Download de presentatie
De presentatie wordt gedownload. Even geduld aub

1
Aanpak chronische en therapieresistente Depressie (Update multidisciplinaire richtlijn)
Jan Spijker, psychiater Pro Persona/Trimbos-instituut/ Radboud universiteit Apeldoorn 2013

2
belangen Ik, of een familielid in de eerste graad, heb geen significant financieel belang bij of ander belang met een commercieel product /organisatie dat direct of indirect een relatie heeft met het wetenschappelijk programma Ik bespreek geen commerciële producten, of experimenteel gebruik van een product dat niet is goedgekeurd voor dit gebruik gedurende de presentatie tijdens het wetenschappelijke programma. Honoraria als spreker van Wyeth, Eli-Lilly, Astra-Zeneca, GlaxoSmithKline en Servier Trimbos-instituut 2

4
Algoritme ernstig/niet-ernstig:
aantal symptomen (>7 = severe); duur (< of > 3 maanden); beloop; functioneren, suicidaliteit, lijden, comorbiditeit recidief
; duur (< of > 3 maanden); beloop; functioneren, suicidaliteit, lijden, comorbiditeit. recidief.")
5
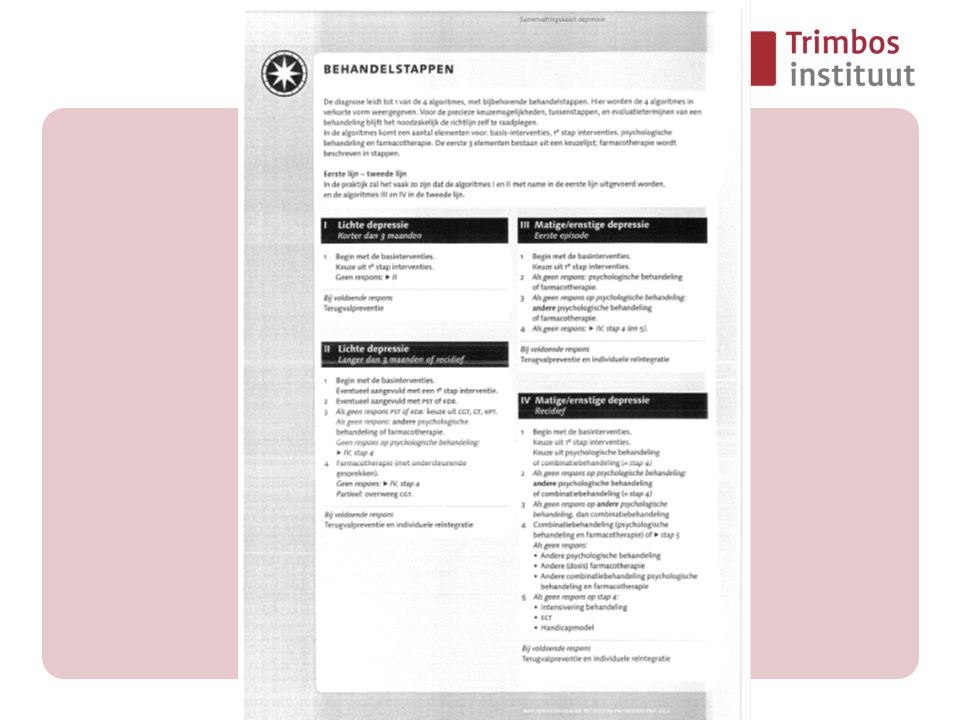
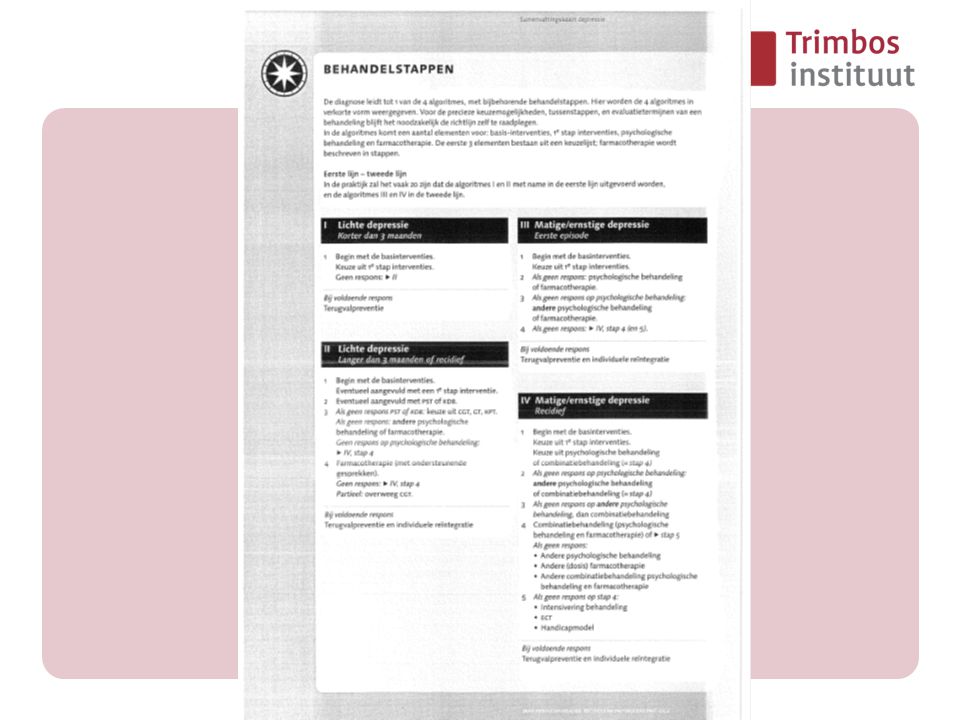
Algoritmes 1e episode- niet-ernstig < 3 mnd
1e episode- niet-ernstig > 3 mnd of recidief 1e episode- ernstig recidief-ernstig

7
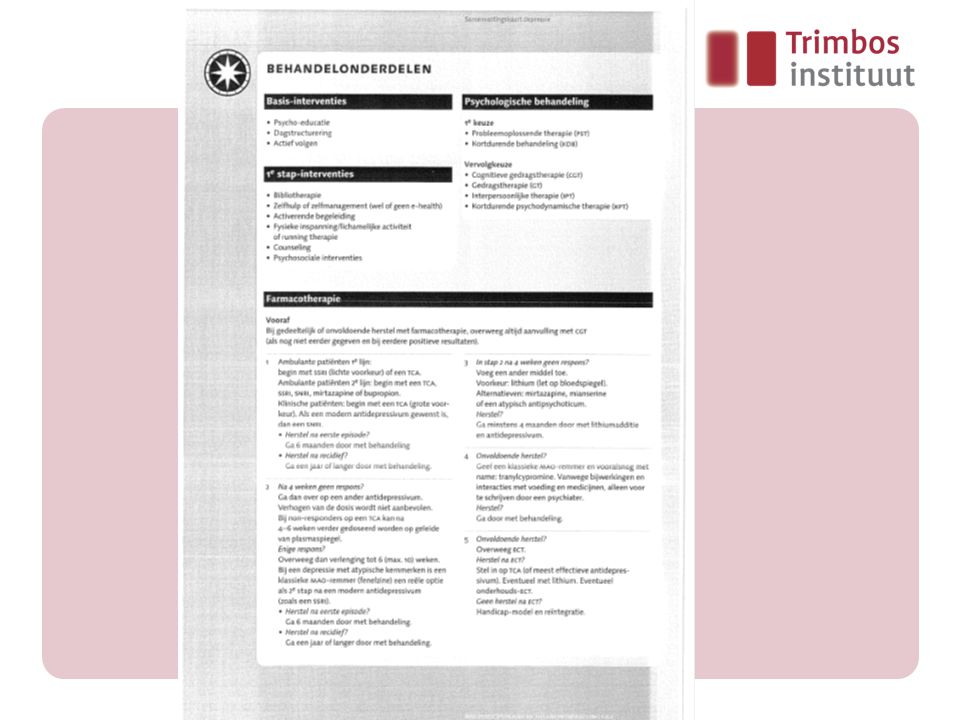
stappenplan Stap 1: ieder AD (SSRI/TCA/SNRI/mirtazapine/bupropion
(opgenomen patienten: TCA/SNRI Stap 2: switch naar andere AD (opgenomen patienten: TCA/SNRI of stap 3) (atypische depressie: MAOI) stap 3: augmenteer met Li, mirtazapine, mianserin, atypische AP stap 4: MAOI stap 5: ECT Alle stappen: ga naar andere stap: 4 wk non-respons, 6 (- to 10) wk partiele respons na herstel: continueer 6 mnd (eerste episode), eenjaar of langer (recidief) combi li + AD: min 4 mnd continueren
 (atypische depressie: MAOI) stap 3: augmenteer met Li, mirtazapine, mianserin, atypische AP. stap 4: MAOI. stap 5: ECT. Alle stappen: ga naar andere stap: 4 wk non-respons, 6 (- to 10) wk partiele respons. na herstel: continueer 6 mnd (eerste episode), eenjaar of langer (recidief) combi li + AD: min 4 mnd continueren.")
8
Literatuur Systematische search van 1 januari 2001 tot begin 2010.
Opbrengst: 918 artikelen Trimbos-instituut 8

9
Niveau van bewijs Studies
A1:Systematische review met minimaal verschillende A2 niveau studies, met consistente resultaten A2:Randomised clinical trial van goede kwaliteit (randomisatie, dubbelblind, gecontroleerd) van voldoende grootte B: Randomised clinical trial van redelijke kwaliteit of onvoldoende grootte of een andere vorm van vergelijkend onderzoek (niet gerandomiseerd, cohortstudie, patient control studie) C: niet vergelijkend onderzoek D: Expert opinie Conclusies 1: 1 A1 studie of in ieder geval 2 onafhankelijke A1 of A2 studies 2: minimaal 2 onafhankelijke niveau B studies 3: 1 niveau A2 of B studie of C studies 4: Expert opinie Trimbos-instituut 9
 van voldoende grootte. B: Randomised clinical trial van redelijke kwaliteit of. onvoldoende grootte of een andere vorm van vergelijkend onderzoek. (niet gerandomiseerd, cohortstudie, patient control studie) C: niet vergelijkend onderzoek. D: Expert opinie. Conclusies. 1: 1 A1 studie of in ieder geval 2 onafhankelijke A1 of A2 studies. 2: minimaal 2 onafhankelijke niveau B studies. 3: 1 niveau A2 of B studie of C studies. 4: Expert opinie. Trimbos-instituut")
10
Chroniciteit > 2 jaar voldoen aan de DSM-criteria
Inclusief: recidiverend met inter-episodisch incompleet herstel Inclusief: dubbele depressie (dysthyme stoornis plus MDE) Niet: dysthyme stoornis Verschil beloopspatronen? 10-20% chronisch beloop; in GGZ 30% chronisch Trimbos-instituut 10
 Niet: dysthyme stoornis. Verschil beloopspatronen 10-20% chronisch beloop; in GGZ 30% chronisch. Trimbos-instituut")
11
Chroniciteit/therapieresistentie
Niet identiek/wel overlap Definitie therapieresistentie: uitgedrukt in aantal niet succesvolle medicatiestappen (voldoende duur, voldoende dosering). Stagering van therapieresistentie Trimbos-instituut 11
. Stagering van therapieresistentie. Trimbos-instituut")
12
Biologische opties Chroniciteit/therapieresistentie
AD zijn waarschijnlijk effectief bij chronische depressie (A2), effectiviteit bij chronische depressie waarschijnlijk minder dan bij niet chronische depressie (A2). AD zijn effectief bij therapieresistente depressie (A1)(zie stappenplan). Het is aannemelijk dat ECT effectief is bij therapieresistente depressie (A2) Er is enig bewijs dat rTMS is op korte termijn effectief bij therapieresistente depressie (A2) Er is geen bewijs dat NVS effectief is bij therapieresistente depressie (A2) DBS niet beoordeeld Trimbos-instituut 12
, effectiviteit bij chronische depressie waarschijnlijk minder dan bij niet chronische depressie (A2). AD zijn effectief bij therapieresistente depressie (A1)(zie stappenplan). Het is aannemelijk dat ECT effectief is bij therapieresistente depressie (A2) Er is enig bewijs dat rTMS is op korte termijn effectief bij therapieresistente depressie (A2) Er is geen bewijs dat NVS effectief is bij therapieresistente depressie (A2) DBS niet beoordeeld. Trimbos-instituut")
13
Biologische opties AD AD zijn effectief bij chronische depressie patienten met chronische depressie of sertraline of imipramine remissie 32% vs 23% (Thase e.a. 2002) AD minder effectief bij chron depressie vs niet chronische depressie remissie 24% vs 30% STAR*D (Gilmer e.a. 2008) Trimbos-instituut 13
 AD minder effectief bij chron depressie vs niet chronische depressie remissie 24% vs 30% STAR*D (Gilmer e.a. 2008) Trimbos-instituut")
14
Biologische opties rTMS
1 review rTMS bij therapieresistentie (1 niet effectieve AD) (Lam e.a, 2008) 24 studies met 1092 pat Significant effect (SMD = 0.48 ), respons van 25% tov 9% in de controle conditie Duur behandeling 1-4wk. Trimbos-instituut 14
 (Lam e.a, 2008) 24 studies met 1092 pat. Significant effect (SMD = 0.48 ), respons van 25% tov 9% in de controle conditie. Duur behandeling 1-4wk. Trimbos-instituut")
15
Biologische opties NVS
1 RCT (Rush e.a., 2005) 235 patienten. Geen significant verschil in effect na 10 wk (15.2% vs 10%) Echter in open follow-up bij 205 patienten nam de respons verder toe (27.2%) Trimbos-instituut 15
 235 patienten. Geen significant verschil in effect na 10 wk (15.2% vs 10%) Echter in open follow-up bij 205 patienten nam de respons verder toe (27.2%) Trimbos-instituut")
16
Aanbevelingen: biologische opties Chroniciteit/therapieresistentie
Bij chroniciteit: AD waarschijnlijk effectief Voorkeur voor AD Overweeg altijd ECT rTMS, NVS??? Trimbos-instituut 16

17
Psychologische opties Chroniciteit/therapieresistentie
Review met 16 studies, 7 met chron. depressie. effect size PT = 0.23 (Cuijpers e.a. 2010) Conclusies: PT is effectief bij chron. depressie maar mogelijk minder effectief dan bij niet-chronische depressie. (B) Aanbeveling: Geen Trimbos-instituut 17
 Conclusies: PT is effectief bij chron. depressie maar mogelijk minder effectief dan bij niet-chronische depressie. (B) Aanbeveling: Geen. Trimbos-instituut")
18
Combinatie behandeling Chroniciteit/therapieresistentie
Conclusies: Combinatie is effectiever dan mono bij chronische depressie (A1). Conclusies: effectiviteit CBASP + AD: tegenstrijdig (A1) Aanbeveling: combinatie verdient voorkeur bij chronische depressie. Nog niet duidelijk of dat met CBASP moet zijn. Trimbos-instituut 18
. Conclusies: effectiviteit CBASP + AD: tegenstrijdig (A1) Aanbeveling: combinatie verdient voorkeur bij chronische depressie. Nog niet duidelijk of dat met CBASP moet zijn. Trimbos-instituut")
19
Combinatie behandeling CBASP
CBASP vs AD vs combi (Keller e.a, 2000) 681 patienten met chronisch depressie Combi 48% remissie vs CBASP 33% vs AD 29% AD+CBASP vs AD vs AD + KPP (Koscis e.a. 2009) Geen verschillen Trimbos-instituut 19
 681 patienten met chronisch depressie. Combi 48% remissie vs CBASP 33% vs AD 29% AD+CBASP vs AD vs AD + KPP (Koscis e.a. 2009) Geen verschillen. Trimbos-instituut")
20
Rehabilitatie Niet specifiek voor de doelgroep chronische en therapieresistente depressie Aanbeveling: wel van belang (maatschappelijk) functioneren, reintegratie, herstel) Trimbos-instituut 20
 functioneren, reintegratie, herstel) Trimbos-instituut")
21
Gecombineerde zorg Model met coordinatie vd zorg, veelal vanuit de 1e lijn;consultatie; stepped care, richtlijn. Diseasemanagement/collaborative care effectief tav afname van depressiesymptomen (A1) Niet specifiek voor de doelgroep chronische en therapieresistente depressie Aanbeveling: gecombineerde zorg is veelbelovend Trimbos-instituut 21
 Niet specifiek voor de doelgroep chronische en therapieresistente depressie. Aanbeveling: gecombineerde zorg is veelbelovend. Trimbos-instituut")
22
Aanbeveling chroniciteit therapieresistentie
1. chronische depressie en geen behandeling 2. chronische depressie en inadequate behandeling 3. chronische en therapieresistente behandeling Voorstel voor therapieresistentie: tenminste twee adequaat uitgevoerde AD stappen en een PT stap. Trimbos-instituut 22

23
Aanbeveling chroniciteit therapieresistentie
Groep 1: algoritme (matig) ernstig (eenmalig/recidief) Groep 2: evalueer de behandeling en begin bij die stap die niet adequaat is uitgevoerd. Groep 3: stap in bij combinatiebehandeling. Biologische stappenplan vervolgen. Intensivering behandeling. Second opinion. Rehabilitatie afhankelijk van context, klinische oordeel, voorkeur patient. Indien rehabilitatie dan in een gecombineerd zorgmodel Trimbos-instituut 23
 ernstig (eenmalig/recidief) Groep 2: evalueer de behandeling en begin bij die stap die niet adequaat is uitgevoerd. Groep 3: stap in bij combinatiebehandeling. Biologische stappenplan vervolgen. Intensivering behandeling. Second opinion. Rehabilitatie afhankelijk van context, klinische oordeel, voorkeur patient. Indien rehabilitatie dan in een gecombineerd zorgmodel. Trimbos-instituut")
25
Algoritme III 1e episode- ernstig
Begin met de basinterventies: Keuze uit 1e stap interventies Als geen respons: psychotherapie of farmacotherapie. Als geen respons op psychotherapie: andere psychotherapie of farmacotherapie. Als geen respons, ga dan naar IV, stap 4 (en 5). Trimbos-instituut 25
. Trimbos-instituut")
26
Algoritme IV recidief-ernstig
Begin met de basinterventies: Keuze uit 1e stap interventies.Keuze uit psychotherapie of combinatiebehandeling (= stap 4) Als geen respons op psychotherapie: andere psychotherapie of combinatiebehandeling (= stap 4) Als geen respons op andere psychotherapie, dan combinatiebehandeling (= stap 4) Combinatiebehandeling (psychotherapie en farmacotherapie). Of naar stap 5. Als geen respons: Andere psychotherapie Andere (dosis) farmacotherapie Andere combinatiebehandeling psychotherapie en farmacotherapie Als geen respons stap 4:Intensivering behandeling stap 4 ECT, Handicapmodel Trimbos-instituut 26
 Als geen respons op psychotherapie: andere psychotherapie of combinatiebehandeling (= stap 4) Als geen respons op andere psychotherapie, dan combinatiebehandeling (= stap 4) Combinatiebehandeling (psychotherapie en farmacotherapie). Of naar stap 5. Als geen respons: Andere psychotherapie Andere (dosis) farmacotherapie Andere combinatiebehandeling psychotherapie en farmacotherapie. Als geen respons stap 4:Intensivering behandeling stap 4 ECT, Handicapmodel. Trimbos-instituut")
27
Vragen ? Voor meer informatie over het Update-project:
Jolanda Meeuwissen (projectleider),
,")
Verwante presentaties










 Quiz Night !>")








