Download de presentatie
De presentatie wordt gedownload. Even geduld aub

2
Systemische therapie: zijn alle doelen nu bereikt?
Dr. Yvonne Kamm internist-oncoloog UMC St Radboud Nijmegen NABON / BOOG 2008

3
Onderwerpen Hormonale therapie: Hoe lang? Tamoxifen of AI? - HST
- CYP2D6 en Tamoxifen Targeted therapie: Trastuzumab Lapatinib Pertuzumab NABON / BOOG 2008

4
ATLAS-trial Adjuvant Tamoxifen, Longer Against Shorther
Internationale gerandomiseerde trial 10 vs 5 jaar tamoxifen vrouwen – voorlopige resultaten Peto, SABCS 2007 NABON / BOOG 2008

5
ER-status en compliance
ER niet getest 41% → gedeelte ER+ ~ 90%, niet 100% Hormonale behandeling 2 jaar na randomisatie 83% v 4% → verschil ~ 80%, niet 100% NABON / BOOG 2008

6
Mogelijke verdere effecten 10 v 5 jaar tamoxifen in ER+
Als (100%) 10 v 5 & (100%) ER+ Als 80% compliance & 90% ER+ Jaren vanaf Diagnose Rel. risico recidief 10 v 5 jaar tamoxifen (se) 5-9 0.83 0.88 (+/- 0.05) 10-14 0.7 0.78 (+/- 0.12) NABON / BOOG 2008
 10 v 5. & (100%) ER+ Als 80% compliance. & 90% ER+ Jaren. vanaf. Diagnose. Rel. risico recidief. 10 v 5 jaar tamoxifen. (se) (+/- 0.05) (+/- 0.12) NABON / BOOG")
7
ATAC-trial ‘Arimidex’, Tamoxifen, Alone or in Combination
Analyse effectiviteit en veiligheid 100-maanden mediane follow-up Anastrozole v Tamoxifen Forbes, SABCS 2007 NABON / BOOG 2008

8
ATAC trial design Postmenopausal women with invasive breast cancer
Surgery radiotherapy chemotherapy Randomisation 1:1:1 for 5 years Anastrozole (n = 3125) Tamoxifen (n = 3116) Discontinued following initial analysis as no efficacy or tolerability benefit compared with tamoxifen arm Combination n=3125 The ATAC trial was designed to compare anastrozole (1 mg/day) with tamoxifen (20 mg/day), alone or in combination. At a planned interim analysis (median follow-up of 33 months), no additional benefits could be found in the combination arm over the monotherapy arms and so the combination arm was closed. ITT population n = 3125 Safety population n = 3092 HR+ subpopulation n = 2618 ITT population n = 3116 Safety population n = 3094 HR+ subpopulation n = 2598 ITT, intent-to-treat; HR+, hormone receptor-positive NABON / BOOG 2008
 Tamoxifen (n = 3116) Discontinued following initial analysis as no efficacy or tolerability benefit compared with tamoxifen arm. Combination. n=3125. The ATAC trial was designed to compare anastrozole (1 mg/day) with tamoxifen (20 mg/day), alone or in combination. At a planned interim analysis (median follow-up of 33 months), no additional benefits could be found in the combination arm over the monotherapy arms and so the combination arm was closed. ITT population n = Safety population. n = HR+ subpopulation n = ITT population n = Safety population. n = HR+ subpopulation n = ITT, intent-to-treat; HR+, hormone receptor-positive. NABON / BOOG")
9
Efficacy endpoints for all patients and HR+ patients
All patients (ITT) HR+ patients Favours anastrozole (A) Favours tamoxifen (T) Hazard ratio Hazard ratio All patients HR+ patients Disease-free survival 0.90 0.85 Time to recurrence 0.81 0.76 Time to distant recurrence 0.86 0.84 Contralateral breast cancer 0.68 0.60 The ATAC trial demonstrated that anastrozole was consistently superior to tamoxifen for all efficacy endpoints except overall survival, death after recurrence and death without recurrence where no significant change was observed. Anastrozole has proven superiority over tamoxifen, in terms of significant reduction in all forms of recurrence, ensuring that women can live cancer-free for longer. Overall survival, after a median follow-up of 100 months, is similar for both anastrozole and tamoxifen. Anastrozole reduces the risk of death following recurrence by 10% Although currently not statistically significant (p=0.2), there is a 90% chance that time to death following recurrence is longer with anastrozole. Deaths without recurrence were slightly but not significantly higher in the anastrozole group but no specific cause of death was elevated; most likely this is due to play of chance. There was no evidence of increased cardiovascular mortality or morbidity. This makes it difficult to show a benefit when patients are dying from other causes by virtue of their old age (mean age 72 years) Death − all causes 1.00 0.97 Death after recurrence 0.91 0.90 Death without recurrence 1.12 1.05 0.2 0.4 0.6 0.8 1.0 1.2 1.5 2.0 Hazard ratio (A / T) and 95% CI NABON / BOOG 2008
 HR+ patients. Favours anastrozole (A) Favours tamoxifen (T) Hazard ratio. Hazard ratio. All patients. HR+ patients. Disease-free survival Time to recurrence Time to distant recurrence Contralateral breast cancer The ATAC trial demonstrated that anastrozole was consistently superior to tamoxifen for all efficacy endpoints except overall survival, death after recurrence and death without recurrence where no significant change was observed. Anastrozole has proven superiority over tamoxifen, in terms of significant reduction in all forms of recurrence, ensuring that women can live cancer-free for longer. Overall survival, after a median follow-up of 100 months, is similar for both anastrozole and tamoxifen. Anastrozole reduces the risk of death following recurrence by 10% Although currently not statistically significant (p=0.2), there is a 90% chance that time to death following recurrence is longer with anastrozole. Deaths without recurrence were slightly but not significantly higher in the anastrozole group but no specific cause of death was elevated; most likely this is due to play of chance. There was no evidence of increased cardiovascular mortality or morbidity. This makes it difficult to show a benefit when patients are dying from other causes by virtue of their old age (mean age 72 years) Death − all causes Death after recurrence Death without recurrence Hazard ratio (A / T) and 95% CI. NABON / BOOG")
10
Time to recurrence HR+ patients
30 30 HR 0.76 95% CI (0.67, 0.87) p-value 0.0001 25 HR+ 25 21.8% 20 20 Tamoxifen (T) Anastrozole (A) 15 15 12.5% 17.0% 10 10 9.7% 5 5 Recurrence rates continued to be lower with anastrozole after treatment completion In the HR+ subgroup, the absolute difference in recurrence increased from 2.8% at 5 years to 4.8% at 9 years in favour of anastrozole. Tamoxifen has a known carryover effect in years 5-9, of about two-thirds the size of that during active treatment. There is a statistically significant larger carryover effect for anastrozole (HR=0.75, 95% CI , p=0.01). Absolute difference 2.8% 4.8% 1 2 3 4 5 6 7 8 9 Follow-up time (years) At risk: A T NABON / BOOG 2008 10
 p-value HR % Tamoxifen (T) Anastrozole (A) % 17.0% % Recurrence rates continued to be lower with anastrozole after treatment completion. In the HR+ subgroup, the absolute difference in recurrence increased from 2.8% at 5 years to 4.8% at 9 years in favour of anastrozole. Tamoxifen has a known carryover effect in years 5-9, of about two-thirds the size of that during active treatment. There is a statistically significant larger carryover effect for anastrozole (HR=0.75, 95% CI , p=0.01). Absolute difference. 2.8% 4.8% Follow-up time (years) At risk: A T. NABON / BOOG")
11
TTR: Carry-over effect in periode na behandeling
Aantal recidieven blijft lager na stop behandeling met anastrozol Tamoxifen heeft bekend carry-over effect in jaar 5-9 van ~ 2/3 de grootte tijdens actieve behandeling Statistisch significant groter carry-over effect voor anastrozol (HR=0.75, 95% CI , p=0.01) Ernstige bijwerkingen tijdens en na behandeling Anastrozol v tamoxifen: Fractuur episoden (%) - Tijdens 2.93 v 1.90* - Na 1.56 v 1.51 Absolute difference in recurrence in the HR+ population in ATAC at 9 years is 4.8% in favour of anastrozole The larger carryover effect seen with anastrozole compared with tamoxifen means that starting with anastrozole has a highly significant impact in the long term References Early Breast Cancer Trialists' Collaborative Group. Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomised trials. Lancet 2005;365: TTR, time to recurrence 1EBCTCG overview. Lancet 2005; 365: NABON / BOOG 2008
 Ernstige bijwerkingen tijdens en na behandeling. Anastrozol v tamoxifen: Fractuur episoden (%) - Tijdens 2.93 v 1.90* - Na 1.56 v Absolute difference in recurrence in the HR+ population in ATAC at 9 years is 4.8% in favour of anastrozole. The larger carryover effect seen with anastrozole compared with tamoxifen means that starting with anastrozole has a highly significant impact in the long term. References. Early Breast Cancer Trialists Collaborative Group. Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomised trials. Lancet 2005;365: TTR, time to recurrence. 1EBCTCG overview. Lancet 2005; 365: NABON / BOOG")
12
Conclusie effectiviteit
100 maanden mediane follow-up: Anastrozole v tamoxifen ↓ recidief: Locoregionaal Contralateraal Op afstand ↑ verschil TTR na behandeling: HR+ : 2.8% na 5 jaar → 4.8% na 9 jaar HR ANA v TAM (5-9 j) = 0.75 (p=0.01) Anastrozole is the only aromatase inhibitor that significantly reduces all forms of breast cancer recurrence: distant, locoregional, contralateral. NABON / BOOG 2008
 = 0.75 (p=0.01) Anastrozole is the only aromatase inhibitor that significantly reduces all forms of breast cancer recurrence: distant, locoregional, contralateral. NABON / BOOG")
13
Conclusie veiligheid Tijdens behandeling: Risico op fractuur
Na 5 jaar behandeling met Anastrozol: Geen overmaat fractuurrisico Geen nieuwe morbiditeit of mortaliteit NABON / BOOG 2008

14
HST: oestrogeen + progesteron
Kruisende lijnen: ↑ BC-risico Cheblowsky NABON / BOOG 2008

15
HST: oestrogenen ↓ BC-risico (of =) NABON / BOOG 2008
 NABON / BOOG 2008")
16
HST-gebruik ↓↓ in midden Ravdin NABON / BOOG 2008

17
HST-gebruik ↓ in midden 2002 NABON / BOOG 2008

18
BC-incidentie ↓ in US = in NL NABON / BOOG 2008

21
COBRA Tamoxifen Trial Vraagstelling
297 BC-patiënten Genotype bepaald CYP2D6 score bepaald o.b.v. allelactiviteit (0 - 2) Vraagstelling Hebben vrouwen die ‘poor metabolizers’ (PMs) van CYP2D6 zijn minder voordeel van tamoxifen t.g.v. lage endoxifenspiegels? En minder bijwerkingen? Stoppen daardoor minder vaak met tamoxifen? NABON / BOOG 2008
 Vraagstelling. Hebben vrouwen die ‘poor metabolizers’ (PMs) van CYP2D6 zijn minder voordeel van tamoxifen t.g.v. lage endoxifenspiegels En minder bijwerkingen Stoppen daardoor minder vaak met tamoxifen NABON / BOOG")
22
Conclusies Implicaties
CYP2D6-score 0 (PMs): geen uitvallers CYP2D6-activiteit: ↑ kans op uitvallers t.g.v. bijw. CYP2D6-score ↑: ↑ aantal uitvallers Implicaties Meeste kans op voordeel TAM = Meeste kans op vroegtijdig stoppen Vroege interventies om bijw. ↓ NABON / BOOG 2008
: geen uitvallers. CYP2D6-activiteit: ↑ kans op uitvallers t.g.v. bijw. CYP2D6-score ↑: ↑ aantal uitvallers. Implicaties. Meeste kans op voordeel TAM = Meeste kans op vroegtijdig stoppen. Vroege interventies om bijw. ↓ NABON / BOOG")
23
HER-paden Geïntegreerde netwerken: weerstaan enkelvoudige verstoringen
Yarden Geïntegreerde netwerken: weerstaan enkelvoudige verstoringen NABON / BOOG 2008

24
HER receptoren Osborn NABON / BOOG 2008

25
Trastuzumab Blokkeert 2-2 NABON / BOOG 2008

26
Trastuzumab beyond progression: fase III studie, 1e-2e lijn M1
156 patiënten HER2+ na taxaan/trastuzumab interim-analyse 21-dagen cyclus: Capecitabine mg/m2/d D1-14 Trastuzumab 6 mg/kg D1 RANDOMI ZE Capecitabine + Trastuzumab Capecitabine von Minckwitz. SABCS 2007 NABON / BOOG 2008

27
Prim. eindpunt. Sec. eindpunt PFS. OS. 5. 6 v 8. 5 mnd. 19. 9 v 20
Prim. eindpunt Sec. eindpunt PFS OS v 8.5 mnd v 20.3 mnd HR = HR = med. FU 11.8 mnd (planned 18 mnd) RR 24.6 v 48.9% NABON / BOOG 2008
 RR 24.6 v 48.9% NABON / BOOG")
28
Lapatinib Blokkeert 1-1, 1-2, 1-3, 2-3 NABON / BOOG 2008

29
Lapatinib + Capecitabine bij hersenmeta’s fase II studie, 2e lijn M1
patiënten HER2+ Na trastuzumab 21-dagen cyclus: Capecitabine mg/m2/d D1-14 Lapatinib mg cont. Mediane PFS 16 weken (95%CI = 11, 19 weken) Lin, SABCS 2007 NABON / BOOG 2008
 Lin, SABCS NABON / BOOG")
30
Pertuzumab ↓ HER2 homo- en heterodimerisatie, ↓ HER signalering, blokkeert 1-2, 2-3 NABON / BOOG 2008

31
Pertuzumab plus trastuzumab
(Cardiale) veiligheid na progressie op trastuzumab NABON / BOOG 2008
 veiligheid na progressie op trastuzumab. NABON / BOOG")
32
Veiligheid Effectiviteit
n = 61 Graad 3 toxiciteit: diarree (1x) LVEF: gem. verandering 1.1% Effectiviteit n = 33 Overall response rate = 18,2 % Clinical benefit rate = 39,4 % NABON / BOOG 2008
 LVEF: gem. verandering 1.1% Effectiviteit. n = 33. Overall response rate = 18,2 % Clinical benefit rate = 39,4 % NABON / BOOG")
33
Conclusies targeted therapie
Signalerend HER-pad is een complex, robuust en zich aanpassend netwerk Remming van dit netwerk is zeer effectief bij HER2+ De novo en verworven resistentie vindt plaats via vele mechanismen M.n. incomplete blokkade van de receptorlaag Gecombineerde receptor inhibitoren verdienen klinische evaluatie Voorspelling van resistentiemechanisme van prim. tumor is van wezenlijk belang NABON / BOOG 2008

34
Discussie ATLAS Groter carry-over effect 10 v 5 jaar TAM
> 5 jaar adjuvante hormonale therapie: impact op uitkomsten voor minstens 14 jaar Moet verlengde adjuvante hormonale therapie als standaard behandeling overwogen worden bij HR+ vroege borstkanker? Voorlopige resultaten BOOG-NABON 2008

35
Discussie ATAC Groter carry-over effect ANA v TAM
Begin behandeling met anastrozol: impact op uitkomsten voor minstens 9 jaar Moet anastrozol als initiële adjuvante therapie als standaard behandeling overwogen worden bij postmenopausale vrouwen met HR+ vroege borstkanker? Publication: The Lancet Oncology, Jan 08 BOOG-NABON 2008

36
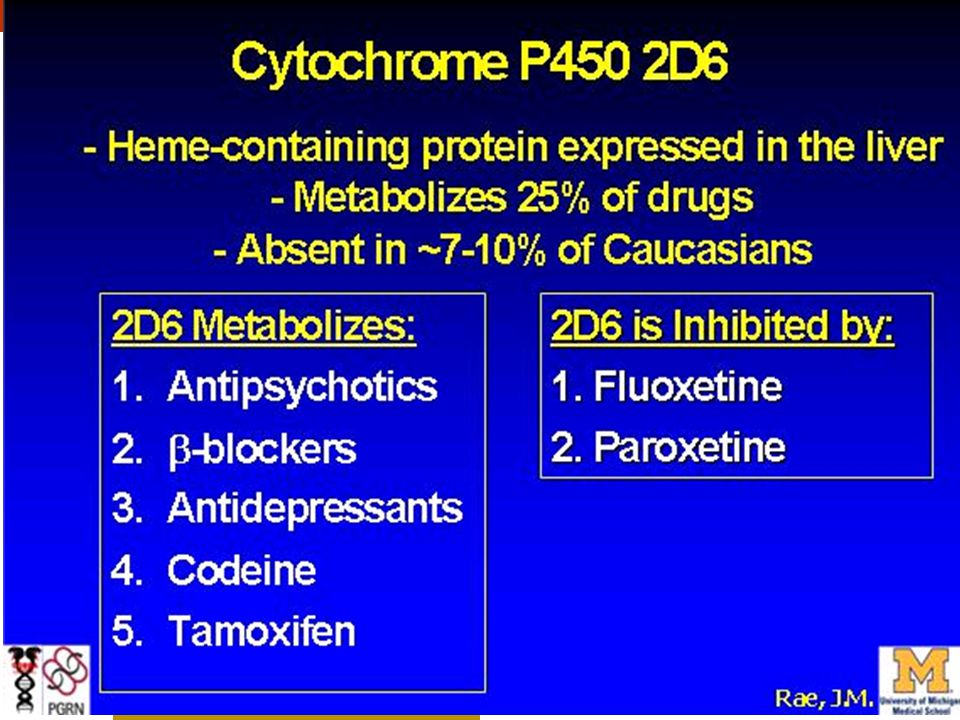
Discussie Cytochroom P450 2D6 activiteit
CYP2D6-activiteit ~: 8% Poor Metabolizers ↑ CYP2D6-activiteit: ↑ kans op bijw. ↑ kans op stop tamoxifen v ↑ kans op voordeel tamoxifen Rekening houden met CYP2D6-activiteit bij tamoxifen? Bijwerkingen? 2D6 inhibitie door fluoxetine, paroxetine Dosering? BOOG-NABON 2008

37
Discussie targeted therapie
Trastuzumab: - Adjuvante strategie: 1 jaar - Palliatieve strategie: treatment beyond progression? Bevacizumab Lapatinib: - Palliatieve strategie: na trastuzumab? bij hersenmeta’s? Pertuzumab: - Nog geen indicatie BOOG-NABON 2008

Verwante presentaties

 DoelgroepVerzondenOntvangen% LG wonen en dagbesteding.>")

















