is a hypothetical scheme based on different pathological studies. Amyloid deposits are observed before the occurence of tangles. When tangles occur also cognitive impairment occurs. This is in line with the amyloid cascade hypothesis, where Abeta precedes the formation of tangles and neuronal loss Disease duration (years) I. II. III. IV. V. VI. Neuropathological staging. Adapted from Nelson et al., JNEN")
14
CSF markers (tau) and AD
 and AD")
16
De ziekte van Alzheimer en Aβ
Etiologie: stoornis van de Aβ productie Diagnostiek: Beeldvorming Aβ in hersenen en bepaling Aβ en tau in liquor Therapie: remming Aβ productie of stimulering van opruiming.

18
≥ 75 “type II” < 75 “type I” 1.5 1.0 0.5 2005 2015 2025 2035 2045
milllion UK patients 1.5 1.0 ≥ 75 “type II” 0.5 < 75 “type I” 2005 2015 2025 2035 2045 year SOURCE: UK Alzheimer Society

19
Leeftijdsdistributie patiënten met dementie:
in wetenschappelijk onderzoek (6953) in bevolking ( ) 5 10 15 20 25 30 35 60-64 65-69 70-74 75-79 80-84 85-89 90-94 patiënten in onderzoek patiënten in bevolking oververtegenwoordiging ondervertegenwoordiging Lancet Neurology 2004
 in bevolking ( ) patiënten in onderzoek. patiënten in bevolking. oververtegenwoordiging. ondervertegenwoordiging. Lancet Neurology")
20
Klinische verschillen vroeg versus
laat ontstane AD Vroeg ontstaan: In vroegstadium gekenmerkt door visuospatiële symptomen, stoornissen in de uitvoerende functies en van de aandacht. Geheugenfunctie nog relatief gespaard. Laat ontstaan: In vroegstadium staan geheugenstoornissen centraal en minder uitgesproken zijn stoornissen van taal en praxis.

21
Etiologische verschillen in vroeg en laat beginnende vormen van de ziekte van Alzheimer
Vroeg beginnend: bij de familale vorm primaire oorzakelijke factor in stoornis van de Aβ productie Laat ontstaan: (sporadische vorm): multifactorieel bepaald. Risicofactoren: Genetische bijdrage van polymorfisme van lipoproteines en immuunfactoren); vasculaire factoren; metabole factoren.
: multifactorieel bepaald. Risicofactoren: Genetische bijdrage van polymorfisme van lipoproteines en immuunfactoren); vasculaire factoren; metabole factoren.")
22
Neuropsychologisch verschillen in profiel
Diagnostische verschillen in vroeg en laat beginnende vormen van de ziekte van Alzheimer Neuropsychologisch verschillen in profiel Beeldvormend onderoek: meer witte stof patholgie, PET scan voor Aβ overlap niet demente ouderen Liqour: tau en Aβ boven 75 jaar geringe specificteit

23
AD: complement C3d in plaques and vascular amyloid
AD: C3d

24
Microglia in Alzheimer’s disease
HLA-DR and Congo red

25
Aß production/clearance
type I AD Disturbance Aß production causal genes other causes Disbalance Aß production/clearance Aß deposits Vulnerability genes: pro-inflammatoir genotype ApoE, clusterine, CR1 Disturbance Aß clearance Environmental factors Head trauma Vasculair factors type II AD

26
Diabetes, arteriosclerosis en de ziekte van Alzheimer
Vroeg beginnende vormen: stoornissen in de productie van insuline, cholesterol of Aβ zijn primair in de pathogenese Laat ontstane vormen: stoornissen in opruimen van cholesterol en Aβ, en insuline resistentie zijn cruciaal in de pathogense.

27
Laat ontstane sporadische vorm van AD
Gemengde type vasculair en neurodegeneratieve(Alzheimer) karakteristieken. 2. Frequente somatische comorbiditeit (diabetes, vasculaire ziekten) 3. Neuropathologische heterogenteit boven 80 jaar (bijvoorbeeld hippocampale sclerosis).
 karakteristieken. 2. Frequente somatische comorbiditeit (diabetes, vasculaire ziekten) 3. Neuropathologische heterogenteit boven 80 jaar (bijvoorbeeld hippocampale sclerosis).")
28
Vroeg vesus laat onstane beelden.
Vroeg ontstaan orgaan specifiek (bijbvoorbeeld diabetes de pancreas) laat ontstaan meer systeemaandoening met als gemeenschappelijk determinant betrokkenheid metabool syndroom, vasculaire factoren en de aangeboren immuniteit.
 laat ontstaan meer systeemaandoening met als gemeenschappelijk determinant betrokkenheid metabool syndroom, vasculaire factoren en de aangeboren immuniteit.")
29
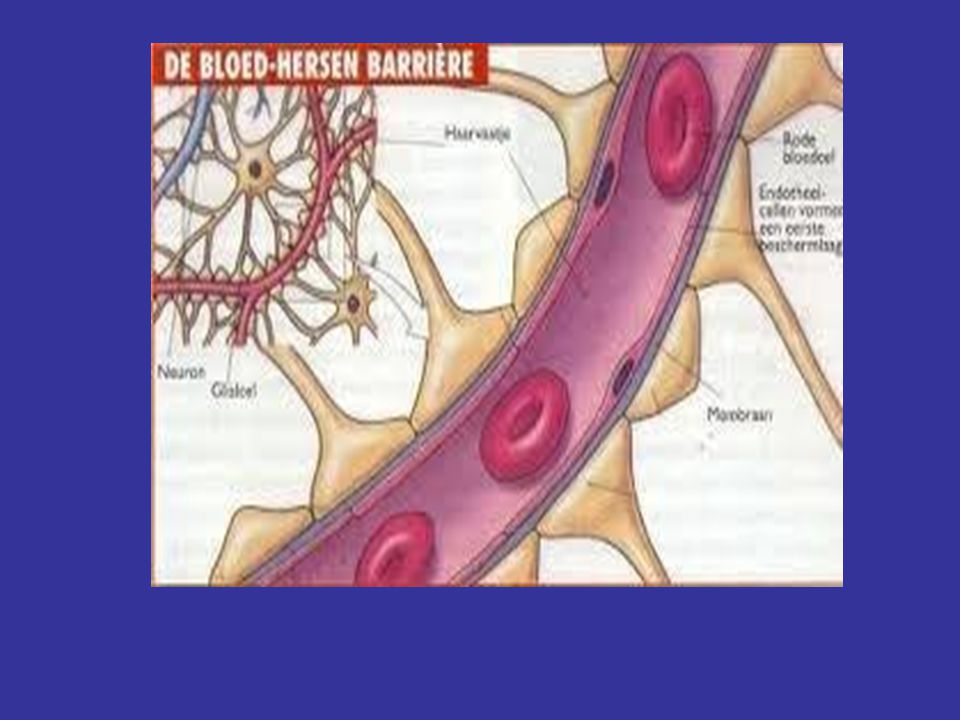
De hersenen als de zetel van psychiatrische stoornissen
de bloed-hersen barriere

33
Aangeboren immuniteit Verworven immuniteit
humoraal cellulair humoraal cellulair complement macofagen lymfocyten antilichamen cytokines

34
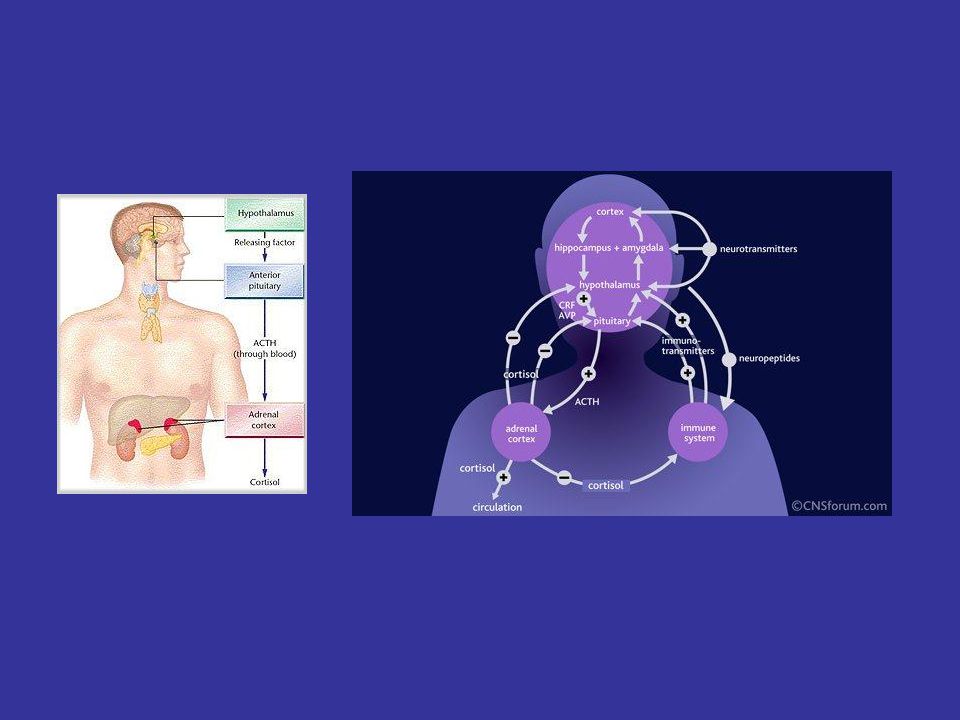
Dementie, delier en depressie - Aangeboren immuniteit - HPA-as - metabole factoren

35
Zijn wij onze hersenen of ons lijf?

36
Dementie, delier en depressie - Depressie en dementie (Paul Naarding) - Delier en dementie (Barbara van Munster)
 - Delier en dementie (Barbara van Munster)")
37
many aetiological factors
delirium ACh Cortical cholinergic projections originate in the basal forebrain, specifically the nucleus basalis of Meynert and the substantia innominata, and they terminate in almost all cortical areas and layers. Rather than serving specific instrumental cortical functions, this diffusely organised cortical input system serves the more fundamental role of detection, selection, discriminating and processing of sensory stimuli and higher processes. Substantial evidence has accumulated in support of the notion that demands in attentional processing are mediated via cortical cholinergic inputs. Deficiencies in these inputs impair discriminatory processes, the efficiency of cortical processing and responsiveness to relevant and new stimuli. Symptom profiles of neurodegenerative diseases affecting the cholinergic system are not very well suited to define exactly the functional consequences of cholinergic impairment, because these effects are difficult to separate from additional neuropathological ramifications that are sometimes only partially known. IL-1 IL-6 TNF many aetiological factors

38
Conclusies - Ouderenpsychiatrie van emancipatie ( ) naar specifieke deskundigheid ( Ontwikkeling laatste jaren (de oudste ouderen) a) verschillen tussen vroeg en laat onstane vormen b) klinische samenhang van comorbide laat ontstane stoornissen c) de pathogenetische samenhang (meer systeemziekten dan lokale orgaanpathologie). d) consequenties voor diagnostiek en behandeling) -
 consequenties voor diagnostiek en behandeling) -.")
Verwante presentaties














to watch throughout the month of August,>")





