Download de presentatie
De presentatie wordt gedownload. Even geduld aub

1
Osteomyelitis

2
Osteomyelitis Hematogene verspreiding
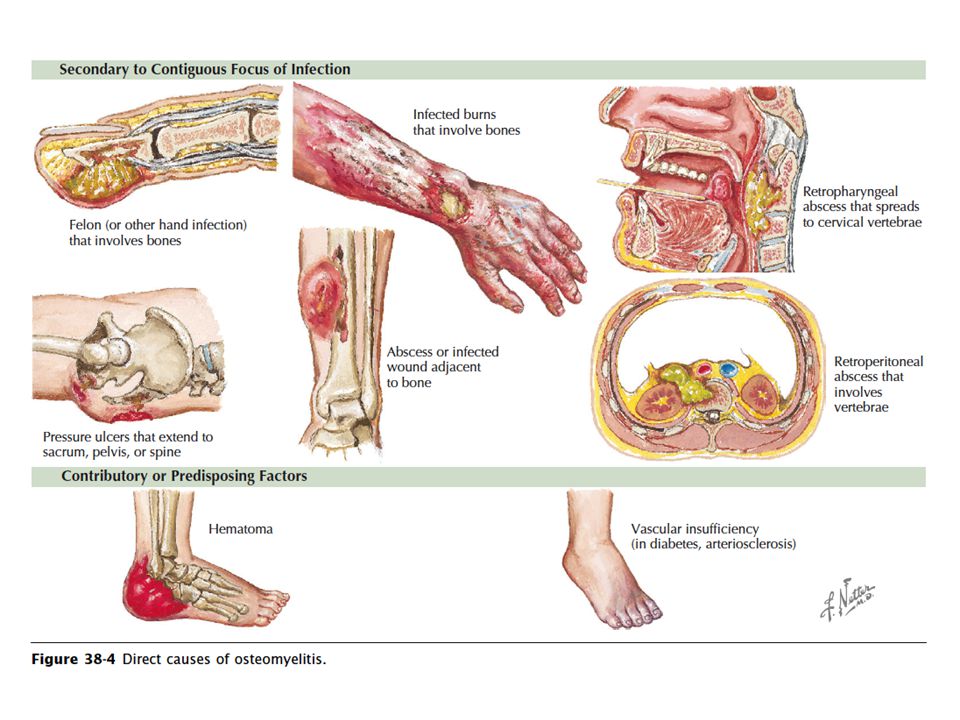
Verspreiding per continuitatum vanuit wekedelen of gewrichten Directe inoculatie t.g.v. trauma of chirurgie

3
Anatomic Classification
II: (Cierny-Mader) 1985 III: IV:
 III: IV:")
5
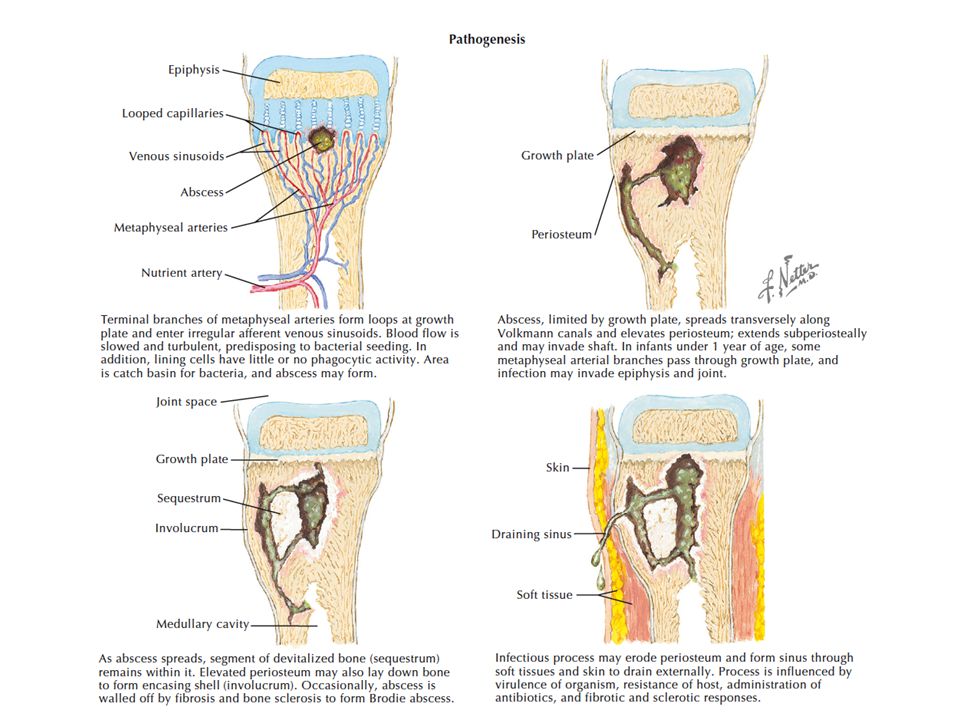
Hematogene osteomyelitis

7
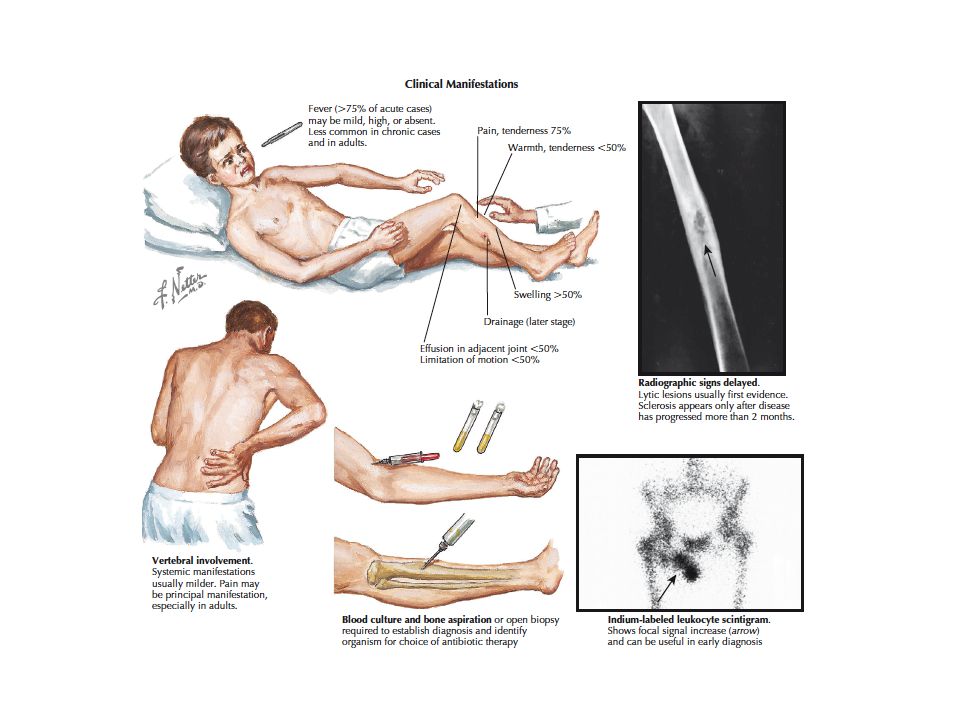
Acute osteomyelitis Meestal in metaphyse
Doorbraak in gewricht septische artritis Metaphyse in gewricht bij knie, heup en schouder

8
Chronische osteomyelitis
De aanwezigheid van een drainerende sinus is pathognomisch voor chronische osteomyelitis Niet helende fracturen en Brodie’s abces Diabetes mellitus Ulcera onderliggende osteomyelitis Als ulcer groter is dan 2 x 2 cm of bot is palpabel is de diagnose osteomyelitis zeer waarschijnlijk

10
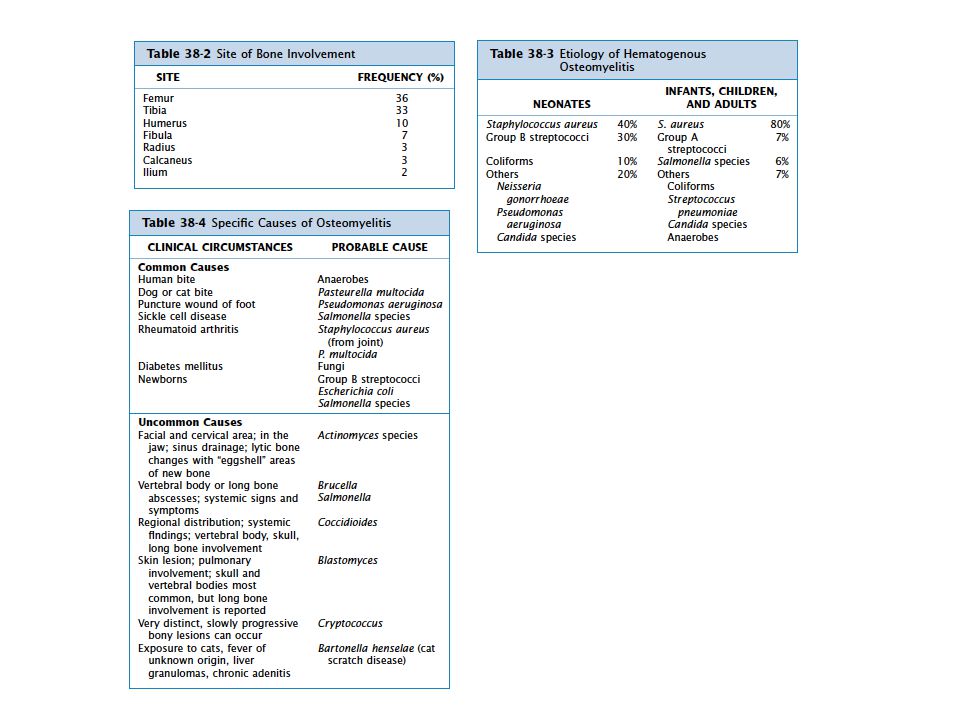
Microbiology of osteomyelitis
Common (>50%) Occasionally (>25%) Rare (<5%) Staphylococcus aureus Streptococci Mycobacterium tuberculosis CNS Enterococci Mycobacterium avium compl. Pseudomonas spp. Atypical mycobacteria Enterobacter spp. Fungi Proteus spp. Candida spp. Escherichia coli Aspergillus spp. Serratia spp. Mycoplasma spp. Anaerobes Tropheryma whipplei Brucella spp. Salmonella spp. Actinomyces spp. Mandell, Douglas and Bennett’s, Principles and practice of infectious diseases, seventh edition
 Occasionally (>25%) Rare (<5%) Staphylococcus aureus. Streptococci. Mycobacterium tuberculosis. CNS. Enterococci. Mycobacterium avium compl. Pseudomonas spp. Atypical mycobacteria. Enterobacter spp. Fungi. Proteus spp. Candida spp. Escherichia coli. Aspergillus spp. Serratia spp. Mycoplasma spp. Anaerobes. Tropheryma whipplei. Brucella spp. Salmonella spp. Actinomyces spp. Mandell, Douglas and Bennett’s, Principles and practice of infectious diseases, seventh edition.")
12
Diagnostiek Een accurate diagnose van osteomyelitis is cruciaal gezien de langdurige behandeling met antibiotica en de eventuele “aggressieve” chirurgische debridement.

13
Diagnostiek Microbiologie Pathologie Beeldvorming: Gewone röntgenfoto
MRI Bot scan PET CT Open chirurgisch biopt of naaldbiopsie

14
Beeldvorming Op gewone x-foto zijn afwijkingen te zien 10 tot 14 dagen na de start van infectie

15
MRI X-foto Figure 1. Plain film radiograph of spinal discitis / osteomyelitis. Lateral view of the lumbar spine demonstrates L 3-4 disc space narrowing (arrow) and end-plate irregularity. Figure 2. MRI of lumbar spine discitis/osteomyelitis. A. Sagittal T1-weighted images of the lumbar spine in the same patient as figure 1 demonstrate T1-hypointense signal (solid arrows) centered around the L3-4 interspace. B. Post gadolinium sagittal fat-suppressed T1-weighted images shows marrow (dashed arrows) and disc enhancement with endplate erosions.
 and end-plate irregularity. Figure 2. MRI of lumbar spine discitis/osteomyelitis. A. Sagittal T1-weighted images of the lumbar spine in the same patient as figure 1 demonstrate T1-hypointense signal (solid arrows) centered around the L3-4 interspace. B. Post gadolinium sagittal fat-suppressed T1-weighted images shows marrow (dashed arrows) and disc enhancement with endplate erosions.")
16
PET-CT An 11-y-old boy with history of X-linked chronic granulomatous disease who underwent 18F-FDG PET/CT as part of his work-up. Coronal PET image demonstrates several areas of osteomyelitis (both feet and distal right femur) (O), several soft-tissue sites of inflammation (left forearm, left femur, and both shins) (I), pneumonia (P), and paratracheal and hilar adenopathy (A). FDG = Fluorine 18 fluorodeoxyglucose
 (O), several soft-tissue sites of inflammation (left forearm, left femur, and both shins) (I), pneumonia (P), and paratracheal and hilar adenopathy (A). FDG = Fluorine 18 fluorodeoxyglucose.")
17
Microbiologie Afname materiaal voor kweek Bloedkweken
Open chirurgische biopsie Naald biopsie Bloedkweken

18
Speciale kweken Mycobacterium tuberculosis Schimmels en gisten
Brucella

19
Therapie Chirurgische debridement Antibiotica (langdurig)
Plus eventueel: Verwijderen van “hardware” Revascularisatie Complete sluiting wond (spierflap) Stabiliteit waarborgen bij evt. fracturen Antibiotica (langdurig) Iv of oraal? Duur?
 Stabiliteit waarborgen bij evt. fracturen. Antibiotica (langdurig) Iv of oraal Duur")
20
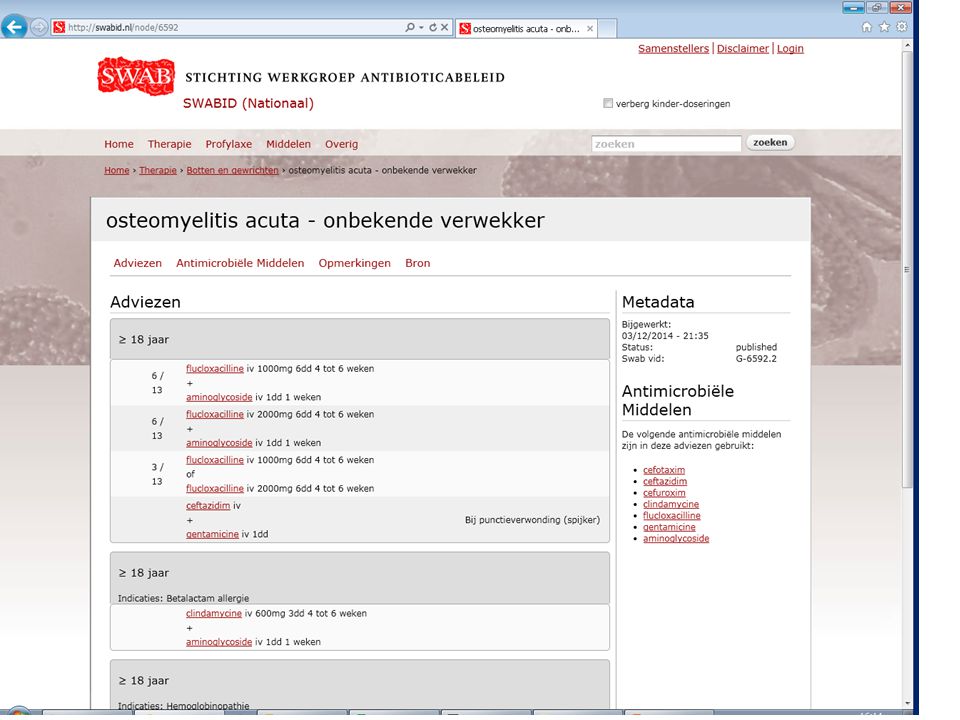
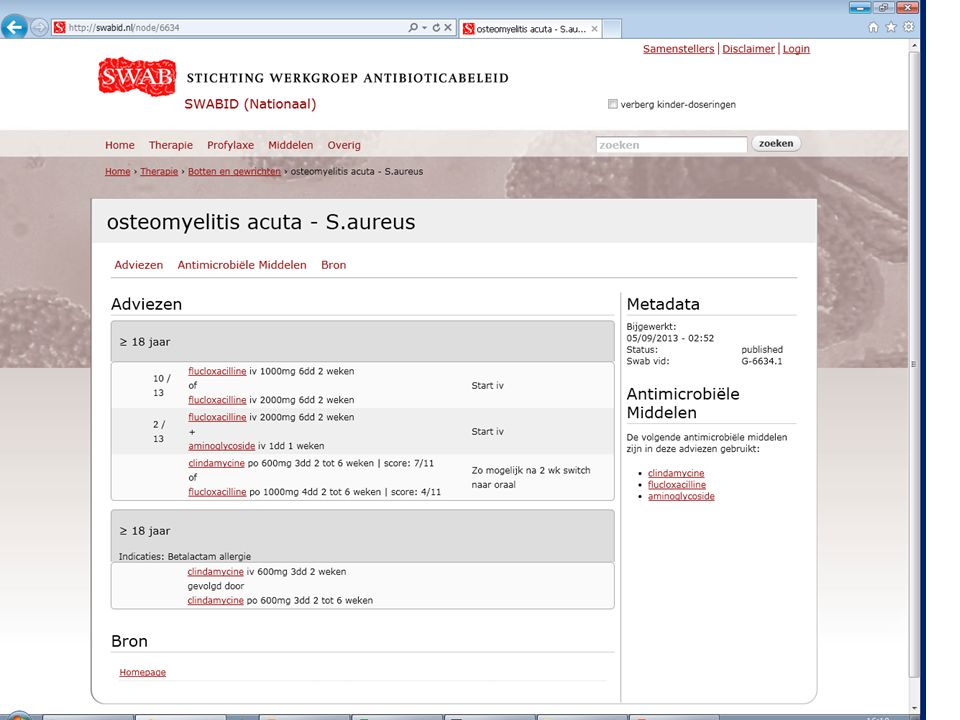
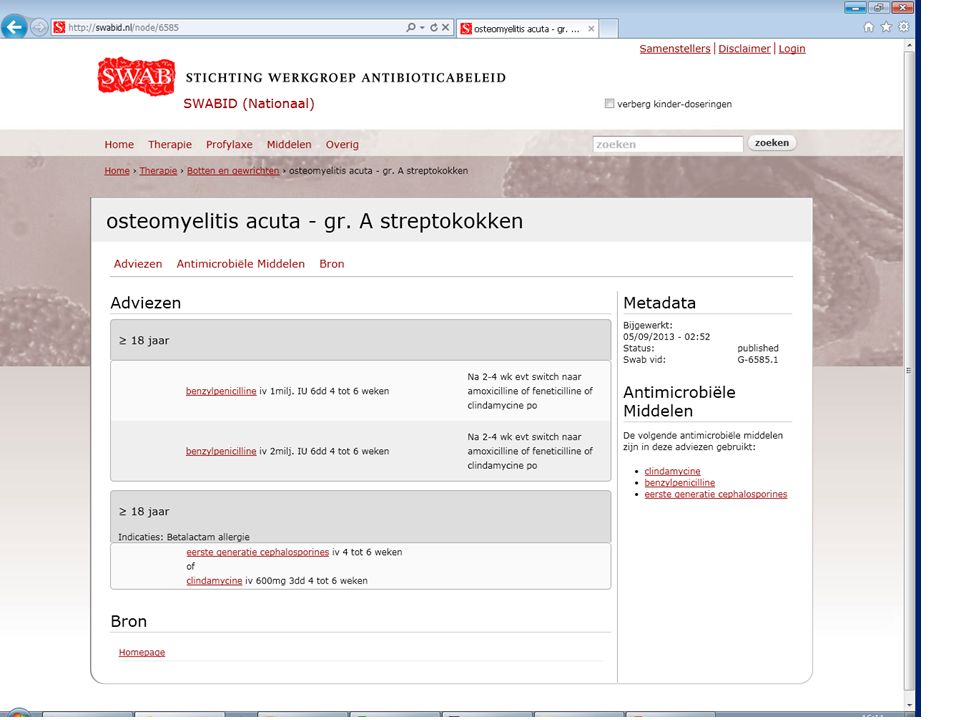
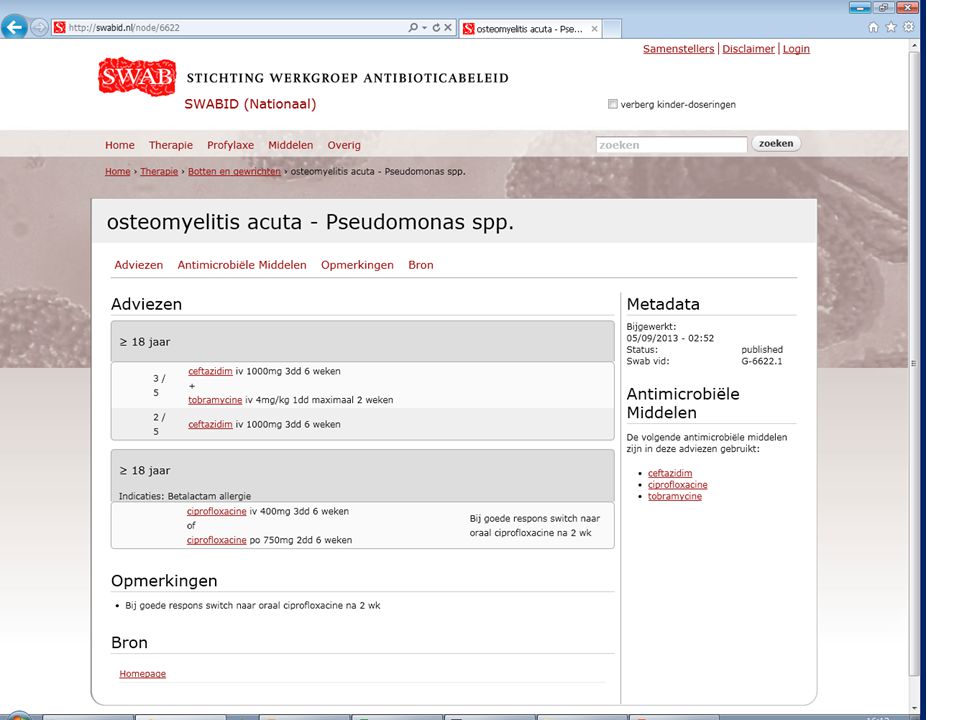
ZGV Acute hematogene osteomyelitis: verwekker onbekend flucloxacilline, clindamycine verwekker bekend S aureus: flucloxacilline, clindamycine Streptokokken: peni, clindamycine Pseudomonas: cefta + genta, cipro

25
ZGV Na trauma of per continuitatem verwekker onbekend geen perifere vaataandoening Flucloxacilline, clindamycine wel perifere vaataandoening clindamycine + /- cipro

28
Casus Dhr R 52 jr. Charcot osteoarthropathie voet
Ulcus met osteomyelitis Bloedkweken: Streptococcus agalactiae Wondkweek: Stapylococcus aureus HSC Amoxicilline/ clavulaanzuur iv.

31
Kweken Bloedkweek Wondkweek

32
Vervolg casus Allergie clindamycine Vragen:
Is oraal behandelen mogelijk? Welke orale opties zijn er? Is er bewijs voor toegevoegde waarde van rifampicine?

33
Review CID CID 2012:54 (1 february)
")
34
Problemen chronische osteomyelitis
Geen goede representatieve kweken Vaak “Delay” in behandeling Therapiefalen

35
Parenterale antibiotica
Botpenetratie beta-lactams 5-20% serumspiegels IV betalactam botspiegels > MIC Orale dosering beta-lactam AB < 10% iv serumspiegels botspiegels < MIC

36
Parenterale antibiotica
Vancomycine lage penetratie in bot Hoge serumspiegels botspiegels > MIC Daptomycine idem.

37
Orale antibiotica AB met goede penetratie in botweefsel:
Fluoroquinolonen ± 30-60% van serumspiegels Linezolid ± 50% Trimethoprim ± 50% Sulfamethoxazol ± 10-20% Doxycycline ± 2-86% afhankelijk welk bot Clindamycine ± 40-70% Metronidazol ± % Rifampicine > 100% Fusidinezuur ± 40-90% Fosfomycine ± 25%

38
Gerandomiseerde studies AB behandeling chronische osteomyelitis
8 kleine studies totaal N=228 5 studies vergelijken iv met oraal Geen significante verschillen in uitkomst na 12 maanden Bijwerkingen iv vs oraal 15,5% vs 4,8%

39
Rifampicine 2 studies met toevoeging rifampicine bij chronische osteomyelitis S. aureus Uitkomst beter in rifampicine groep Genezing17 van 20 vs 12 van 21 Zimmerli: geïnfecteerde prothesen Cipro + rifamp vs cipro mono 3-6 mnd Genezing 100% vs 58% 4 van 5 pt met therapiefalen ontw. cipro R

40
Gerandomiseerde studies co-trimoxazol
Cloxacillin vs co-trim + rifamp bij S. aureus N=50 8 weken 20 patiënten met prothese “Cure rate” 91% vs 89% Follow-up 10 jr. “relaps rate” 10% vs 11%

41
Opmerkingen Weinig hard bewijs bij AB behandeling chronische osteomyelitis Studies met lage aantallen en heterogene groepen Minder studies voor iv dan orale AB

42
Conclusies Orale behandeling met oraal AB met goede penetratie bot lijkt acceptabel Ciprofloxacine 2dd750mg Co-trimoxazol 7-10 mg/kg/dg (trimethoprim) Clindamycine, doxycycline, Linezolid Toevoeging rifampicine alleen bewezen effect bij S. aureus Geen evidence voor duur therapie (na chirurgische debridement)
 Clindamycine, doxycycline, Linezolid. Toevoeging rifampicine alleen bewezen effect bij S. aureus. Geen evidence voor duur therapie (na chirurgische debridement)")
43
Vervolg casus Bloedkweek Wondkweek

44
Behandeling? Chirurgische debridement met sluiten defect mogelijk?
Beste orale optie co-trimoxazol? Rifampicine toevoegen? In 25% gevallen DM en osteomyelitis) toch amputatie… Vragen en discussie
 toch amputatie… Vragen en discussie.")
Verwante presentaties




 -20 % van een de patiënten met een 1 ste gebeurtenis.>")







>")








