Download de presentatie
De presentatie wordt gedownload. Even geduld aub

1
Relevantie van observationeel onderzoek in de klinische praktijk
Themabijeenkomst “observationeel onderzoek” 20 september 2005

2
Nederlandse Coöperatieve Studie naar de Adequaatheid van Dialyse

3
Presentatie NECOSAD Mogelijkheden observationeel onderzoek; voorbeelden: - HD versus PD - Vroege versus late start - Dialysedosis PD Conclusies

4
NECOSAD Initiatief van de Dialyse Groep Nederland (DGN)
Eerste ideeën 1991 NECOSAD-1 (pilot-studie) NECOSAD-2 Uitgevoerd in 38 dialysecentra Gefinancierd door de Nierstichting en de Ziekenfondsraad
 NECOSAD-2. Uitgevoerd in 38 dialysecentra. Gefinancierd door de Nierstichting en de. Ziekenfondsraad.")
5
Organisatie NECOSAD Begeleidingscommissie Raad van Toezicht
Dr. A. J. Apperloo, Dr. J. N. M. Barendrecht, Dr. R. J. Birnie, Dr. M. Boekhout, Dr. W. H. Boer, Dr. E. F. H. van Bommel, Prof. Dr. H. R. Büller, F. Th. de Charro, Dr. C. J. Doorenbos, Dr. W. T. van Dorp, Dr. A. van Es, Dr. W. J. Fagel, Dr. G. W. Feith, Dr. C. F. M. Franssen, Dr. L. A. M. Frenken, Dr. J. A. C. A . van Geelen, Dr. P. G. G. Gerlag, Drs. J. P. M. C. Gorgels, Dr. W. Grave, Dr. R. M. Huisman, Dr. K. J. Jager, Dr. K. Jie, Drs. W. A.. H. Koning-Mulder, Dr. M. I. Koolen, Dr. T. K. Kremer Hovinga, Drs. A. T. J. Lavrijssen, Dr. A. W. Mulder, Dr. K. J. Parlevliet, Dr. J. L. C. M. van Saase, Drs. M. J. M. Schonk, Dr. M. M. J. Schuurmans, Prof. Dr. J. G. P. Tijssen, Dr. R. M. Valentijn, Dr. GH Vastenburg, Dr. C. A. Verburgh, Dr. V. M. C. Verstappen, Dr. H. H. Vincent, Dr. P. Vos. Raad van Toezicht Prof. dr. G. K. van der Hem Prof. dr H. A. Koomans Prof. dr. K. M. L. Leunissen Dr. R. van Leusen Projectleiding Dr. E. W. Boeschoten Dr. F. W. Dekker Prof. dr. R. T. Krediet Onderzoeksverpleegkundigen NECOSAD NECOSAD – verpleegkundigen in de centra

6
Doelstellingen NECOSAD
Analyse van de factoren die de uitkomst van de dialysebehandeling in Nederland bepalen Toetsen en ontwikkelen van richtlijnen voor een optimale behandeling Bijdragen aan de kwaliteit van de behandeling door terugkoppeling van centrumgebonden resultaten en het ontwikkelen van benchmarks

7
Studieopzet van NECOSAD
Prospectieve observationele multi-center cohort studie bij incidente volwassen dialysepatiënten. Binnen dit cohort gerandomiseerde trial HD versus PD

8
Gegevensverzameling 4 - 0 weken voor de start:
demografie, poliklinische voorbereiding, starttherapie (+ reden), primaire nierziekte, co-morbiditeit, rookgewoonten, lengte, gewicht, RR, medicijngebruik, albumine, ureum, creatinine, GFR, kwaliteit van leven 0, 3, 6, 12, 18…..maanden dialysemodaliteit, therapiewisselingen, registratie op wachtlijst NTx, gewicht, RR, voedingstoestand, medicijngebruik, opnames, lab., dialysedosis, rGFR, Karnofsky-index, KvL.
, primaire nierziekte, co-morbiditeit, rookgewoonten, lengte, gewicht, RR, medicijngebruik, albumine, ureum, creatinine, GFR, kwaliteit van leven. 0, 3, 6, 12, 18…..maanden. dialysemodaliteit, therapiewisselingen, registratie op wachtlijst NTx, gewicht, RR, voedingstoestand, medicijngebruik, opnames, lab., dialysedosis, rGFR, Karnofsky-index, KvL.")
9
Database Per 01-05-03 ondergebracht bij Hans Mak Instituut

10
Ingevroren materiaal Op elk meetmoment afname van spijtmateriaal (serum, urine en dialysaat) Vanaf 2000 werden ook bloedmonsters voor genotypering ingevroren

11
Inclusion NECOSAD - 2

12
Baseline Characteristics Necosad-2
HD PD Number % 1184 (68) 545 (32) % Male 60 63 Age (sd) 62,1 (14,5) 53,6 (14,6) Prim. Kidney Dis.: Diabetes (%) 15 16 Glomerulonephr. (%) 11 18 Vascular (%) 21 14 Co-morbidity: Low (%) 32 53 Medium (%) 35 29 High (%) 33
 545 (32) % Male Age (sd) 62,1 (14,5) 53,6 (14,6) Prim. Kidney Dis.: Diabetes (%) Glomerulonephr. (%) Vascular (%) Co-morbidity: Low (%) Medium (%) High (%) 33.")
13
Presentatie NECOSAD Mogelijkheden observationeel onderzoek; voorbeelden: - HD versus PD - Vroege versus late start - Dialysedosis PD Conclusies

14
Survival in HD and PD Several studies show small and opposing differences between HD and PD for survival and for quality of life Variability - due to methodological differences such as type of statistical models, case-mix and follow-up? - or due to an absence of a true difference between HD and PD ?

16
Design & Aim A randomized controlled trial (RCT) within a prospective cohort Compare survival and quality of life between Hemodialysis and Peritoneal dialysis patients In an effort to improve the quality and outcomes of dialysis care, the National Kidney Foundation – Dialysis Outcomes Quality Initiative was established. In 1997 practical guidelines for the initiation of dialysis were published (AJKD 1997) by the PD work group. However, before we can implement these guidelines into daily practice we have to be aware that, as DOQI stated itself, this guideline is purely opinion based. Implementation of this guideline would require an earlier start than usual in dialysis practice. This would have impact on daily life of patients and on dialysis recourses and costs Thus before implementation, it is essential to evaluate the benefit of this guideline against its negative aspects.
 by the PD work group. However, before we can implement these guidelines into daily practice we have to be aware that, as DOQI stated itself, this guideline is purely opinion based. Implementation of this guideline would require an earlier start than usual in dialysis practice. This would have impact on daily life of patients and on dialysis recourses and costs. Thus before implementation, it is essential to evaluate the benefit of this guideline against its negative aspects.")
17
Study design Patients without medical, social or logistic objections were invited Patients were educated about HD and PD Informed consent Patients were randomized by telephone service: HD or PD Patients were treated according to usual local care All consecutive new ESRD patients starting with chronic dialysis treatment in 29 Dutch centres who: New on chronic dialysis treatment, thus never had renal replacement therapy before Patients had to be 18 years or older

18
Study design Primary outcome: QALY in first 2 years
QALY: quality of the time spent on dialysis Patients evaluated their own quality with EuroQol All consecutive new ESRD patients starting with chronic dialysis treatment in 29 Dutch centres who: New on chronic dialysis treatment, thus never had renal replacement therapy before Patients had to be 18 years or older

19
EuroQol Best imaginable state Worst imaginable state 100 80 60 40 20
All consecutive new ESRD patients starting with chronic dialysis treatment in 29 Dutch centres who: New on chronic dialysis treatment, thus never had renal replacement therapy before Patients had to be 18 years or older

20
Example: QALY-scores after 2-yrs.
80.0 55.0 † 20.6

21
Study design Difference of 10 QALY-points clinical relevant
Calculated sample size: 100 patients 50 HD patients 50 PD patients All consecutive new ESRD patients starting with chronic dialysis treatment in 29 Dutch centres who: New on chronic dialysis treatment, thus never had renal replacement therapy before Patients had to be 18 years or older

22
Trial profile

23
Trial profile

24
Mean (SD) QALY-scores after 2 yrs. i.t.t.
HD patients: 59.1 (11.7) PD patients: 54.0 (18.9) Difference HD and PD: (p = 0.41) Difference after adjustment: (p = 0.63) (adjusted for: age, comorbidity, primary kidney disease) Some of the basic characteristics of our population No difference in age or sex Of course a difference in renal Kt/V and nPNA, that is due to the definition of late and timely Noticeable is the fact that no difference in Body mass Index was observed although this is included in the classification of patients in late or timely, apparently this parameter does not play a important role in the classification, Comorbidity was classified according to classification of Kahn. No difference in comorbidity
 PD patients: 54.0 (18.9) Difference HD and PD: 5.1 (p = 0.41) Difference after adjustment: 2.1 (p = 0.63) (adjusted for: age, comorbidity, primary kidney disease) Some of the basic characteristics of our population. No difference in age or sex. Of course a difference in renal Kt/V and nPNA, that is due to the definition of late and timely. Noticeable is the fact that no difference in Body mass Index was observed although this is included in the classification of patients in late or timely, apparently this parameter does not play a important role in the classification, Comorbidity was classified according to classification of Kahn. No difference in comorbidity.")
25
Deceased after 5-year follow-up
Years Total HD (50%) PD (25%) Some of the basic characteristics of our population No difference in age or sex Of course a difference in renal Kt/V and nPNA, that is due to the definition of late and timely Noticeable is the fact that no difference in Body mass Index was observed although this is included in the classification of patients in late or timely, apparently this parameter does not play a important role in the classification, Comorbidity was classified according to classification of Kahn. No difference in comorbidity
 PD (25%) Some of the basic characteristics of our population. No difference in age or sex. Of course a difference in renal Kt/V and nPNA, that is due to the definition of late and timely. Noticeable is the fact that no difference in Body mass Index was observed although this is included in the classification of patients in late or timely, apparently this parameter does not play a important role in the classification, Comorbidity was classified according to classification of Kahn. No difference in comorbidity.")
26
Survival (i.t.t.)
")
27
Hazard ratio’s after 5 years follow-up i.t.t.
Adjusted hazard ratio’s. Adjusted for: age, sex, pn, and comorbidity. We do see a significant higher risk of mortality for a late start: RR 2.11, the effect of this increased risk is mainly due to the level of residual renal function (ktv or gfr) and in to a lesser extend due to estimated protein intake. We see a lover mortality risk for timely starters, but how large is this gain in survival ?
 and in to a lesser extend due to estimated protein intake. We see a lover mortality risk for timely starters, but how large is this gain in survival")
28
Number changed modality after 5-yr follow-up
Years Total HD (11%) PD (35%) Some of the basic characteristics of our population No difference in age or sex Of course a difference in renal Kt/V and nPNA, that is due to the definition of late and timely Noticeable is the fact that no difference in Body mass Index was observed although this is included in the classification of patients in late or timely, apparently this parameter does not play a important role in the classification, Comorbidity was classified according to classification of Kahn. No difference in comorbidity
 PD (35%) Some of the basic characteristics of our population. No difference in age or sex. Of course a difference in renal Kt/V and nPNA, that is due to the definition of late and timely. Noticeable is the fact that no difference in Body mass Index was observed although this is included in the classification of patients in late or timely, apparently this parameter does not play a important role in the classification, Comorbidity was classified according to classification of Kahn. No difference in comorbidity.")
29
Conclusions from the RCT HD versus PD
In terms of QALY scores HD and PD are equivalent Better survival on PD compared to HD over the first 5 years in i.t.t. analysis Incident dialysis patients may benefit from starting on PD

30
Termorshuizen et al. Hemodialysis and peritoneal dialysis: comparison of adjusted mortality rates according to the duration of dialysis: analysis of the NECOSAD 2 study. JASN 2003;14: Design & Aim Prospective cohort study of patients new on dialysis treatment Compare mortality rates between HD and PD patients In an effort to improve the quality and outcomes of dialysis care, the National Kidney Foundation – Dialysis Outcomes Quality Initiative was established. In 1997 practical guidelines for the initiation of dialysis were published (AJKD 1997) by the PD work group. However, before we can implement these guidelines into daily practice we have to be aware that, as DOQI stated itself, this guideline is purely opinion based. Implementation of this guideline would require an earlier start than usual in dialysis practice. This would have impact on daily life of patients and on dialysis recourses and costs Thus before implementation, it is essential to evaluate the benefit of this guideline against its negative aspects.
 by the PD work group. However, before we can implement these guidelines into daily practice we have to be aware that, as DOQI stated itself, this guideline is purely opinion based. Implementation of this guideline would require an earlier start than usual in dialysis practice. This would have impact on daily life of patients and on dialysis recourses and costs. Thus before implementation, it is essential to evaluate the benefit of this guideline against its negative aspects.")
31
Patient characteristics – 3 months
Some of the basic characteristics of our population No difference in age or sex Of course a difference in renal Kt/V and nPNA, that is due to the definition of late and timely Noticeable is the fact that no difference in Body mass Index was observed although this is included in the classification of patients in late or timely, apparently this parameter does not play a important role in the classification, Comorbidity was classified according to classification of Kahn. No difference in comorbidity * p<0.05 HD vs PD

32
Patient characteristics (cont’d)
Some of the basic characteristics of our population No difference in age or sex Of course a difference in renal Kt/V and nPNA, that is due to the definition of late and timely Noticeable is the fact that no difference in Body mass Index was observed although this is included in the classification of patients in late or timely, apparently this parameter does not play a important role in the classification, Comorbidity was classified according to classification of Kahn. No difference in comorbidity * p<0.05 HD vs PD

33
Unadjusted death rates and RR of death HD – PD cohort study

34
Multivariate analysis HD compared with PD Adjusted for: ( age, gender, comorbidity, prim kidney dis, SGA, Hb, Alb, renal Kt/v baseline) Time period (mo) as treated ITT Adj HR % CI 3 to 12 – 2.50 – 2.18 12 to 24 – 1.77 – 1.72 24 to 36 – 0.91 – 0.87 36 to 48 – 0.57 – 0.73
 as treated. ITT. Adj HR 95% CI. 3 to – – to – – to – – to – –")
35
Conclusions from the prospective cohort study
During the first 2 years lower mortality rates in PD patients < 60 yr After 2 years tendency towards greater relative mortality rates for PD patients, especially in PD patients > 60 yr Indication of a survival benefit of long-term PD patients after switching to HD

36
From: Lysacht M et al. ASAIO Trans, 1991

37
Significant risk factors for the decline of GFR during the 1st year on dialysis
relative risk effect on index GFR (mL/min) HD vs PD Diastolic BP (10 mm Hg ) Proteinuria (g/day) From: Jansen MAM et al. Kidney Int, 2002
 HD vs PD Diastolic BP. (10 mm Hg ) Proteinuria. (g/day) From: Jansen MAM et al. Kidney Int,")
38
Dialysis related mechanisms responsible for the decline in rGFR (adjusted for baseline GFR, age, sex, PKD, comorbidity) ß p HD: hypotensive episodes PD: dehydration Jansen et al KI 2002;62:

39
Presentatie NECOSAD Mogelijkheden observationeel onderzoek; voorbeelden: - HD versus PD - Vroege versus late start - Dialysedosis PD Conclusies

40
Lancet 2001:358:

41
NECOSAD analysis Korevaar et al Lancet 2001;358:1046-1050
Consecutive new ESRD patients > 18 yrs in 29 dialysis centres Exclusion of patients without predialysis care and with malignancies GFR 0-4 weeks before start dialysis Timely start defined according to DOQ1

42
Initiation guideline DOQI Am J Kidney Dis 1997
Timely initiation 1. renal Kt/Vurea 2.0/week 2. Renal Kt/Vurea < 2.0, but BMI 20 kg/m² and nPNA 0.8/kg/day Late initiation: all other patients

43
Patient characteristics at start
late (n=94) timely (n=159) age (yrs) male (%) BMI (kg/m²) GFR (ml/min/1.73 m³) * Kt/Vurea (per week) * % HD * = p < 0.05
 timely (n=159) age (yrs) male (%) BMI (kg/m²) GFR (ml/min/1.73 m³) * Kt/Vurea (per week) * % HD * = p <")
45
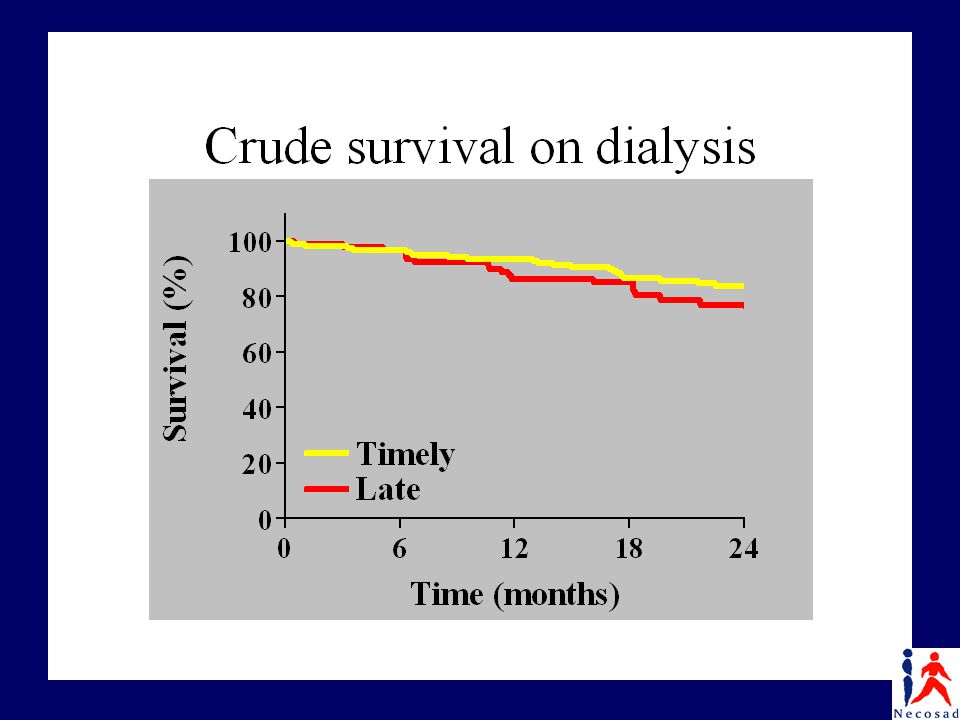
Comparison between timely and late starters
Timely starters have a 2.5 month longer survival on dialysis after 3 years, but Timely starters begin dialysis 4.1 to 8.3 months earlier in the time course of their disease No effect of an early start of dialysis on survival

46
Comparison between timely and late starters
No effect of a timely start of dialysis on survival Effect on quality of life?

47
Korevaar et al Am J Kidney Dis 2002;39:108-115

48
Conclusions Early start of dialysis
NKF-DOQI targets on the start of dialysis were not evidence based An earlier start of chronic dialysis in patients with end-stage renal disease than currently applied in developed countries is not warranted

49
Presentatie NECOSAD Mogelijkheden observationeel onderzoek; voorbeelden: - HD versus PD - Vroege versus late start - Dialysedosis PD Conclusies

50
Ademex study (Paniagua R. et al. J Am Soc Nephrol, 2002)
965 Mexican patients with peritoneal creatinine clearance < 60 L/week/1.73 m2. Control: 4 x 2L CAPD treated: pCCr > 60 L/week/1.73 m2. No differences in baseline characteristics. Minimum follow-up: 2 years.

51
ADEMEX: Treatment Characteristics
Mean Difference Averaged Across the Study: 11 L/week/1.73 (57L vs 46L) 11% Control vs. 59% Treated achieved pCCr>60 L/week/1.73 at least once during the study p<.001
 11% Control vs. 59% Treated achieved pCCr>60 L/week/1.73 at least once during the study. p<.001.")
52
ADEMEX: Primary Outcome
Control: 1-Yr Survival=85.5%, 2-Yr Survival=68.3% Treated: 1-Yr Survival=83.9%, 2-Yr Survival=69.3% RR(Treated:Control)=1.00 95% CI: (0.80, 1.24)
= % CI: (0.80, 1.24)")
53
Conclusion ADEMEX No difference in survival between patients having a weekly creatinin clearance < 60L/week and > 60L/week What should the minimal target be?

54
PD adequacy - Necosad

55
PD adequacy - NECOSAD Inclusion:
PD patients 3-months after the start of dialysis treatment Age > 18 years Informed consent Chronische of systemische inflammatie is iets wat veel voorkomt bij dialyse patiënten, volgens de literatuur komt dit bij 35 tot 65% van de dialyse patiënten voor. Maar wat is inflammatie eigenlijk. We weten allemaal dat als je je per ongeluk snijd in de keuken dat daar dan een respons op volgt, zodanig dat de beschadiging weer herstelt wordt en eventuele antilichamen te elimineren. Dit wordt klinisch zichtbaar door roodheid, zwelling, pijn en warmte. Dit is een tijdelijke reactie, waarbij stoffen vrijkomen die voor deze processen zorgen, de zgn inflammatoire mediatoren. Wanneer deze stoffen erin slagen om de ontsteking te elimineren, verdwijnen deze inflammatoire mediatoren. Echter, wanneer de aanmaak van inflammatoire mediatoren doorgaat zonder hele duidelijke stimulus, spreken we van chronische inflammatie

56
Patient characteristics (N=413)
")
57
Follow-up

58
Survival 1.07: on average increase of 4 mg/L 32 %

59
Unfavourable effect Favourable effect
effect on QOL * * *

60
Anuric PD patients (N=130)
")
61
Anuric patients* * Adjusted for age, time on dialysis, comorbidity, SGA, serum albumin, hemoglobin ref

62
Anuric patients –cut off point: 1.7
* Adjusted for age, time on dialysis, comorbidity, SGA, serum albumin, hemoglobin ref

63
Anuric patients – 2 cut off points
* Adjusted for age, time on dialysis, comorbidity, SGA, serum albumin, hemoglobin ref ref

64
PD adequacy All PD pts: No effect of dialysis dose on mortality or on QOL Effect of residual renal function on mortality and QOL Anuric patients: Kt/V ≤ 1.5 → increased mortality risk

65
Presentatie NECOSAD Mogelijkheden observationeel onderzoek; voorbeelden: - HD versus PD - Vroege versus late start - Dialysedosis PD Conclusies

66
Hierarchy of study designs (Levels of evidence)
Randomized Controlled Trial Prospective cohort Retrospective cohort … A critical view on epidemiological studies always begins with the study designs used. You all know there are several studydesigns possible, with a certain hierarchy. It has been referred to as levels of evidence, and in the context of effects of therapy we have the RCT as the design providing the strongest evidence. Less strong evidence is produced by cohort studies, by case control studies, or by case reports. Now the main purpose of randomization is to prevent selection bias. When comparing PD to hemodialysis, randomization would be extremely important, as we all know that without randomization we select completely different patients for hemo than for PD. Main purpose of randomization is to prevent selection bias (=confounding by indication or prognosis)
")
67
Conclusions In many clinical situations RCT’s are very difficult to perform because of obvious ethical reasons Therefore observational studies have to provide the evidence Carefully designed large prospective controlled cohort studies with wide variations in patient- and treatment characteristics are required.

Verwante presentaties



![Deltion College Engels C1 Gesprekken voeren [Edu/002]/ subvaardigheid lezen thema: Order, order…. can-do : kan een bijeenkomst voorzitten © Anne Beeker.](/8/2048322/big_thumb.jpg "Deltion College Engels C1 Gesprekken voeren [Edu/002]/ subvaardigheid lezen thema: Order, order…. can-do : kan een bijeenkomst voorzitten © Anne Beeker.>")













 DIAGNOSTIEK MONITORING ICD’S EN BIVENTRICULAIRE PACING PLOTSE DOOD.>")

