Download de presentatie
De presentatie wordt gedownload. Even geduld aub

1
CARTS studie Ideeën voor een vervolgstudie?
Prof Dr Hans de Wilt Department of Surgery Division of Surgical Oncology and GI Surgery St Radboud UMC Nijmegen

2
Disclosure belangen spreker
(potentiële) belangenverstrengeling Geen / Zie hieronder Voor bijeenkomst mogelijk relevante relaties met bedrijven Bedrijfsnamen Sponsoring of onderzoeksgeld Honorarium of andere (financiële) vergoeding Aandeelhouder Andere relatie, namelijk … Roche (restricted grant CARTS) Sprekersvergoeding
 belangenverstrengeling. Geen / Zie hieronder Voor bijeenkomst mogelijk relevante relaties met bedrijven. Bedrijfsnamen. Sponsoring of onderzoeksgeld. Honorarium of andere (financiële) vergoeding. Aandeelhouder. Andere relatie, namelijk … Roche (restricted grant CARTS) Sprekersvergoeding. ")
3
Chirurgie voor het colorectaal carcinoom na de gereviseerde richtlijn
Richtlijnen Nieuwe studies

4
Rectum carcinoom: voor 2014
Very early rectal cancers (≤ T1): TEM
: TEM.")
5
Rectum carcinoom: voor 2014
Very early rectal cancers (≤ T1): TEM Early rectal cancers: 5x5Gy + TME
: TEM. Early rectal cancers: 5x5Gy + TME.")
6
Rectum carcinoom: voor 2014
Very early rectal cancers (≤ T1): TEM Early rectal cancers: TME only Advanced rectal cancers: Chemoradiation and (Beyond) TME
: TEM. Early rectal cancers: TME only. Advanced rectal cancers: Chemoradiation and (Beyond) TME.")
7
Rectumsparende behandeling (Richtlijnen 2014)
Bij een klinisch beoordeeld laag risico T1 rectumcarcinoom: Diameter kleiner dan 3-4 cm, Goed tot matig gedifferentieerd Geen lymfangioinvasie Lokale excisie zonder neo-adjuvante therapie overwegen Alleen na volledige stadiëring in een multidisciplinair oncologisch overleg, minder bewijs voor lange termijn oncologische veiligheid. Door middel van een endoscopische techniek Transanale endoscopische microchirurgie (TEM) Single port transanale endoscopische chirurgie (SPTS) Nauwkeurig gestandaardiseerd pathologisch onderzoek
 Single port transanale endoscopische chirurgie (SPTS) Nauwkeurig gestandaardiseerd pathologisch onderzoek.")
8
Rectum carcinoom: 2014 en erna
Very early rectal cancers (≤ T1): TEM Rectum carcinoom: 2014 en erna
: TEM. Rectum carcinoom: 2014 en erna.")
9
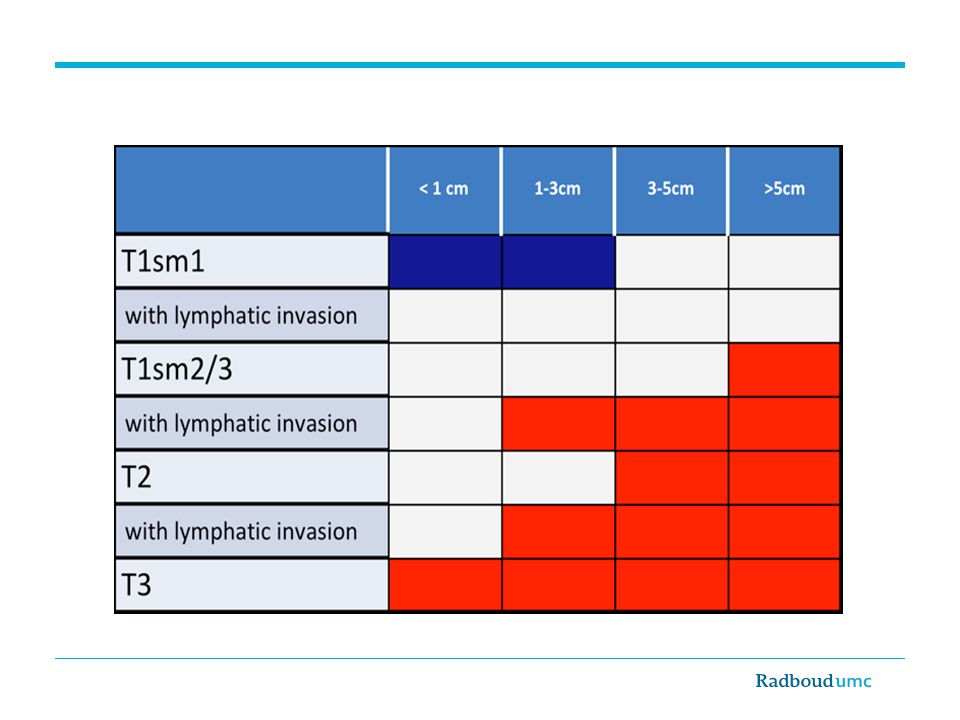
Rectumsparende behandeling (Concept richtlijnen) Na lokale excisie van een rectumafwijking een invasief carcinoom: Hoog risico T1 Slecht gedifferentieerd Lymfangioinvasie Tumorvrije marge <1 mm / inconclusieve ≥T2 stadium Aanvullende radicale chirurgie Bij twijfel over de uiteindelijke radicaliteit preoperatieve radiotherapie
 Na lokale excisie van een rectumafwijking een invasief carcinoom: Hoog risico T1 Slecht gedifferentieerd Lymfangioinvasie Tumorvrije marge <1 mm / inconclusieve ≥T2 stadium Aanvullende radicale chirurgie Bij twijfel over de uiteindelijke radicaliteit preoperatieve radiotherapie")
10
Rectal preserving therapy for early rectal cancer
TESAR trial Rectal preserving therapy for early rectal cancer Jurriaan Tuynman, MD, PhD Pieter Tanis, MD, PhD Wernard Borstlap, MD

13
Locale excisie voor T2,3 rectum carcinoom
Hoger T stadium = hoger lokaal recidief (30-40%) Niet acceptabel als standaard behandeling Hoogbejaarde/ernstige co-morbiditeit een alternatief
 Niet acceptabel als standaard behandeling. Hoogbejaarde/ernstige co-morbiditeit een alternatief.")
14
Rectum carcinoom Total Mesorectal Excision: Gouden standaard
‘Early rectal cancer’ (T1/3N0): Lokaal recidief laag Overleving excellent Radiotherapie onnodig, morbiditeit 14
: Lokaal recidief laag. Overleving excellent. Radiotherapie onnodig, morbiditeit. 14.")
15
Early distal rectal cancer
Total Mesorectal Excision: Mortaliteit (2.5% Dutch Audit 2013) Morbiditeit (lekkage) Defaecatie stoornissen Colostoma, colo-anale anastomose Urogenitale/sexuele dysfunctie Alternatief? 15
 Morbiditeit (lekkage) Defaecatie stoornissen. Colostoma, colo-anale anastomose. Urogenitale/sexuele dysfunctie. Alternatief 15.")
16
Dedicated radiologists in a center of excellence
Pre-selected group of patients with a clinical complete response J Clin Oncol 2011

17
Complete Respons Pathologische CR na CRtx voor locally advanced tumoren 16% (1) Hoe bepaal je een cCR: RT Rectoscopie ERUS CT/MRI PET Wanneer te bepalen? (6, 8, 10, 12 weken ?) cCR = pCR? 1) Maas et al., Lancet Oncol 2011, Martin et al., Br J Surg 2012 17
 cCR = pCR 1) Maas et al., Lancet Oncol 2011, Martin et al., Br J Surg")
18
Rectumsparende behandeling (concept richtlijnen)
Na (chemo)radiotherapie bij complete klinische respons dient buiten studieverband geen ‘wait and see’ beleid te worden toegepast. Follow-up na lokale excisie van een rectumcarcinoom: 2 tot 3 jaar endoscopische inspectie van het litteken MRI bekken met intervallen van 3 tot 6 maanden Afstandsmetastasen follow-up en surveillance coloscopie Eventuele endorectale echografie na lokale excisie kan op basis van de beschikbare literatuur niet worden gedaan. >>> REGISTRATIE STUDIE Beets, vd Velde
radiotherapie bij complete klinische respons dient buiten studieverband geen ‘wait and see’ beleid te worden toegepast. Follow-up na lokale excisie van een rectumcarcinoom: 2 tot 3 jaar endoscopische inspectie van het litteken. MRI bekken met intervallen van 3 tot 6 maanden. Afstandsmetastasen follow-up en surveillance coloscopie. Eventuele endorectale echografie na lokale excisie kan op basis van de beschikbare literatuur niet worden gedaan. >>> REGISTRATIE STUDIE. Beets, vd Velde.")
19
BMC Surgery 2011

20
Phase II study in the Netherlands
55 pts with distal cT1-3N0M0 rectal cancer Tattoo, clips, etc. of original tumorbed Prim endpoint ≥ 30 % ypT0-1 R0 after TEM Sec endpoints Local recurrence rate & QOL Toxicity & morbidity BMC Surgery 2011

21
CARTS 55 patients Chemoradiation (25x2 Gy + Xeloda) In preparation
 In preparation")
22
Chemoradiation 4 patients stopped chemoradiation treatment
1 died of E-coli sepsis, day 24 (74yr male) 1 died of gastrointestinal toxicity, day 36 (53 yr male) 1 severe vomiting and diarrhoea, day 27 (59yr female) 1 pain and radiation proctitis, day 30 (60yr female) 47 of 51 (90%) standard protocol chemoradiation 4 chemotherapy dose reduction In preparation
 1 died of gastrointestinal toxicity, day 36 (53 yr male) 1 severe vomiting and diarrhoea, day 27 (59yr female) 1 pain and radiation proctitis, day 30 (60yr female) 47 of 51 (90%) standard protocol chemoradiation. 4 chemotherapy dose reduction. In preparation.")
23
CARTS 55 patients Chemoradiation (25x2 Gy + Xeloda)
52 response evaluation 3 stopped CRtx: (2 deaths) 1 refused surgery CARTS In preparation
 1 refused surgery. CARTS. In preparation.")
24
Clinical response (Scopy, Endo ultrasound, MRI)
4 pts with minor/no clinical response: TME surgery 2 ypT1N0 (overstaged) 2 ypT2N1 47 pts with successfull clinical response: TEM treatment 21 ypT0N0 9 ypT1N0 15 ypT2N0 (understaged) 1 ypT3N0 1 ypT0N1 In preparation
 2 ypT2N1. 47 pts with successfull clinical response: TEM treatment. 21 ypT0N0. 9 ypT1N0. 15 ypT2N0 (understaged) 1 ypT3N0. 1 ypT0N1. In preparation.")
25
CARTS 55 patients Chemoradiation (25x2 Gy + Xeloda) 3 stopped CRtx:
52 Surgery 47 TEM 21 ypT0 9 ypT1 17 ≥ ypT2 4 TME 3 stopped CRtx: (2 deaths) 1 refused surgery CARTS In preparation
 1 refused surgery. CARTS. In preparation.")
26
Clinical results Total number of patients organ saving:
30/55 TEM ypT0-1N0 (55%) 9/55 TEM ypT2N0 (16%) 1/55 no surgery (2%) 40/55 patients (73%) In preparation
 9/55 TEM ypT2N0 (16%) 1/55 no surgery (2%) 40/55 patients (73%) In preparation.")
27
CARTS Secondary endpoints
Recurrence 4 pts (median follow-up 17 months) ypT1Nx (9 months) ypT2Nx (8 months) ypT2Nx (7 months) ypT2Nx (10 months) In preparation
 ypT1Nx (9 months) ypT2Nx (8 months) ypT2Nx (7 months) ypT2Nx (10 months) In preparation.")
28
Early distal rectal cancer
Chemoradiatie + TEM de gouden standaard? 55-60% succesvol 40% overbehandeling (Chemoradiatie was niet nodig) 3x recidief bij ypT2 Toxiciteit Lange termijn ?? Randomiseren versus standaard chirurgie
 3x recidief bij ypT2. Toxiciteit. Lange termijn Randomiseren versus standaard chirurgie.")
29
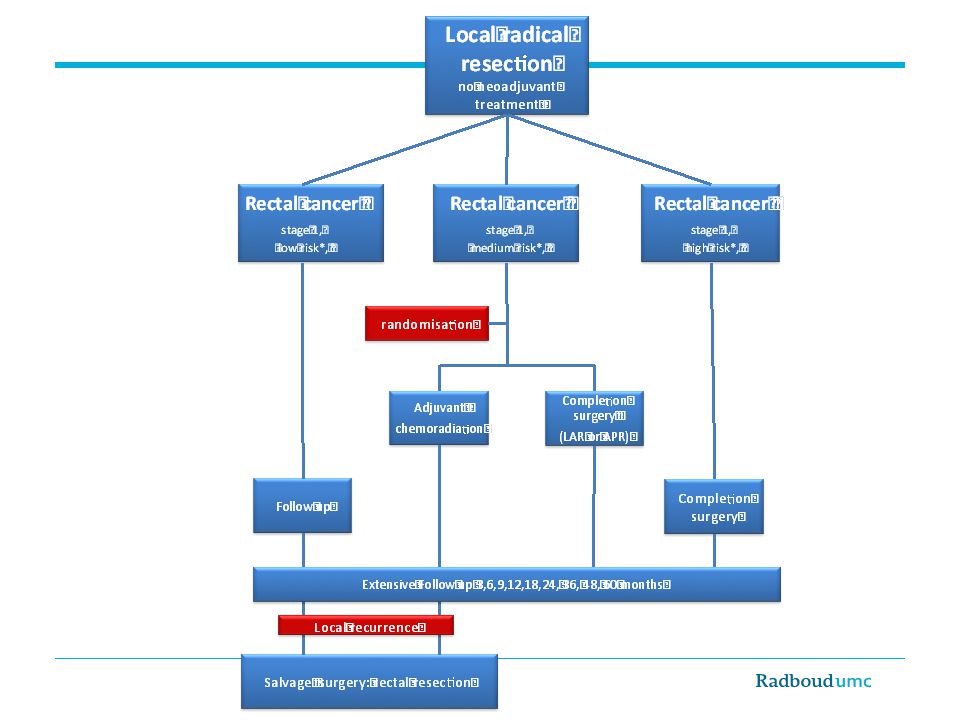
Rectumsparende behandeling (concept richtlijnen)
Neo-adjuvante (chemo)radiotherapie gevolgd door lokale excisie, bij: Hoog risico T1N0 (slecht gedifferentieerd, lymfangioinvasie) T2-3N0 rectumcarcinoom Alleen indien standaard behandeling door patiënt niet wordt verdragen (leeftijd, comorbiditeit) of wordt geweigerd, of in studieverband. ypT0-1 stadium: Follow-up. ypT2-3 stadium: Radicale chirurgie (interval van 6-8 weken).
radiotherapie gevolgd door lokale excisie, bij: Hoog risico T1N0 (slecht gedifferentieerd, lymfangioinvasie) T2-3N0 rectumcarcinoom. Alleen indien standaard behandeling door patiënt niet wordt verdragen (leeftijd, comorbiditeit) of wordt geweigerd, of in studieverband. ypT0-1 stadium: Follow-up. ypT2-3 stadium: Radicale chirurgie (interval van 6-8 weken).")
30
TRECARTS UK - the Netherlands collaboration
Randomized phase II/III study cT2/3N0 (<10mm nodes, if 5-10: no malignant signs) Tumors <6 cm of ano-rectal verge Treatment: Chemoradiation or 5x5 Gy (1 week) vs standard surgery
 Tumors <6 cm of ano-rectal verge. Treatment: Chemoradiation or 5x5 Gy (1 week) vs standard surgery.")
31
TRECARTS Obvious tumor: TME (APR, LAR) Partial response: TEM
(near) complete response: Follow-up Primary endpoint (phase II): Randomisation possible Secondary endpoint (phase III): QOL, recurrence, survival
 complete response: Follow-up. Primary endpoint (phase II): Randomisation possible. Secondary endpoint (phase III): QOL, recurrence, survival.")
32
cT1-3N0 distal rectal cancer
TRECARTS cT1-3N0 distal rectal cancer Randomisation 5x5Gy Watchfull waiting TEM TME 25x2G+ Xeloda Standard TME surgery In preparation

33
Rectum carcinoom: 2014 en erna
Very early rectal cancers (≤ T1): TEM Hoog risico T1 na poliepectomie/TEM: TESAR Hoog-mid T2,3N0: TME Laag T2,3N0: TRECART N1 rectumcarcinoom *: 5x5 en TME Bedreigde MRF *: Chemoradiation and (Beyond) TME Rapido *) ALTIJD herevaluatie na 6-8 weken met MRI, RT, scopie Indien (near) complete response: Registratie studie Rectum carcinoom: 2014 en erna
: TEM. Hoog risico T1 na poliepectomie/TEM: TESAR. Hoog-mid T2,3N0: TME. Laag T2,3N0: TRECART. N1 rectumcarcinoom *: 5x5 en TME. Bedreigde MRF *: Chemoradiation and (Beyond) TME. Rapido. *) ALTIJD herevaluatie na 6-8 weken met MRI, RT, scopie. Indien (near) complete response: Registratie studie. Rectum carcinoom: 2014 en erna.")
34
RECTUMCARCINOOM 2014 en erna
Direct opereren Geen plaats voor 5x5Gy en direct TME Altijd rectumsparende optie overwegen: TEM, (chemo)radiotherapie lang wachten (minimaal 10 weken) Watchfull waiting, TEM when in doubt, salvage TME TRIALS, TRIALS, TRIALS
radiotherapie lang wachten (minimaal 10 weken) Watchfull waiting, TEM when in doubt, salvage TME. TRIALS, TRIALS, TRIALS.")
Verwante presentaties















, Andre Bergman (internist-oncoloog,>")



