Download de presentatie
De presentatie wordt gedownload. Even geduld aub

1
Passend gebruik van ICD’s implanteren we teveel? AMC Hartcentrum symposium a la carte 5 december 2014

2
Met een ICD Voorkomen plotselinge dood

3
Met een ICD iemand die gereanimeerd is iemand die gereanimeerd is iemand met een ernstige ritmestr. iemand met een ernstige ritmestr. of het sterke vermoeden daarop of het sterke vermoeden daarop Voorkomen plotselinge dood Secundaire preventie

4
Als het risico erop sterk verhoogd is na een hartinfarct én na een hartinfarct én een verminderde hartfunctie én een verminderde hartfunctie én korte ritmestoornissen korte ritmestoornissen Voorkomen plotselinge dood Primaire preventie

5
Als het risico erop sterk verhoogd is na een hartinfarct én na een hartinfarct én een verminderde hartfunctie een verminderde hartfunctie Voorkomen plotselinge dood Primaire preventie ‘MADIT-II profiel’

6
Als het risico erop sterk verhoogd is na een hartinfarct én na een hartinfarct én een verminderde hartfunctie een verminderde hartfunctie bij een anderszins verminderde HF bij een anderszins verminderde HF sommige erfelijke hartritmestr. sommige erfelijke hartritmestr. Voorkomen plotselinge dood Primaire preventie ‘SCDHeFT profiel’

7
12 months16 months41.4 months27 months 13 months45 months6 months Sudden Cardiac Death in CHF Patients with low LVEF SCD accounts for ~50% of all deaths.

8
MADIT-I/MADIT-II/SCDHeFT Inclusion CriteriaMADIT 1 (196 patients) MADIT-II 2 (704 patients) SCHDHeFT 3 (2521 patients) CAD/Post-MI LV Dysfunction (<35%) (<40%) (<35%) NSVT Inducible VT on EPS Inducible, non- suppressible VT on EPS 1 Moss AJ. N Engl J Med. 1996;335:1933-40. 2 Moss AJ. N Engl J Med. 2002; 346:877-83. 3 Bardy GH. N Engl J Med. 2005; 352:225-37.

9
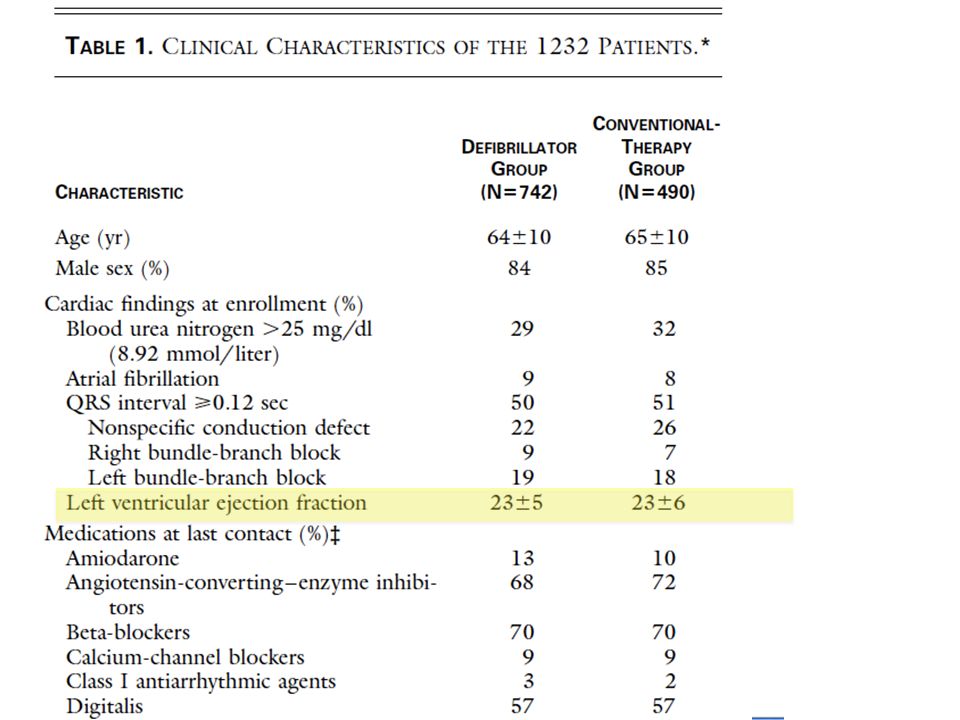
MADIT II MADIT II At least 1 month following MI At least 1 month following MI LVEF < 30% LVEF < 30% N=1232, 3:2 randomization ICD vs. “conventional” N=1232, 3:2 randomization ICD vs. “conventional” Relative risk 0.69 / 20 month survival 86% vs. 80% Relative risk 0.69 / 20 month survival 86% vs. 80% MADIT-II Survival Results

10
Moss AJ. N Engl J Med. 2002;346:877-83. Defibrillator Conventional P = 0.007 1.0 0.9 0.8 0.7 0.6 0.0 Probability of Survival 01234 Year No. At Risk Defibrillator742502 (0.91)274 (0.94)110 (0.78)9 Conventional490329 (0.90)170 (0.78) 65 (0.69)3
274 (0.94)110 (0.78)9 Conventional (0.90)170 (0.78) 65 (0.69)3.")
11
MADIT II: 8 years of follow-up

12
31% reduced total mortality (19.8% vs. 14.2%) ≥ 5 years post MI Majority of patients had no intervention More HF submissions in ICD group Why is the effect only after 9 months? The MADIT-II trial LVEF 1 mth post-MI & 3 mths Revasc.
 ≥ 5 years post MI Majority of patients had no intervention More HF submissions in ICD group Why is the effect only after 9 months. The MADIT-II trial LVEF 1 mth post-MI & 3 mths Revasc..")
13
MADIT II, tijd vs effect ICD Circulation 2004;109:1082-84 Conclusie: Aritmogeen substraat heeft tijd nodig om zich te ontwikkelen. ICD implantatie niet te vroeg post infarct.

15
Sudden death or CA & resuscitation (%) in Valiant; 2005 LVEF < 40% or CHF
 in Valiant; 2005 LVEF < 40% or CHF")
16
SCD-Heft SCD-Heft NYHA II or III, LVEF < 35 % NYHA II or III, LVEF < 35 % Conventional vs. Amiodarone vs. ICD (single lead, VVI 34 min -1 Conventional vs. Amiodarone vs. ICD (single lead, VVI 34 min -1 N=2521 N=2521 Ischemic vs. non-ischemic 52/48 Ischemic vs. non-ischemic 52/48 Median follow-up 46 months Median follow-up 46 months Relative risk C vs. A ns; ICD vs A/C 0.77 Relative risk C vs. A ns; ICD vs A/C 0.77 No difference DCM vs. IHD No difference DCM vs. IHD DCM – Primary prevention

17
SCD-HeFT, resultaten

18
MADIT-II, SCDHeFT profile still going strong in 2014?

19
Dalal D, Arking D, Cheng A, Akar FG, Post W, Kao L, et al. Circulation 2006;114: suppl:558-9. SCDHeFT Profile SCDHeFT Profile 465 patients 465 patients annual shock rate 4.5% (incl VT) annual shock rate 4.5% (incl VT) Baltimore data (PROSE_ICD)
 annual shock rate 4.5% (incl VT) Baltimore data (PROSE_ICD).")
20
Sudden death or CA & resuscitation (%) in Valiant; 2005 LVEF < 40% or CHF Max 4%/y
 in Valiant; 2005 LVEF < 40% or CHF Max 4%/y")
21
Sudden death or CA & resuscitation (%) in Valiant; 2005 LVEF < 40% or CHF Max 2%/y
 in Valiant; 2005 LVEF < 40% or CHF Max 2%/y")
22
LUMC data 2054 ICD implanted patients 2054 ICD implanted patients Primary: 1110 (54%) Primary: 1110 (54%) 211 (19%) app ther 211 (19%) app ther 105 (9%) app shock 105 (9%) app shock Secondary: 944 (46%) Secondary: 944 (46%) 416 (44%) app ther 416 (44%) app ther 300 (32%) app shock 300 (32%) app shock Appropriate ICD therapy was observed in 169 MADIT II ICD patients (24%). Courtesy Martin Schalij 2010

24
Primary prevention JW Borleffs, LUMC Primary Prevention: Patient survival Courtesy Martin Schalij 2010 LUMC data MADIT II 3y mortality ICD group >20% SCDHeFT 5y mortality ICD group 29%

25
First and Second app shock Courtesy Martin Schalij 2010

26
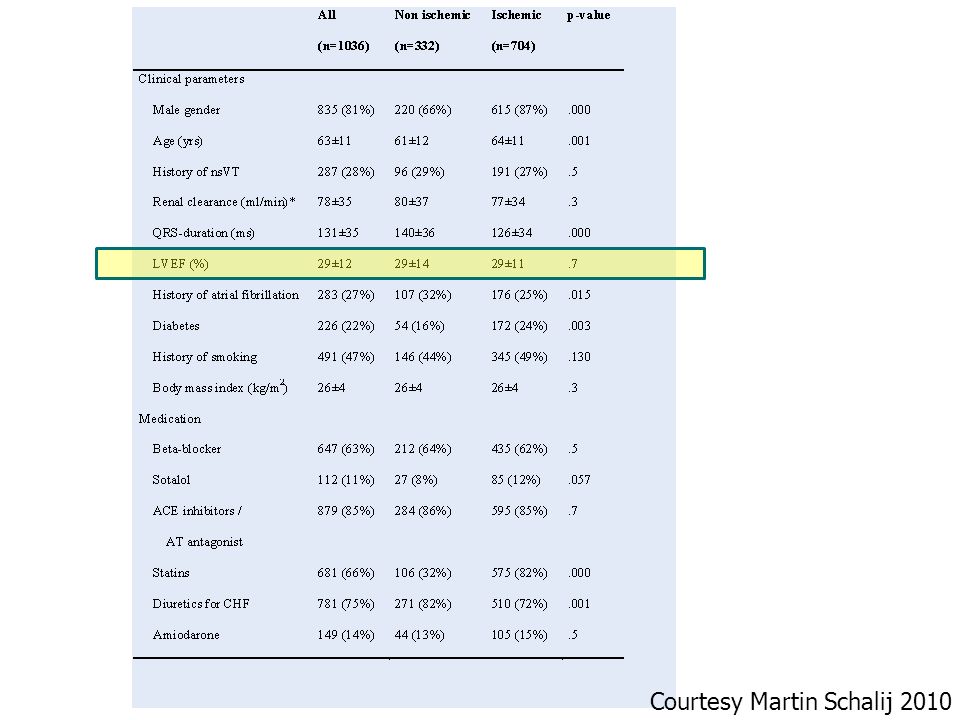
Analysis of Erasmus MC database for CAD and DCM (January 2004 - June 2009) Prospective cohort study of 684 consecutive primary prevention ICD patients with CAD or DCM. CAD in 420 (61%) Prospective cohort study of 684 consecutive primary prevention ICD patients with CAD or DCM. CAD in 420 (61%) DCM in 264 (39%) DCM in 264 (39%) mean LVEF 26 ± 8% Mortality, appropriate and inappropriate shocks Mortality, appropriate and inappropriate shocks Courtesy Luc Jordaens 2010
 Prospective cohort study of 684 consecutive primary prevention ICD patients with CAD or DCM. CAD in 420 (61%) DCM in 264 (39%) DCM in 264 (39%) mean LVEF 26 ± 8% Mortality, appropriate and inappropriate shocks Mortality, appropriate and inappropriate shocks Courtesy Luc Jordaens")
27
65 (10%) over a mean of 27,6 months, MADIT II 3y mortality ICD group >20% SCDHeFT 5y mortality ICD group 29% 65 (10%) over a mean of 27,6 months,
 over a mean of 27,6 months, MADIT II 3y mortality ICD group >20% SCDHeFT 5y mortality ICD group 29% 65 (10%) over a mean of 27,6 months,")
28
Appropriate shocks / ATP 150 (22%) at a median of 20 months Courtesy Luc Jordaens 2010
 at a median of 20 months Courtesy Luc Jordaens 2010")
29
All cause mortality versus LVEF and shocks / ATP Courtesy Luc Jordaens 2010

30
Comparison with the Amsterdam AMC and the Erasmus MC N = 587 patients Courtesy Luc Jordaens 2010 AMC 2006 pts

31
Comparison with the Amsterdam AMC and the Erasmus MC N = 587 patients Courtesy Luc Jordaens 2010

32
32

33
33 ICD use in primary prevention 2006

34
34 ICD use in primary prevention 2008

35
Neth Heart Journal 2009

36
36

37
37 Benefit overestimated Benefit overestimated Adverse effects underestimated Adverse effects underestimated Morbidity Morbidity Quality of life Quality of life Proarrhythmia Proarrhythmia Unfavorable cost-effectiveness Unfavorable cost-effectiveness More specific riskstratification (risk scores) More specific riskstratification (risk scores) Should be reconsidered!! Should be reconsidered!! ICD use in primary prevention

38
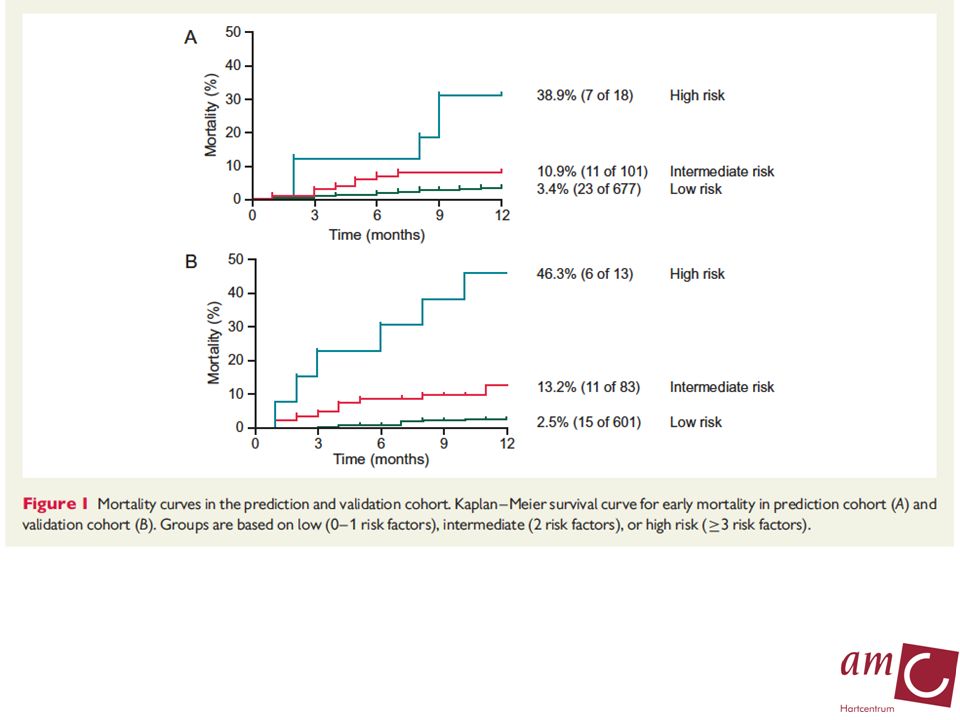
38 Riskfactors Riskfactors - NYHA > class II - age > 70y - Ureum > 9.3 mmol/l - QRS > 0.12 s - AFib No benefit ICD in pts with 0 or ≥ 3 riskfactors Goldenberg I et al., JACC 2008;51:288-296 ICD use in primary prevention

39
N=577 iCMP (AMC, MST) Goldenberg score
 Goldenberg score")
40
N=577 iCMP (AMC, MST) Goldenberg score
 Goldenberg score")
41
Prediction cohort (AMC, MST): 861pts “SCDHeFT profile” Validation cohort (EMC): 706
: 861pts SCDHeFT profile Validation cohort (EMC): 706")
43
Waarom zo anders? MADIT infarcten vs 2014 infarcten MADIT infarcten vs 2014 infarcten PCI treated PCI treated Optimal drug therapy? Optimal drug therapy? Mean LVEF in MADIT ±23% Mean LVEF in MADIT ±23% Mean LVEF in 2010 close to 30% Mean LVEF in 2010 close to 30% Risk stratification is not optimal! Risk stratification is not optimal!

44
Nieuw onderzoek dus nodig Primaire preventie patienten Primaire preventie patienten PCI treated PCI treated Optimal drug therapy Optimal drug therapy Risico factors post-hoc MADIT-II analyses Risico factors post-hoc MADIT-II analyses + anderen (LUMC, AMC, MST ervaring) + anderen (LUMC, AMC, MST ervaring) Prospectieve registry Prospectieve registry
 + anderen (LUMC, AMC, MST ervaring) Prospectieve registry Prospectieve registry")
45
Nieuw onderzoek dus nodig 1500 patienten (LVEF <35%) 1500 patienten (LVEF <35%) 1.5 jaar enrollment 1.5 jaar enrollment 2 jaar follow-up gemiddeld, minimaal 18mnd 2 jaar follow-up gemiddeld, minimaal 18mnd Risico factors post-hoc MADIT-II analyses Risico factors post-hoc MADIT-II analyses + anderen (LUMC ervaring) + anderen (LUMC ervaring) Uitgebreide documentatie alle relevante events Uitgebreide documentatie alle relevante events
 1500 patienten (LVEF <35%) 1.5 jaar enrollment 1.5 jaar enrollment 2 jaar follow-up gemiddeld, minimaal 18mnd 2 jaar follow-up gemiddeld, minimaal 18mnd Risico factors post-hoc MADIT-II analyses Risico factors post-hoc MADIT-II analyses + anderen (LUMC ervaring) + anderen (LUMC ervaring) Uitgebreide documentatie alle relevante events Uitgebreide documentatie alle relevante events")
46
Do-IT Prospective registry Prospective registry Mortality Mortality Appropriate ICD shocks Appropriate ICD shocks Inappropriate ICD shocks Inappropriate ICD shocks Cost effective analysis (Dijkgraaf, AMC) Cost effective analysis (Dijkgraaf, AMC) To assess the cost minimization and budget impact of targeted supply of ICD implantation To assess the cost minimization and budget impact of targeted supply of ICD implantation
 Cost effective analysis (Dijkgraaf, AMC) To assess the cost minimization and budget impact of targeted supply of ICD implantation To assess the cost minimization and budget impact of targeted supply of ICD implantation")
47
Conclusies De Huidige ICD populatie is een andere dan die uit ‘de trials’ De Huidige ICD populatie is een andere dan die uit ‘de trials’ Infarcten anders behandeld Infarcten anders behandeld Betere ondersteunende therapie Betere ondersteunende therapie Betere risico inschatting nodig Betere risico inschatting nodig Gaat mogelijk komen (Do-It) Gaat mogelijk komen (Do-It)
 Gaat mogelijk komen (Do-It)")
48
Thank you

49
nogmaals dank aan Lieve Peeters, Pauline Ebbinkhuijsen Lieve Peeters, Pauline Ebbinkhuijsen Onze sponsors van vandaag Onze sponsors van vandaag Uw allen voor uw aanwezigheid Uw allen voor uw aanwezigheid

Verwante presentaties













 in patients presenting without persistent ST-segment elevation 20-4-20151Eduard van den.>")
![Deltion College Engels B2 (telefoon)gesprekken voeren[Edu/002] /subvaardigheid lezen/schrijven thema: I am so sorry for you… can-do : kan medeleven betuigen.](/6/5659076/big_thumb.jpg "Deltion College Engels B2 (telefoon)gesprekken voeren[Edu/002] /subvaardigheid lezen/schrijven thema: I am so sorry for you… can-do : kan medeleven betuigen.>")





 een consumptie van 10 gram zout per dag is goed. De gemiddelde zoutinname per persoon, die we vandaag de dag.>")