Download de presentatie
De presentatie wordt gedownload. Even geduld aub

1
Behandeling van hyperlipidemie in ‘Chronic Kidney Disease’ (CKD) M. Couttenye Kidney Disease: Improving Global Outcomes (KDIGO) Lipid Work Group. KDIGO Clinical Practice Guideline for Lipid Management in Chronic Kidney Disease. Kidney inter., Suppl. 2013; 3: 259–305
 Lipid Work Group. KDIGO Clinical Practice Guideline for Lipid Management in Chronic Kidney Disease. Kidney inter., Suppl. 2013; 3: 259–305.")
2
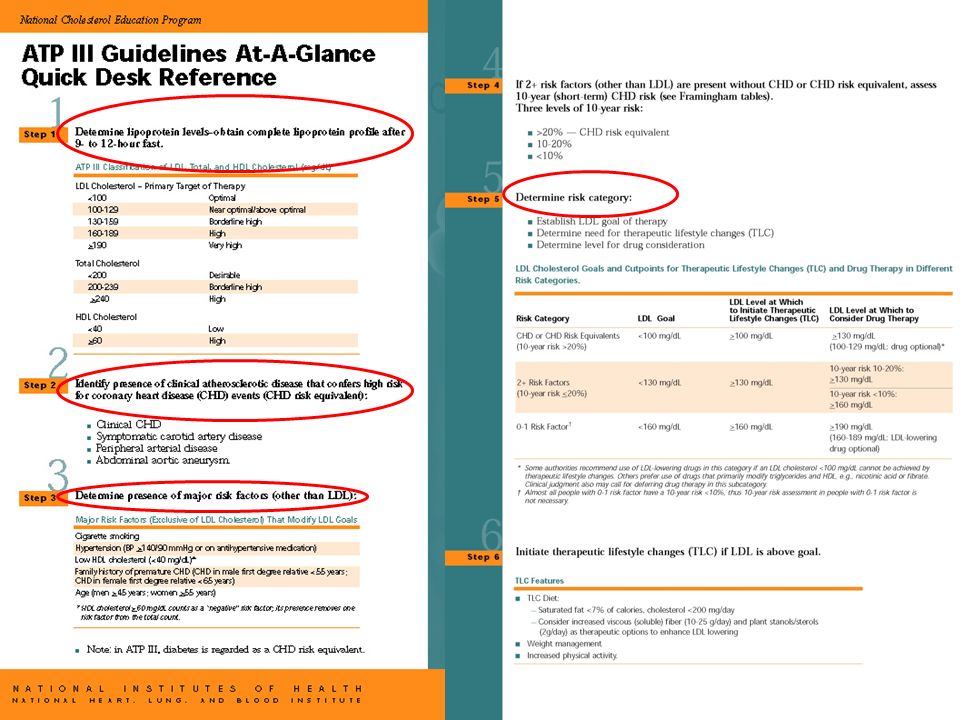
Waarom nieuwe guidelines? Vorige dateren van 2003 Waren gebaseerd op ATP III guidelines (2002):
:")
4
Waarom nieuwe guidelines? Vorige dateren van 2003 Waren gebaseerd op ATP III guidelines (2002): doch - enkel voor e-GFR > 15 ml/min - CKD = CHD risk equivalent - Cave : meer nevenwerkingen
: doch - enkel voor e-GFR > 15 ml/min - CKD = CHD risk equivalent - Cave : meer nevenwerkingen.")
5
What’s new since 2003 ? Massa trials in non-CKD patiënten Uiteindelijk toch ook in CKD - ALERT (transplantation) - 4D (diabetes) - PREVEND IT (preventie ESRD) - AURORA (rosuva in HD: mortality and CV events) - MAAR… NEGATIEF
 - 4D (diabetes) - PREVEND IT (preventie ESRD) - AURORA (rosuva in HD: mortality and CV events) - MAAR… NEGATIEF.")
6
Mogelijke verklaringen? Opzet van de studies? Niches? Vasculaire stijfheid ? Vasculaire calcificaties? Structurele hartafwijkingen? Sympathische overactiveit? Toegenomen risico op ritmestoornissen en hartfalen?

7
Tot 2011 … “PIVOTAL “ STUDY: SHARP (heart and renal protection in CKD (non-dialysis and dialysis) patients basis voor nieuwe guidelines
 patients basis voor nieuwe guidelines")
8
KDIGO 2013 1. Assess lipid status: when and how 2. Prescribe lipid-lowering treatment: when and how PS: inmiddels ook nieuwe guidelines voor non-CKD: ACC-AHA 2013

9
Chapter 2: Pharmacological cholesterol-lowering treatment in adults INLEIDING Doel van behandeling = reductie artheriosclerotische morbiditeit/mortaliteit Life style maatregelen ? - Beperkt effect op cholesterol - Geen bewezen effect op “harde” eindpunten Enkel bewijs voor effect van statines (± ezitimibe) op “major atherosclerotic events” (MACE’s) bij patiënten met CKD DUS: Statines: Voor wie? Aan welke dosis?
 op major atherosclerotic events (MACE’s) bij patiënten met CKD DUS: Statines: Voor wie. Aan welke dosis .")
10
Chapter 2: Pharmacological cholesterol-lowering treatment in adults ACHTERGROND : voor wie? LDL-C is onafhankelijke risicofactor voor MACE’s in de algemene populatie maar niet in CKD patienten In dialyse patiënten: paradoxale associatie LDL-C/ CHD o.a. door factor ondervoeding In non-dialyse CKD patiënten:hoe lager de e-GFR, hoe lager de predictieve waarde van LDL-C voor CHD In de algemene populatie is de absolute verbetering van het coronair risico d.m.v. statines proportioneel met het base- line coronair risico Vandaar:

11
Chapter 2: Pharmacological cholesterol-lowering treatment in adults 3 determinanten om te beslissen tot voorschrijven van lipiden verlagende therapie: 1. Baseline coronair risico (coronary death or non-fatal MI): >10/ 1000 patiënt-jaren 2. Case–fatality rate na MI: steeds hoger in CKD 3. Bewijs dat de medicatie werkt ! BESLUIT: in CKD voorschrijven op basis van 1. coronair risico en 3.klinische studies met harde eindpunten
: >10/ 1000 patiënt-jaren 2. Case–fatality rate na MI: steeds hoger in CKD 3. Bewijs dat de medicatie werkt . BESLUIT: in CKD voorschrijven op basis van 1. coronair risico en 3.klinische studies met harde eindpunten.")
12
Chapter 2: Pharmacological cholesterol-lowering treatment in adults ACHTERGROND : voor wie ? Coronair risico?

14
Chapter 2: Pharmacological cholesterol-lowering treatment in adults GUIDELINES GuidelineAgeeGFRCompoundGrade of evidence 2.1.1 ≥ 50 < 60 (G3-G5) (no RRT) Statin (± ezetimibe)1A 2.1.2 ≥ 50≥ 60 (G1-G2) (no RRT) Statin1B 2.218-49G1-G5 (no RRT) Statin IF*2A 2.3 ≥ 18 DialysisStart ? Not routinely Continue ? Yes 2A 2C 2.4 ≥ 18 TransplantationStatin2B *one or more of these criteria: Known coronary disease Diabetes mellitus Prior ischemic stroke Estimated 10 y incidence of coronary death or non fatal MI > 10% (calculator)
.")
15
Chapter 2: Pharmacological cholesterol-lowering treatment in adults ACHTERGROND: hoeveel ? Er is geen evidentie (ook niet in algemene populatie!) dat dosis moet aangepast worden aan een “streef-LDL-C” Neveneffecten zijn dosisafhankelijk, in de algemene populatie maar a fortiriori in CKD patiënten: - Gewijzigde farmacokinetiek - Geneesmiddeleninteracties (polyfarmacie!) - Co-morbiditeiten PRAGMATISCHE OPLOSSING: veilige dosissen in RCT’s in CKD patiënten - geen voorkeur voor type statine
 dat dosis moet aangepast worden aan een streef-LDL-C Neveneffecten zijn dosisafhankelijk, in de algemene populatie maar a fortiriori in CKD patiënten: - Gewijzigde farmacokinetiek - Geneesmiddeleninteracties (polyfarmacie!) - Co-morbiditeiten PRAGMATISCHE OPLOSSING: veilige dosissen in RCT’s in CKD patiënten - geen voorkeur voor type statine.")
16
Chapter 2: Pharmacological cholesterol-lowering treatment in adults hoeveel ?

17
Chapter 2: Pharmacological cholesterol-lowering treatment in adults Monitoring? Quid CK, levertesten ? - Geen monitoring in a-symptomatische patiënten! - Levertesten enkel baseline bepalen

18
Chapter 1 : Assessment of lipidstatus in adults with CKD KDIGO 1.1: In adults with newly identified CKD (including those treated with chronic dialysis or kidney transplantation), we recommend evaluation with a lipid profile (total cholesterol, LDL cholesterol, HDL cholesterol, triglycerides).(1C) Rationale ? - Om potentieel remedieerbare (secundaire) oorzaken uit te sluiten - Om ernstige dyslipidemieën te detecteren : Alarm-levels voor verder onderzoek (LDL > 190 mg/dl- TG > 1000 mg/dl) 1C ? Geen direct bewijs van klinisch voordeel van de meting … maar geen nadelen. PS: geen Lp(a) nodig !
 oorzaken uit te sluiten - Om ernstige dyslipidemieën te detecteren : Alarm-levels voor verder onderzoek (LDL > 190 mg/dl- TG > 1000 mg/dl) 1C . Geen direct bewijs van klinisch voordeel van de meting … maar geen nadelen. PS: geen Lp(a) nodig !.")
19
KDIGO 1.1: In adults with newly identified CKD (including those treated with chronic dialysis or kidney transplantation), we recommend evaluation with a lipid profile (total cholesterol, LDL cholesterol, HDL cholesterol, triglycerides).(1C)
, we recommend evaluation with a lipid profile (total cholesterol, LDL cholesterol, HDL cholesterol, triglycerides).(1C)")
20
Chapter 1 : Assessment of lipidstatus in adults with CKD KDIGO1.2: In adults with CKD (including those treated with chronic dialysis or kidney transplantation), follow-up measurement of lipid levels is not required for the majority of patients. (Not Graded) Dosis statine NIET meer optitreren: er is geen evidentie die deze strategie onderbouwt (in CKD en non-CKD!) Belangrijke within- subject variabiliteit van de meting Verband LDL- adverse clinical outcome is zwak in CKD Risico op neveneffecten van de medicatie in CKD Potentiele indicaties voor LDL monitoring ? - Compliance - Veranderen van RRT modaliteit - Nieuwe remedieerbare oorzaak? - CKD patients <50 y (cfr 2.2)
 Dosis statine NIET meer optitreren: er is geen evidentie die deze strategie onderbouwt (in CKD en non-CKD!) Belangrijke within- subject variabiliteit van de meting Verband LDL- adverse clinical outcome is zwak in CKD Risico op neveneffecten van de medicatie in CKD Potentiele indicaties voor LDL monitoring . - Compliance - Veranderen van RRT modaliteit - Nieuwe remedieerbare oorzaak. - CKD patients <50 y (cfr 2.2).")
21
Summary (a) Rule out remediable causes of secondary dyslipidemia. (b) Establish the indication of treatment (YES or NO) and select agent and dose. (c) Treat according to a ‘‘fire-and-forget’’ strategy: do not measure LDL-C unless the results would alter management.
 Establish the indication of treatment (YES or NO) and select agent and dose. (c) Treat according to a ‘‘fire-and-forget’’ strategy: do not measure LDL-C unless the results would alter management..")
22
Summary Upon first presentation to establish the diagnosis of CKD, the nephrologist will obtain a full lipid profile as part of routine care. In case of referral and to confirm the CKD diagnosis, a full lipid profile may already be available. Results of the lipid profile should be used together with other clinical data to rule out remediable causes of secondary dyslipidemia. If excluded, the nephrologist will establish whether statin treatment is indicated (YES or NO) based on underlying cardiovascular risk. If the level of risk suggests that statin treatment is indicated, she/he will select a dose of a statin (Table 4) that is available in her/his country and has been tested for safety in people with CKD. Contemporary practice and other clinical practice guidelines emphasize the use of targets for LDL-C (e.g., 1.8 or 2.6 mmol/l [70 or 100mg/dl]),which require repeated measurements of LDL-C and treatment escalation with higher doses of statin or initiation of combination lipid-lowering therapy (‘‘treat-to-target’’ strategy) when the LDL-C target is not met.The KDIGO Work Group does not recommend the treat- to-target strategy because it has never been proven beneficial in any clinical trial. Inaddition, higher doses of statins have not been proven to be safe in the setting of CKD. Therefore, the Work Group recommends a ‘‘fire-and-forget’’ strategy for patients with CKD (see Rationale for Recommendation 1.2). Physicians may choose to perform follow-up measurement of lipid levels in patients for whom these measurements are judged to favorably influence adherence to treatment or other processes of care.
 based on underlying cardiovascular risk. If the level of risk suggests that statin treatment is indicated, she/he will select a dose of a statin (Table 4) that is available in her/his country and has been tested for safety in people with CKD. Contemporary practice and other clinical practice guidelines emphasize the use of targets for LDL-C (e.g., 1.8 or 2.6 mmol/l [70 or 100mg/dl]),which require repeated measurements of LDL-C and treatment escalation with higher doses of statin or initiation of combination lipid-lowering therapy (‘‘treat-to-target’’ strategy) when the LDL-C target is not met.The KDIGO Work Group does not recommend the treat- to-target strategy because it has never been proven beneficial in any clinical trial. Inaddition, higher doses of statins have not been proven to be safe in the setting of CKD. Therefore, the Work Group recommends a ‘‘fire-and-forget’’ strategy for patients with CKD (see Rationale for Recommendation 1.2). Physicians may choose to perform follow-up measurement of lipid levels in patients for whom these measurements are judged to favorably influence adherence to treatment or other processes of care..")
23
KDIGO research recommendations SHARP: follow up beyond 5 y ? Effect on renal progression ? Majority of CKD is managed in primary care : audits in this setting ? Pooling of 4D, AURORA & SHARP : better assessment of benefit/risk in dialysis patients

24
Enkele oefeningen ?

25
!Ook nieuwe guidelines voor algemene(non- CKD)populatie: ACC-AHA guidelines for use of statins in patients at increased CV risk Keaney JF Jr et al. N Engl J Med 2014;370:275-278. Figure 1. 2013 American College of Cardiology–American Heart Association Guidelines for Use of Statin Therapy in Patients at Increased Cardiovascular Risk. Persons with clinical atherosclerotic cardiovascular disease (CVD) include those with an acute coronary syndrome and those with a history of myocardial infarction, stable or unstable angina, coronary or other arterial revascularization, or stroke, transient ischemic attack, or peripheral arterial disease that is presumed to be of atherosclerotic origin. High-intensity statin therapy is recommended for most patients meeting these criteria. Patients predisposed to adverse statin effects (including those with impaired renal or hepatic function, other serious coexisting conditions, a history of statin intolerance, concomitant use of drugs affecting statin metabolism, an age of >75 years, or unexplained elevations in alanine aminotransferase levels >3 times the upper limit of the normal range) should use moderate-intensity statin therapy when high-intensity statin therapy would otherwise be recommended. The 10-year risk of atherosclerotic CVD is calculated with the use of the new risk calculator available at http://my.americanheart.org/cvriskcalculator or at http://www.cardiosource.org/science-and-quality/practice-guidelines-and-quality-standards/2013-prevention-guideline- tools.aspx. LDL denotes low-density lipoprotein, and NYHA New York Heart Association.
 include those with an acute coronary syndrome and those with a history of myocardial infarction, stable or unstable angina, coronary or other arterial revascularization, or stroke, transient ischemic attack, or peripheral arterial disease that is presumed to be of atherosclerotic origin. High-intensity statin therapy is recommended for most patients meeting these criteria. Patients predisposed to adverse statin effects (including those with impaired renal or hepatic function, other serious coexisting conditions, a history of statin intolerance, concomitant use of drugs affecting statin metabolism, an age of >75 years, or unexplained elevations in alanine aminotransferase levels >3 times the upper limit of the normal range) should use moderate-intensity statin therapy when high-intensity statin therapy would otherwise be recommended. The 10-year risk of atherosclerotic CVD is calculated with the use of the new risk calculator available at or at tools.aspx. LDL denotes low-density lipoprotein, and NYHA New York Heart Association..")
26
ACC-AHA guidelines Keaney JF Jr et al. N Engl J Med 2014;370:275-278.

27
ACC-AHA guidelines: key features 4 subgroups of patients eligible Exclusion criteria 1. Age > 75 Y, unless clinical atherosclerotic disease 2. Need for hemodialysis 3. NYHA class II, II or IV Fixed doses of statins (NO non-statin lipid lowering drugs!) Monitoring for muscle or hepatic injury, or diabetes
 Monitoring for muscle or hepatic injury, or diabetes.")
28
ACC-AHA guidelines: implications Avoidance of medication in certain patient groups No LDL-monitoring! No non-statin lipid lowering drugs in statin-tolerant patients Less use of statins in patients> 75 y Use of a new CV risk calculator

29
Overige guidelines Chapter 3: Assessement of lipid status in children with CKD 3.1. In children with newly identified CKD (including those treated with chronic dialysis or kidney transplan-tation), we recommend evaluation with a lipid profile (total cholesterol, LDL cholesterol, HDL cholesterol, triglycerides). (1C) 3.2: In children with CKD (including those treated with chronic dialysis or kidney transplantation), we suggest annual follow-up measurement of fasting lipid levels. (NotGraded)
, we recommend evaluation with a lipid profile (total cholesterol, LDL cholesterol, HDL cholesterol, triglycerides). (1C) 3.2: In children with CKD (including those treated with chronic dialysis or kidney transplantation), we suggest annual follow-up measurement of fasting lipid levels. (NotGraded).")
30
Overige guidelines Chapter 4: Pharmacological cholesterol-lowering treatment in children 4.1. In children less than 18 years of age with CKD (including those treated with chronic dialysis or kidney transplantation), we suggest that statins or statin/ezetimibe combination not be initiated. (2C)
, we suggest that statins or statin/ezetimibe combination not be initiated. (2C).")
31
Overige guidelines Chapter 5: Triglyceride-lowering treatment in adults 5.1. In adults with CKD (including those treated with chronic dialysis or kidney transplantation) and hypertriglyceridemiea, we suggest that therapeutic lifestyle changes be advised. (2D)
 and hypertriglyceridemiea, we suggest that therapeutic lifestyle changes be advised. (2D).")
32
Overige guidelines Chapter 6: Triglyceride-lowering treatment in children 6.1. In children with CKD (including those treated with chronic dialysis or kidney transplantation) and hypertriglyceridemia, we suggest that therapeutic lifestyle changes be advised. (2D)
 and hypertriglyceridemia, we suggest that therapeutic lifestyle changes be advised. (2D).")
Verwante presentaties






>")

![Deltion College Engels En Projectopdracht [Edu/001] thema: research without borders can-do/gesprekken voeren : 1. kan eenvoudige feitelijke informatie.](/9/2250308/big_thumb.jpg "Deltion College Engels En Projectopdracht [Edu/001] thema: research without borders can-do/gesprekken voeren : 1. kan eenvoudige feitelijke informatie.>")

![Deltion College Engels B2 Spreken/presentaties/subvaardigheid lezen [Edu/003] thema: Holland – coffee shops and euthanasia? can-do : kan een duidelijk.](/10/2833741/big_thumb.jpg "Deltion College Engels B2 Spreken/presentaties/subvaardigheid lezen [Edu/003] thema: Holland – coffee shops and euthanasia? can-do : kan een duidelijk.>")
![Deltion College Engels B1 Gesprekken voeren [Edu/006] thema: Look, it says ‘No smoking’… can-do : kan minder routinematige zaken regelen © Anne Beeker.](/10/2924527/big_thumb.jpg "Deltion College Engels B1 Gesprekken voeren [Edu/006] thema: Look, it says ‘No smoking’… can-do : kan minder routinematige zaken regelen © Anne Beeker.>")
![Deltion College Engels B2 Schrijven [Edu/006] thema: Euromail can-do : kan in persoonlijke e-mails nieuws en standpunten van een ander becommentariëren.](/10/2930340/big_thumb.jpg "Deltion College Engels B2 Schrijven [Edu/006] thema: Euromail can-do : kan in persoonlijke e-mails nieuws en standpunten van een ander becommentariëren.>")
![Deltion College Engels C1 Spreken [Edu/002] thema: A book that deserves to be read can-do : kan duidelijke, gedetailleerde samenvatting geven van een gelezen.](/11/3027448/big_thumb.jpg "Deltion College Engels C1 Spreken [Edu/002] thema: A book that deserves to be read can-do : kan duidelijke, gedetailleerde samenvatting geven van een gelezen.>")
![Deltion College Engels B2 Gesprekken voeren [Edu/005]/subvaardigheid luisteren thema: ‘Pink pop and air-controllers on strike’ can-do : kan in een telefoongesprek.](/11/3032113/big_thumb.jpg "Deltion College Engels B2 Gesprekken voeren [Edu/005]/subvaardigheid luisteren thema: ‘Pink pop and air-controllers on strike’ can-do : kan in een telefoongesprek.>")
![Deltion College Engels B1 En Spreken/Presentaties [Edu/006] Thema: “The radio station“ can-do : kan een publiek toespreken, kan verzonnen gebeurtenissen.](/11/3209251/big_thumb.jpg "Deltion College Engels B1 En Spreken/Presentaties [Edu/006] Thema: “The radio station“ can-do : kan een publiek toespreken, kan verzonnen gebeurtenissen.>")
![Deltion College Engels C1 Schrijven [Edu/007] thema: Mind twister or how to write an essay… can-do : kan heldere, goed gestructureerde uiteenzetting schrijven.](/11/3238151/big_thumb.jpg "Deltion College Engels C1 Schrijven [Edu/007] thema: Mind twister or how to write an essay… can-do : kan heldere, goed gestructureerde uiteenzetting schrijven.>")

![Deltion College Engels B2 Lezen [Edu/003] thema: Topical News Lessons: The Onestop Magazine can-do: kan artikelen en rapporten begrijpen die gaan over.](/11/3259133/big_thumb.jpg "Deltion College Engels B2 Lezen [Edu/003] thema: Topical News Lessons: The Onestop Magazine can-do: kan artikelen en rapporten begrijpen die gaan over.>")
![Deltion College Engels B2 Spreken [Edu/001] thema: What’s in the news? can-do : kan verslag doen van een gebeurtenis en daarbij meningen met argumenten.](/11/3263484/big_thumb.jpg "Deltion College Engels B2 Spreken [Edu/001] thema: What’s in the news? can-do : kan verslag doen van een gebeurtenis en daarbij meningen met argumenten.>")
![Deltion College Engels B1 Spreken [Edu/001] thema: song texts can-do : kan een onderwerp dat mij interesseert op een redelijk vlotte manier beschrijven.](/11/3632386/big_thumb.jpg "Deltion College Engels B1 Spreken [Edu/001] thema: song texts can-do : kan een onderwerp dat mij interesseert op een redelijk vlotte manier beschrijven.>")