Download de presentatie
De presentatie wordt gedownload. Even geduld aub

1
GIST: gisteren, vandaag en morgen
10e Contactdag dd A.K.L. Reyners Internist-oncoloog UMCG

2
GISTEREN Gisteren

3
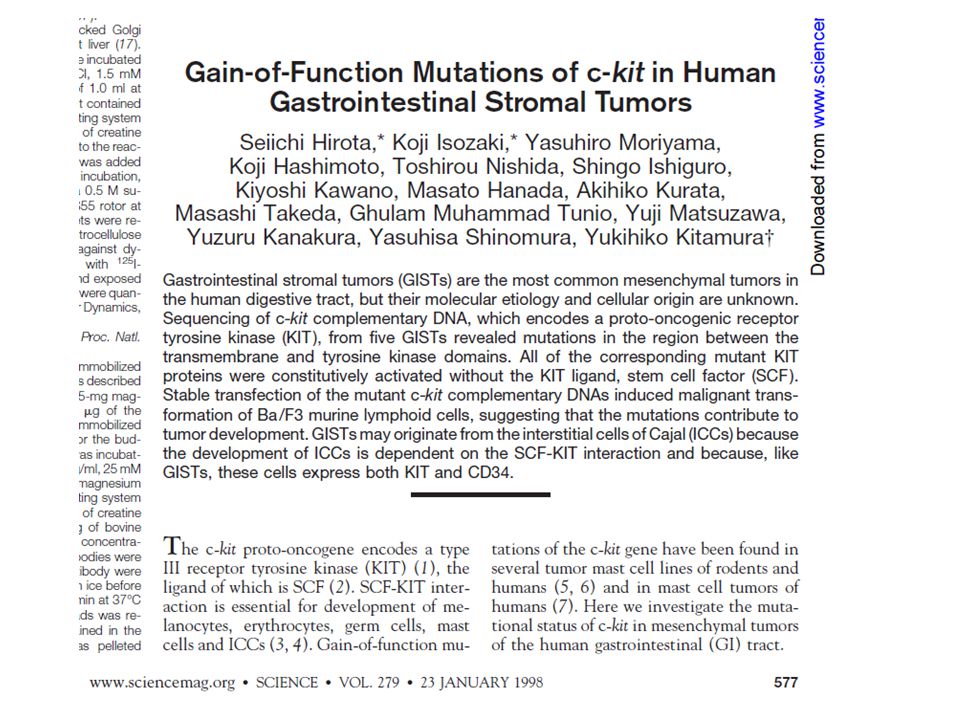
GastroIntestinale Stroma Tumor

4
GIST Subtype sarcoom Man:vrouw verhouding Vooral in 5e – 7e decade
0.2% van de gastrointestinale tumoren nieuwe patiënten per jaar (Europa en US) Man:vrouw verhouding Vooral in 5e – 7e decade [slide 2] Gastrointestinal Stromal Tumours (GISTs)1 GISTs represent a rare subset of sarcoma (tumour of mesenchymal origin) that develops in the gastrointestinal (GI) tract and may spread within the abdomen. GISTs are rare neoplasms, representing less than 1% of all tumours of the GI tract; nonetheless, GISTs are the most common mesenchymal malignancy of the GI tract. Approximately 3000 to 5000 cases of GI sarcoma occur annually in the United States. Men and women are affected equally, and it is unusual to find GISTs in patients less than 40 years of age. The peak incidence seems to occur during the 5th to 7th decades of life. The definition of GIST is evolving; it has recently been described as a distinct clinical and histopathological entity. Reference: 1. Miettinen M, Sarlomo-Rikala M, Lasota J. Gastrointestinal stromal tumors: recent advances in understanding of their biology. Hum Pathol ;30:
 Man:vrouw verhouding. Vooral in 5e – 7e decade. [slide 2] Gastrointestinal Stromal Tumours (GISTs)1. GISTs represent a rare subset of sarcoma (tumour of mesenchymal origin) that develops in the gastrointestinal (GI) tract and may spread within the abdomen. GISTs are rare neoplasms, representing less than 1% of all tumours of the GI tract; nonetheless, GISTs are the most common mesenchymal malignancy of the GI tract. Approximately 3000 to 5000 cases of GI sarcoma occur annually in the United States. Men and women are affected equally, and it is unusual to find GISTs in patients less than 40 years of age. The peak incidence seems to occur during the 5th to 7th decades of life. The definition of GIST is evolving; it has recently been described as a distinct clinical and histopathological entity. Reference: 1. Miettinen M, Sarlomo-Rikala M, Lasota J. Gastrointestinal stromal tumors: recent advances in understanding of their biology. Hum Pathol. 1999;30:")
5
Gisteren Operatie is DE behandeling 5-jaars overleving 50% tot 65%
Recidief kan pas na meer dan 10 jaar optreden! Na incomplete resectie / uitzaaingen bij presentatie Gemiddelde overleving <1 jaar 5-jaars overleving <35% [slide 13] Traditional Treatment Options Pre-Imatinib Mesylate1-4 Surgery is the primary treatment modality for GISTs. Tumours should be completely resected at the initial surgery. Patients with grossly positive margins or unresectable disease have a median survival of only 9 to 12 months. For patients who undergo complete resection, there is high likelihood of recurrence within the abdomen. Median time to recurrence is 7 months to 2 years; the probability of recurrence after re-excision approaches 100%. In a large series of GISTs with adequate follow-up, surgical resection led to 50% to 65% 5-year disease-free survival. Surgical cures are much more common when incidentally discovered GISTs are included in the data. These asymptomatic tumours are often small, with benign histological features, and sometimes may be evident only on pathological examination of a specimen removed for another reason (eg, microleiomyomas). As most GISTs are asymptomatic until very large, less than 50% of the tumours can be completely resected at presentation. Overall, 5-year survival for high-risk GISTs varies widely, and has been reported as anywhere between 30% and 80%. Recurrences have been reported up to 20 years after primary surgery. In patients who present with metastases or have unresectable disease, the median survival is less than 1 year, and the 5-year survival rates are less than 35%. References: 1. Pierie JP, Choudry U, Muzikansky A, et al. The effect of surgery and grade on outcome of gastrointestinal stromal tumors. Arch Surg ;136: 2. Miettinen M, Sarlomo-Rikala M, Lasota J. Gastrointestinal stromal tumors: recent advances in understanding of their biology. Hum Pathol ;30: 3. Hatch KF, Blanchard DK, Hatch GF III, et al. Tumors of the rectum and anal canal. World J Surg. 2000;24: 4. Plaat BE, Hollema H, Molenaar WM, et al. Soft tissue leiomyosarcomas and malignant gastrointestinal stromal tumors: differences in clinical outcome and expression of multidrug resistance proteins. J Clin Oncol ;18:
. As most GISTs are asymptomatic until very large, less than 50% of the tumours can be completely resected at presentation. Overall, 5-year survival for high-risk GISTs varies widely, and has been reported as anywhere between 30% and 80%. Recurrences have been reported up to 20 years after primary surgery. In patients who present with metastases or have unresectable disease, the median survival is less than 1 year, and the 5-year survival rates are less than 35%. References: 1. Pierie JP, Choudry U, Muzikansky A, et al. The effect of surgery and grade on outcome of gastrointestinal stromal tumors. Arch Surg. 2001;136: Miettinen M, Sarlomo-Rikala M, Lasota J. Gastrointestinal stromal tumors: recent advances in understanding of their biology. Hum Pathol. 1999;30: Hatch KF, Blanchard DK, Hatch GF III, et al. Tumors of the rectum and anal canal. World J Surg. 2000;24: Plaat BE, Hollema H, Molenaar WM, et al. Soft tissue leiomyosarcomas and malignant gastrointestinal stromal tumors: differences in clinical outcome and expression of multidrug resistance proteins. J Clin Oncol. 2000;18:")
6
Gisteren Chemotherapie is niet werkzaam response rate: <10%
Geen overlevingsvoordeel GISTs zijn niet gevoelig voor radiotherapie response rate: <5% [slide 14] Traditional Treatment Options Pre-Imatinib Mesylate (cont.)1-4 Multiple chemotherapeutic regimens have been used to treat residual, recurrent, or metastatic disease, with uniformly poor results. Randomised trials of doxorubicin, ifosfamide, and other combination agents have had response rates of less than 10%. The expression of multidrug-resistant proteins is more pronounced in GISTs than in soft tissue leiomyosarcomas, which may relate to their low response to chemotherapy and poor survival rates. In spite of the poor chemotherapeutic response rates, most patients with metastatic disease undergo multiple courses of chemotherapy, because no other treatment options exist. Radiation therapy is rarely used for GISTs, because of the radiation sensitivity of adjacent organs and the relative radioresistance of these tumours. Malignant rectal GISTs are occasionally treated with neoadjuvant radiation therapy; however, data supporting neoadjuvant radiation therapy are unavailable given the rarity of rectal GISTs. Treatment options for metastatic lesions are even more limited. Surgical resection of metastases is often performed; however, there are no survival data supporting this practice. Most high-risk GISTs do not respond to radiotherapy and/or chemotherapy and are ultimately fatal. References: 1. Pierie JP, Choudry U, Muzikansky A, et al. The effect of surgery and grade on outcome of gastrointestinal stromal tumors. Arch Surg ;136: 2. Miettinen M, Sarlomo-Rikala M, Lasota J. Gastrointestinal stromal tumors: recent advances in understanding of their biology. Hum Pathol ;30: 3. Hatch KF, Blanchard DK, Hatch GF III, et al. Tumors of the rectum and anal canal. World J Surg. 2000;24: 4. Plaat BE, Hollema H, Molenaar WM, et al. Soft tissue leiomyosarcomas and malignant gastrointestinal stromal tumours: differences in clinical outcome and expression of multidrug resistance proteins. J Clin Oncol ;18:
1-4. Multiple chemotherapeutic regimens have been used to treat residual, recurrent, or metastatic disease, with uniformly poor results. Randomised trials of doxorubicin, ifosfamide, and other combination agents have had response rates of less than 10%. The expression of multidrug-resistant proteins is more pronounced in GISTs than in soft tissue leiomyosarcomas, which may relate to their low response to chemotherapy and poor survival rates. In spite of the poor chemotherapeutic response rates, most patients with metastatic disease undergo multiple courses of chemotherapy, because no other treatment options exist. Radiation therapy is rarely used for GISTs, because of the radiation sensitivity of adjacent organs and the relative radioresistance of these tumours. Malignant rectal GISTs are occasionally treated with neoadjuvant radiation therapy; however, data supporting neoadjuvant radiation therapy are unavailable given the rarity of rectal GISTs. Treatment options for metastatic lesions are even more limited. Surgical resection of metastases is often performed; however, there are no survival data supporting this practice. Most high-risk GISTs do not respond to radiotherapy and/or chemotherapy and are ultimately fatal. References: 1. Pierie JP, Choudry U, Muzikansky A, et al. The effect of surgery and grade on outcome of gastrointestinal stromal tumors. Arch Surg. 2001;136: Miettinen M, Sarlomo-Rikala M, Lasota J. Gastrointestinal stromal tumors: recent advances in understanding of their biology. Hum Pathol. 1999;30: Hatch KF, Blanchard DK, Hatch GF III, et al. Tumors of the rectum and anal canal. World J Surg. 2000;24: Plaat BE, Hollema H, Molenaar WM, et al. Soft tissue leiomyosarcomas and malignant gastrointestinal stromal tumours: differences in clinical outcome and expression of multidrug resistance proteins. J Clin Oncol. 2000;18:")
8
GIST: CD117 positief

9
Imatinib

11
Maart 2001: NEJM

12
Mei 2001:

14
Vandaag

15
Vandaag 5 GIST centra in Nederland

16
Accrual in EORTC trial 62005

17
Behandelingen Neo-adjuvant: voor operatie Adjuvant: na operatie
Palliatief

18
Behandelingen Neo-adjuvant: imatinib Adjuvant: imatinib
Palliatief: 1.imatinib 2.sunitinib (3.regorafenib)
")
19
Palliatief – imatinib (fase 2)
Complete response (CR) 0 Partial response (PR) 79 (53.7) Stable disease (SD) 41(27.9) Progressive disease (PD) 20 (13.6) Nonevaluable 7 (5) [slide 47] GIST Phase II: Best Confirmed Responses1 Overall, 40% of patients achieved a confirmed PR. PR: 50% to 99% decrease from baseline of all measurable disease, no progression of evaluable disease (<2 cm), and no new lesions.2 No patient achieved a CR. CR: complete disappearance of all measurable (>2 cm) and evaluable (<2 cm) disease with no new lesions. Any symptoms attributed to the tumour must be resolved.2 SD was confirmed in 41% of patients, and only 12% of patients experienced PD. SD or no response: a response that does not qualify as CR, PR, PD, or unknown. SD, therefore, may be a lesion that stays as is or decreases from 0% to 49% from baseline, or increases 0% to 49% from baseline.2 PD: an increase of 50% or 10 cm2 of all measurable lesions, or clear worsening from previous assessment of any evaluable disease, or reappearance of lesion that had disappeared, or failure to return for evaluation due to death or deterioration.2 Approximately 80% of the patients in this trial benefitted from imatinib therapy through either reduction or stabilisation of their GIST lesion. References: 1. Data on file. Novartis Pharma AG, Basel, Switzerland. 2. Green S, Weiss GR. Southwest Oncology Group standard response criteria, endpoint definitions and toxicity criteria. Invest New Drugs ;10: Demetri GD et al.NEJM 2002;347(7):
 0. Partial response (PR) 79 (53.7) Stable disease (SD) 41(27.9) Progressive disease (PD) 20 (13.6) Nonevaluable 7 (5) [slide 47] GIST Phase II: Best Confirmed Responses1. Overall, 40% of patients achieved a confirmed PR. PR: 50% to 99% decrease from baseline of all measurable disease, no progression of evaluable disease (<2 cm), and no new lesions.2. No patient achieved a CR. CR: complete disappearance of all measurable (>2 cm) and evaluable (<2 cm) disease with no new lesions. Any symptoms attributed to the tumour must be resolved.2. SD was confirmed in 41% of patients, and only 12% of patients experienced PD. SD or no response: a response that does not qualify as CR, PR, PD, or unknown. SD, therefore, may be a lesion that stays as is or decreases from 0% to 49% from baseline, or increases 0% to 49% from baseline.2. PD: an increase of 50% or 10 cm2 of all measurable lesions, or clear worsening from previous assessment of any evaluable disease, or reappearance of lesion that had disappeared, or failure to return for evaluation due to death or deterioration.2. Approximately 80% of the patients in this trial benefitted from imatinib therapy through either reduction or stabilisation of their GIST lesion. References: 1. Data on file. Novartis Pharma AG, Basel, Switzerland. 2. Green S, Weiss GR. Southwest Oncology Group standard response criteria, endpoint definitions and toxicity criteria. Invest New Drugs. 1992;10: Demetri GD et al.NEJM 2002;347(7):")
20
Palliatief - imatinib

21
Palliatief - imatinib

22
Before imatinib After imatinib June 27, 2000 October 4, 2000
[slide 50] CT Scan Results: Decrease in Tumour Volume1 Transaxial CT scan of the abdomen. Before imatinib therapy (left panel), this large GIST tumour was a protuberant mass in the lower abdomen. After 1 month of treatment with imatinib (right panel), the tumour size decreased considerably. There is a residual mass in the pelvis. Reference: 1. Demetri GD, von Mehren M, Blanke CD, et al. Antitumor effects of an oral selective tyrosine kinase inhibitor, imatinib mesylate, in patients with advanced gastrointestinal stromal tumors. N Engl J Med In press.
, this large GIST tumour was a protuberant mass in the lower abdomen. After 1 month of treatment with imatinib (right panel), the tumour size decreased considerably. There is a residual mass in the pelvis. Reference: 1. Demetri GD, von Mehren M, Blanke CD, et al. Antitumor effects of an oral selective tyrosine kinase inhibitor, imatinib mesylate, in patients with advanced gastrointestinal stromal tumors. N Engl J Med In press.")
23
CT en PET Scan Resultaten
July 3, 2000 October 5, 2000 Before imatinib After imatinib [slide 51] Comparison of CT and PET Scan Results1 A hepatic metastasis imaged with CT scan and 18FDG-PET before treatment with imatinib and 1 month after treatment initiation. A decrease in tumour size noted on the CT scan image. Concomitantly, a marked decrease in glycolytic activity of the many metastases is evident in the PET scan after imatinib therapy. Reference: 1. Data on file. Novartis Pharma AG, Basel, Switzerland.

24
Lange termijn - imatinib
147 US/Finland mediane follow up 34 maanden 67% PR en 16% SD 84% PR na 1 jaar mediane respons 30 maanden

25
GIST: mutatie analyse

26
Palliatief - imatinib Heinrich M C et al. JCO 2008;26:5360-5367
Correlation of gastrointestinal stromal tumor (GIST) genotype and time to progression or overall survival for patients with CD117-positive GISTs. Heinrich M C et al. JCO 2008;26:
 genotype and time to progression or overall survival for patients with CD117-positive GISTs. Heinrich M C et al. JCO 2008;26:")
27
Mutaties en respons 88% KIT mutaties 76% exon 11: 84% PR
4.7% PDGFRA mutaties: 0-67% PR Overig geen mutatie:0% PR, 35% SD

28
Resistentie Target Dosering van de drug

29
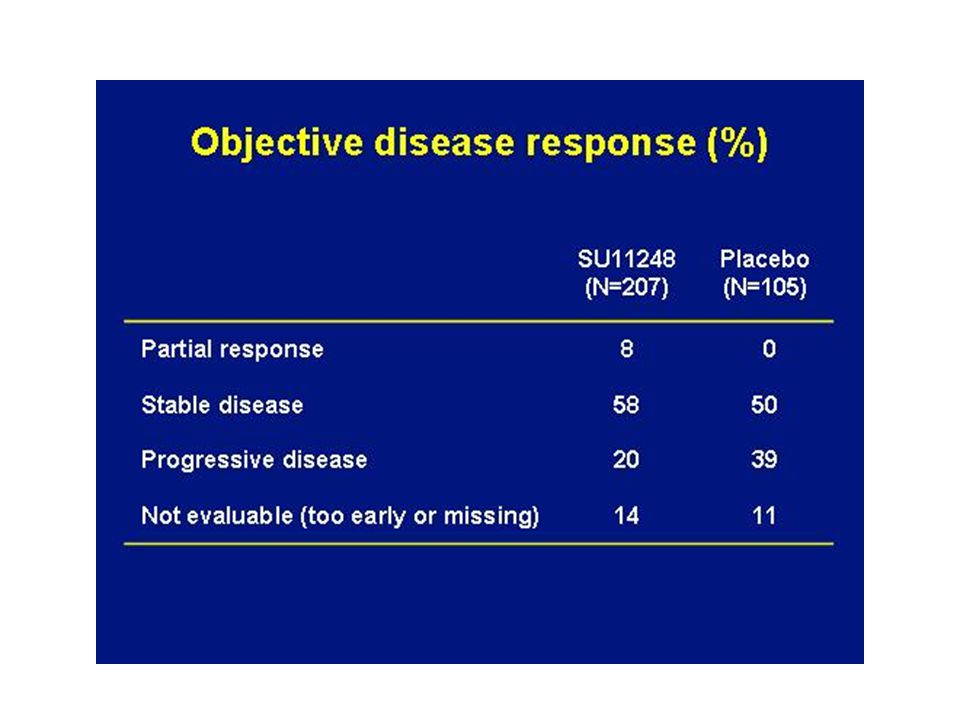
Palliatief - sunitinib
50 mg/d 4 wk op, wk af 2:1 Randomisatie Crossover naar SU11248 bij progressie Placebo Based on the SU11248 activity seen in phase I/II studies in GIST, a phase III trial has begun. In this trial, 357 patients with imatinib-resistant GIST will be randomized 2:1 to: 2: SU11248, 50 mg/d, 4 weeks on, 2 weeks off 1: Placebo At progression, patients who had been randomized to placebo will receive SU11248, and those who had been randomized to SU11248 will leave the study. Primary end point is time to tumor progression. doel: N = 357 Primair eindpunt: TTP

30
Palliatief - sunitinib

31
Risicoclassificatie Miettinen-Lasota
Tumor karakteristieken Percentage patiënten met recidief Groep Grootte Mitosen maag jejunum/ileum duodenum rectum 1 ≤2 cm ≤5/50 HPF 0% 2 2-5 cm 1.9% 4.3% 8.3% 8.5% 3a 5-10 cm 3.6% 24% 34% 57% 3b >10 cm 12% 52% 4 >5/50 HPF 50% 54% 5 16% 73% 6a 55% 85% 86% 71% 6b 90% Seminars in diagnostic pathology 2008; 23;70-83.

32
JAMA 2012: resultaten

33
JAMA 2012: resultaten

34
Nederlandse richtlijn
Bij patiënten met meer dan 50% kans op metastasen volgens een van de huidig beschikbare risicotabellen geldt dus het advies 3 jaar adjuvant te behandelen. Indien de patiënt neoadjuvante behandeling met imatinib heeft gehad dan wordt deze periode meegeteld in de totale duur van 3 jaar. Het advies is patiënten die in aanmerking komen voor adjuvante behandeling te verwijzen naar een centrum voor mutatieanalyse en behandeling. Patiënten met imatinib resistente tumoren komen niet in aanmerking voor behandeling.

35
Morgen

36
Palliatief - regorafenib
Percent control 0% 0.1% 0.1-1% 1-5% 5-10% 10-35% Wilhelm SM et al. Int J Cancer 2011; 129:

37
Palliatief - regorafenib

38
Behandeling aangepast
De toekomst Behandeling aangepast aan de persoon en aan de tumorkenmerken in de loop van de tijd

39
De toekomst

42
Adjuvant - imatinib

43
GRID studie 43 2 : 1 Regorafenib + best supportive care (BSC)
160 mg once daily 3 weeks on, 1 week off (n=133) Placebo + BSC 3 weeks on, 1 week off (n=66) RANDOM I ZAT I ON Metastatic/ unresectable GIST patients progressing despite at least prior imatinib and sunitinib (n=236 screened; n=199 randomized) Disease progression per independent blinded central review OF F TREATMENT Unblinding Crossover offered for placebo arm or continued regorafenib for treatment arm Regorafenib (unblinded) until next progression Best supportive care includes any method to preserve the comfort and dignity of the patient, excluding disease-specific antineoplastic therapy, such as any kinase inhibitor, chemotherapy, radiotherapy, or surgical intervention. 43
 Placebo + BSC 3 weeks on, 1 week off (n=66) RANDOM I ZAT I ON. Metastatic/ unresectable GIST patients progressing despite at least prior imatinib and sunitinib. (n=236 screened; n=199 randomized) Disease progression. per independent blinded central review. OF F. TREATMENT. Unblinding. Crossover offered for placebo arm or continued regorafenib for treatment arm. Regorafenib (unblinded) until next progression. Best supportive care includes any method to preserve the comfort and dignity of the patient, excluding disease-specific antineoplastic therapy, such as any kinase inhibitor, chemotherapy, radiotherapy, or surgical intervention. 43.")
44
Palliatief - regorafenib

Verwante presentaties










morgen>")










