Download de presentatie
De presentatie wordt gedownload. Even geduld aub

1
uw welzijn verdient onze beste zorg
Het XYZ van HCV en HP Dodonaeus 2012 Lode Van Overbeke uw welzijn verdient onze beste zorg

2
XYZ van HCV

3
HCV : waar stonden we ? Therapie: Duur - Slaagpercentages
Pegylated interferon, 1 x sc per week Ribaverine 200 mg, à 3 co per dag Duur - Slaagpercentages Type 1 : 48 weken - 50% Type 2 en 3 : 24 weken – 80 % (Type 4 en 5 en 6 : 48 weken %)
")
4
Zomer 2012: protease inhibitoren

5
Protease inhibitoren Enkel voor type 1
Triple-therapie : geassocieerd aan ‘back-bone’ Peginterferon sc 1 x per week Ribaverine 200 mg, 2 – 2à3 co per dag Slaagpercentage naar70% Welke Telaprevir (Incivek® Janssen) Boceprevir (Victrelis® MSD) COMPLEX – veel pillen – veel ‘stopping-rules’
 Boceprevir (Victrelis® MSD) COMPLEX – veel pillen – veel ‘stopping-rules’")
6
Telaprevir Boceprevir
750mg (twee 375mg co) peroraal 3 x daags met (vettig) eten geen lead-in Gedurende 12 weken met Peg-IFN/RBV Bijkomende 12 or 36 weken Peg- IFN/RBV 800mg (vier 200mg co) peroraal 3 x daags met eten 4-weken Peg-IFN/RBV lead-in Gedurende 24, 32 of 44 weken met Peg-IFN/RBV Bijkomende 12 weken Peg-IFN/RBV zo stop BOC op Week 36 Telaprevir/boceprevir dosis mag niet gereduceerd of herstart éénmaal gestopt Peg-IFN: peginterferon; RBV: ribavirin
 peroraal 3 x daags met (vettig) eten. geen lead-in. Gedurende 12 weken met Peg-IFN/RBV. Bijkomende 12 or 36 weken Peg- IFN/RBV. 800mg (vier 200mg co) peroraal 3 x daags met eten. 4-weken Peg-IFN/RBV lead-in. Gedurende 24, 32 of 44 weken met Peg-IFN/RBV. Bijkomende 12 weken Peg-IFN/RBV zo stop BOC op Week 36. Telaprevir/boceprevir dosis mag niet gereduceerd of herstart éénmaal gestopt. Peg-IFN: peginterferon; RBV: ribavirin.")
7
Telaprevir Non-cirrhotic naïves and relapsers achieving undetectable HCV RNA at Week 4 and 12 (eRVR) STOP Telaprevir + PR PR PR Non-cirrhotic naïves and relapsers without eRVR Partial and null responders Patients with cirrhosis Weeks 4 12 24 36 48 HCV RNA If >1000 IU/mL at Week 4 or 12: discontinue all drugs If detectable at Week 24 or 36: discontinue PR

8
Boceprevir STOP BOC + PR BOC + PR* PR BOC + PR
Treatment-naïve without cirrhosis who achieve undetectable HCV RNA at Weeks 8 and 24 PR lead-in BOC + PR BOC + PR* PR Non-cirrhotic treatment-naïve with detectable HCV RNA at Week 8 but undetectable at Week 24* Non-cirrhotic relapsers and partial responders BOC + PR HCV RNA If ≥100 IU/mL discontinue all drugs If detectable discontinue all drugs Null responders Patients with cirrhosis 4 8 12 24 28 28 36 48 Weeks *This regimen has only been tested in patients who have failed previous therapy who were late responders

9
Bijwerkingen Peg-IFN/RBV: Bijkomende bijwerkingen
Vermoeidheid, hoofdpijn, nausea, spierpijn, koorts Anaemie en neutropenie Depressie, insomnia, prikkelbaarheid Rash Bijkomende bijwerkingen Telaprevir : rash, jeuk, anaemie, anorectale klachten, nausea en diarree Boceprevir: anaemie, droge huid, dysgeusie, rash , neutropenie

10
Telaprevir - rash Rash Mild Moderate
Monitor for progression or systemic symptoms until the rash is resolved For moderate rash, consider consultation with a specialist in dermatology. For moderate rash that progresses, permanent discontinuation of telaprevir should be considered If the rash does not improve within 7 days following telaprevir discontinuation, ribavirin should be interrupted. Interruption of ribavirin may be required sooner if the rash worsens despite discontinuation of telaprevir Peginterferon alfa may be continued unless interruption is medically indicated For moderate rash that progresses to severe (≥50% body surface area), permanently discontinue telaprevir Mild Moderate Rash Treating patients with mild or moderate rash Use topical corticosteroids* Permitted systemic antihistaminic drugs may be tried for the treatment of associated pruritus Limit exposure to sun/heat and wear loose-fitting clothes *Concomitant use of systemic dexamethasone with telaprevir may result in loss of therapeutic effect of telaprevir. This combination should be used with caution or alternatives should be considered Telaprevir EU SmPC
, permanently discontinue telaprevir. Mild. Moderate. Rash. Treating patients with mild or moderate rash. Use topical corticosteroids* Permitted systemic antihistaminic drugs may be tried for the treatment of associated pruritus. Limit exposure to sun/heat and wear loose-fitting clothes. *Concomitant use of systemic dexamethasone with telaprevir may result in loss of therapeutic effect of telaprevir. This combination should be used with caution or alternatives should be considered. Telaprevir EU SmPC.")
11
TELAPREVIR must not be restarted if discontinued
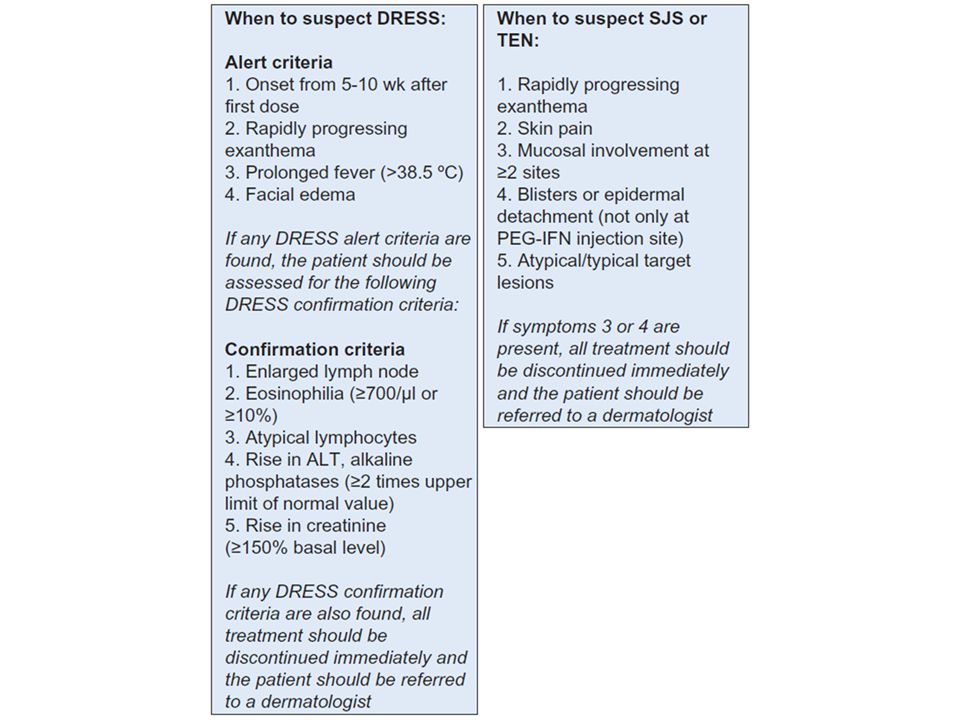
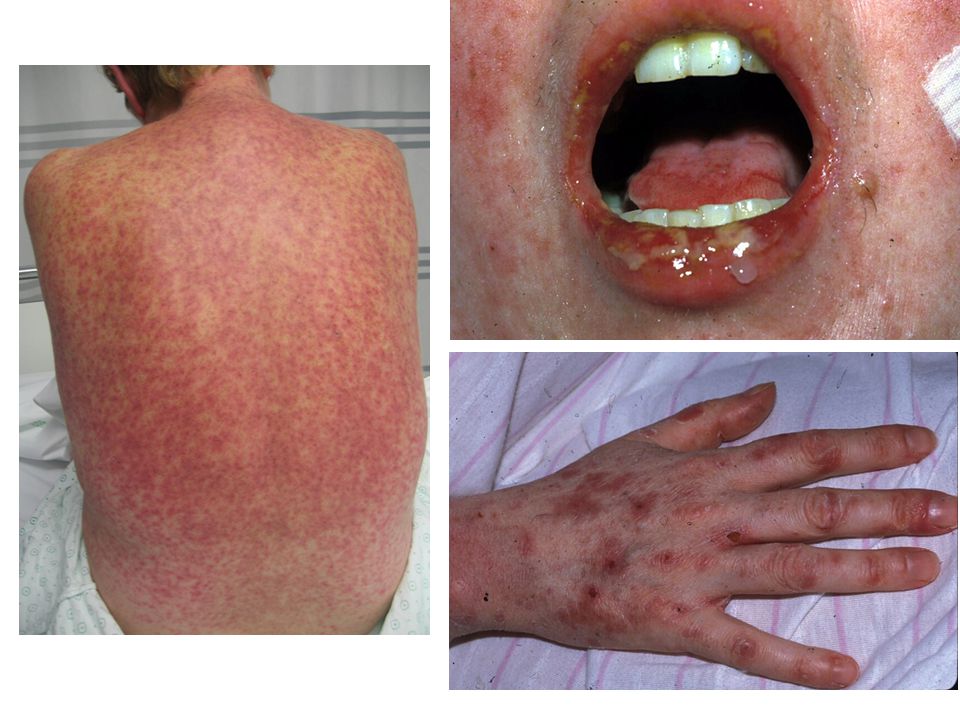
Telaprevir - rash Severe: extent of rash >50% of body surface area or associated with significant systemic symptoms, mucous membrane ulceration, target lesions, epidermal detachment SCAR: generalized bullous eruption, drug rash with eosinophilia and systemic symptoms (DRESS), Stevens-Johnson Syndrome (SJS)/toxic epidermal necrolysis (TEN), acute generalized exanthematous pustulosis (AGEP), erythema multiforme (EM) Permanently discontinue telaprevir immediately. Consultation with a specialist in dermatology is recommended Monitor for progression or systemic symptoms until the rash is resolved. If no improvement within 7 days of stopping telaprevir (or earlier if rash worsens), sequential or simultaneous interruption or discontinuation of ribavirin and/or peginterferon should be considered Rash Severe Permanent and immediate discontinuation of telaprevir, peginterferon and ribavirin is required Consult with a specialist in dermatology SCAR? TELAPREVIR must not be restarted if discontinued Telaprevir EU SmPC
, Stevens-Johnson Syndrome (SJS)/toxic epidermal necrolysis (TEN), acute generalized exanthematous pustulosis (AGEP), erythema multiforme (EM) Permanently discontinue telaprevir immediately. Consultation with a specialist in dermatology is recommended. Monitor for progression or systemic symptoms until the rash is resolved. If no improvement within 7 days of stopping telaprevir (or earlier if rash worsens), sequential or simultaneous interruption or discontinuation of ribavirin and/or peginterferon should be considered. Rash. Severe. Permanent and immediate discontinuation of telaprevir, peginterferon and ribavirin is required. Consult with a specialist in dermatology. SCAR TELAPREVIR must not be restarted if discontinued. Telaprevir EU SmPC.")
14
Boceprevir : anaemie 160 150 140 130 120 110 T12/PR (750mg q8h) Placebo/PR48 Mean +/– SE Notes This slide describes the changes in hemoglobin levels observed in patients receiving T12/PR and placebo/PR in clinical trials. Decreases in hemoglobin were observed with placebo/PR as well as T12/PR, although the decreases with telaprevir triple therapy were somewhat more pronounced than with dual therapy. After the telaprevir dosing phase had ended at Week 12, hemoglobin levels improved. By Week 20, levels were similar to those seen with control. Similar findings are not yet available with boceprevir, which was administered in combination with PR for 24 to 44 weeks in Phase III trials. References BL 2 4 6 8 10 12 14 16 20 24 28 36 48 Weeks EPO veel gebruikt in de studies, in België niet terugbetaald Meer marge om ribaverine te reduceren Transfusie ?

15
GENEESMIDDELEN INTERACTIES !!!

16
TAKE HOME protease inhibitoren
Enkel type 1 Complex en veel pillen GENEESMIDDELEN INTERACTIES !!! NIETS ASSOCIËREN ZONDER TE VERIFIËREN anticonceptie GEEN DOSIS REDUCTIES DUUR : tot 50,000 euro per behandeling

17
XYZ van HP

18
HP : indicatie tot therapie
Strict (Maastricht III): Maag en duodenale ulcera. Zowel actieve als doorgemaakte Atrofische gastritis MALT lymfoom van de maag Familiaal maagkanker (eerste graadsverwanten) of volgende op resectie van maagkanker
: Maag en duodenale ulcera. Zowel actieve als doorgemaakte. Atrofische gastritis. MALT lymfoom van de maag. Familiaal maagkanker (eerste graadsverwanten) of volgende op resectie van maagkanker.")
19
Indicatie tot therapie
Andere : Onverklaarde ferriprieve anaemie (dus negatieve colonoscopie) ITP (idiopathische thrombocytopenische purpura) Vóór start (langdurige) NSAID therapie Dyspepsie : beperkt effect (N.N.T. 12 dwz 12 patiënten dienen behandeld te worden om één patient te doen genezen), is wel kosten-baten en effectiever dan langdurig PPI. Preventie maagkanker bij hoog-risico patiënten Bij langdurig PPI gebruik > 1 jaar (preventie atrofische gastritis) Familiaal – persoonlijke voorgeschiedenis Ernstige pan-gastritis, corpus-dominante gastritis, ernstige atrofie Omgevingsfactoren : zwaar nicotine abusus, werkers in stof, kool, kwarts, steengroeves
 ITP (idiopathische thrombocytopenische purpura) Vóór start (langdurige) NSAID therapie. Dyspepsie : beperkt effect (N.N.T. 12 dwz 12 patiënten dienen behandeld te worden om één patient te doen genezen), is wel kosten-baten en effectiever dan langdurig PPI. Preventie maagkanker bij hoog-risico patiënten. Bij langdurig PPI gebruik > 1 jaar (preventie atrofische gastritis) Familiaal – persoonlijke voorgeschiedenis. Ernstige pan-gastritis, corpus-dominante gastritis, ernstige atrofie. Omgevingsfactoren : zwaar nicotine abusus, werkers in stof, kool, kwarts, steengroeves.")
20
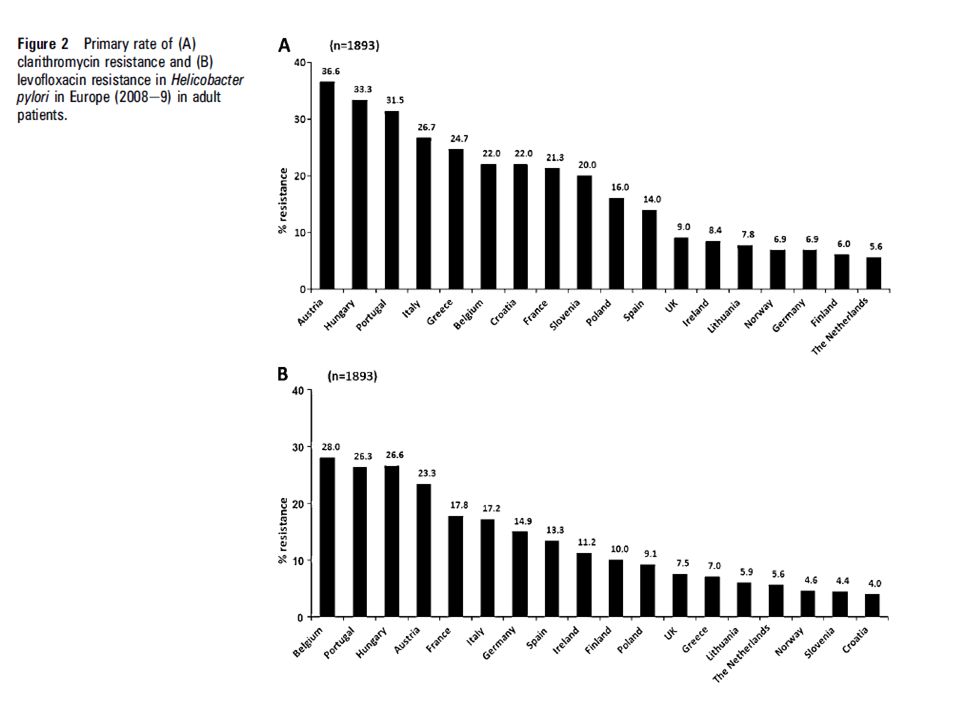
Resistentie probleem Resistentie op claritromycine is problematisch
Klassieke triple therapie : 10 – 30 % succes Amoxycilline resistentie : zeer zeldzaam Metronidazole resistentie in vitro Heeft minder gevolg in vivo Hoger en langer doseren

21
Maastricht IV consensus
Claritromycine-bevattende triple therapie moet verlaten worden in regio’s met hoge resistentie (> 15 à 20 %) zonder voorafgaand gevoeligheidstesten UEGW Stockholm 2011, Gut 2012 ; 61:
 zonder voorafgaand gevoeligheidstesten. UEGW Stockholm 2011, Gut 2012 ; 61:")
23
Maastricht IV – hoge resistentie 1ste lijn
Bismuth-bevattende quadruple therapie Probleem van beschikbaarheid Zo deze niet beschikbaar : sequentiële therapie Succesratio 75% zo claritro-resistentie

24
Voorstel eerste lijn : sequentiële therapie
Dag 1 2 3 4 5 6 7 8 9 10 PPI 2 x 40 mg per dag Amoxicilline 2 x 1 g per dag Claritromycine 2 x 500 mg per dag + Tinidazole/metro 2 x 500 mg per dag

25
Of bismuth bevattend (zo beschikbaar)
Metronidazole 250 mg, 4 x per dag Tetracycline HCL 500 mg, 4 x per dag PPI 40 mg, 2 x per dag 10 à 14 dagen

26
Tweede lijn zo hoge resistentie. Maastricht IV
“levofloxacine containing triple therapy” is recommended “rising rates of levofloxaxine resistance should be taken into account” probleem in België

27
Practisch tweede lijn Bismuth quadruple zo initieel sequentieel (of vice verca Testen gevoeligheid (zeker aan te raden voor derde lijn) Speciale cultuurbodems, best telefonisch af te spreken

28
Alternatieve schema’s
Rifabutine 2 x 150 mg dd PLUS amoxy 2 x 1 g dd PLUS PPI 2 x 40 mg dd (Levofloxacine 1 x 500 mg dd PLUS amoxy 2 x 1 g dd PLUS PPI 2 x 40 mg dd) Alternatieve sequentiële: PPI 2 x 40 mg dd, amoxy 2 x 1 gg (d1-d5) , levofloxacine 2 x 250 à 500 mg (d6-d10) tinidazole/metronidazole 2 x 500 mg (d6-10) striktheid indicatie tot eradicatie ?
 Alternatieve sequentiële: PPI 2 x 40 mg dd, amoxy 2 x 1 gg (d1-d5) , levofloxacine 2 x 250 à 500 mg (d6-d10) tinidazole/metronidazole 2 x 500 mg (d6-10) striktheid indicatie tot eradicatie")
29
Penicilline allergie Bismuth quadruple

30
Controle eradicatie Na twee weken stop PPI (anti-H2 mag verder gegeven worden) 4 weken na eradicatie therapie
 4 weken na eradicatie therapie.")
31
uw welzijn verdient onze beste zorg
Dank uw welzijn verdient onze beste zorg

Verwante presentaties
 SEPSIS>")



![Deltion College Engels C1 Spreken [Edu/003] thema “Oprah at Deltion” can-do : kan duidelijke, gedetailleerde beschrijving geven van complexe onderwerpen,](/8/2033280/big_thumb.jpg "Deltion College Engels C1 Spreken [Edu/003] thema “Oprah at Deltion” can-do : kan duidelijke, gedetailleerde beschrijving geven van complexe onderwerpen,>")


![Deltion College Engels C1 Gesprekken voeren [Edu/002]/ subvaardigheid lezen thema: Order, order…. can-do : kan een bijeenkomst voorzitten © Anne Beeker.](/8/2048322/big_thumb.jpg "Deltion College Engels C1 Gesprekken voeren [Edu/002]/ subvaardigheid lezen thema: Order, order…. can-do : kan een bijeenkomst voorzitten © Anne Beeker.>")









 DIAGNOSTIEK MONITORING ICD’S EN BIVENTRICULAIRE PACING PLOTSE DOOD.>")

