Download de presentatie
De presentatie wordt gedownload. Even geduld aub

1
Neurosurgical treatment of Parkinson’s disease
Bart Nuttin Dept. of Neurosurgery

2
Surgical treatment of the parkinsonian patient
Lesion : Vim, GPi Electrical stimulation Transplant : experimental Gene therapy : future

3
Components implanted The Activa® System comprises the lead, extension and neurostimulator, all of which are fully implantable. The neurostimulator is a pacemaker-like device that is the power source for the system. It is about 7.5 cm (3 inches) wide and 1.3 cm (0.5 inches) thick and contains a small battery and computer chip programmed to send electrical pulses to control symptoms of movement disorders. The extension is an insulated wire placed under the scalp and outside the skull that connects to the lead and runs behind the ear, down the neck, and into the chest below the collarbone where it connects to the neurostimulator. Occasionally the neurostimulator will be placed under the skin on the lower abdominal wall. The lead is an insulated wire terminating in four electrodes. The Medtronic® Model 3387 and 3389 DBSTM Leads are designed to electrically stimulate specific areas of the brain (deep brain stimulation). The Model 3387 DBS lead features wide (1.5 mm) spacing between each of the four electrodes at the distal end. The Model 3389 DBS lead features narrow (0.5 mm) spacing between each of the four electrodes at the distal end.
 wide and 1.3 cm (0.5 inches) thick and contains a small battery and computer chip programmed to send electrical pulses to control symptoms of movement disorders. The extension is an insulated wire placed under the scalp and outside the skull that connects to the lead and runs behind the ear, down the neck, and into the chest below the collarbone where it connects to the neurostimulator. Occasionally the neurostimulator will be placed under the skin on the lower abdominal wall. The lead is an insulated wire terminating in four electrodes. The Medtronic® Model 3387 and 3389 DBSTM Leads are designed to electrically stimulate specific areas of the brain (deep brain stimulation). The Model 3387 DBS lead features wide (1.5 mm) spacing between each of the four electrodes at the distal end. The Model 3389 DBS lead features narrow (0.5 mm) spacing between each of the four electrodes at the distal end.")
4
(+) (+) (-) (-) Monopolar Bipolar
Stimulation mode can be adjusted to reach different regions of tissue (+) (+) (-) (-) Selection of monopolar (unipolar) or bipolar modes enables the stimulation of different regions in the tissue surrounding the electrodes. The negative electrode exerts the therapeutic effect. In monopolar mode, one or more of the four electrodes of the lead serves as the negative pole (cathode) and the neurostimulator case functions as the positive pole (anode), producing a spherical field. Typically, one electrode is activated. In bipolar mode, adjacent electrodes on the lead have opposing polarity. One or more electrodes of the DBS lead serves as the positive pole (anode), and one or more of the remaining electrodes functions as the negative pole (cathode). The typical bipolar setting consists of one positive and one negative electrode. This generates a more focused field with a higher current intensity, compared with the monopolar mode. Focusing the field in this way may help to maximise the therapeutic effect and reduce side effects. Monopolar Bipolar
 (+) (-) (-) Selection of monopolar (unipolar) or bipolar modes enables the stimulation of different regions in the tissue surrounding the electrodes. The negative electrode exerts the therapeutic effect. In monopolar mode, one or more of the four electrodes of the lead serves as the negative pole (cathode) and the neurostimulator case functions as the positive pole (anode), producing a spherical field. Typically, one electrode is activated. In bipolar mode, adjacent electrodes on the lead have opposing polarity. One or more electrodes of the DBS lead serves as the positive pole (anode), and one or more of the remaining electrodes functions as the negative pole (cathode). The typical bipolar setting consists of one positive and one negative electrode. This generates a more focused field with a higher current intensity, compared with the monopolar mode. Focusing the field in this way may help to maximise the therapeutic effect and reduce side effects. Monopolar. Bipolar.")
5
Pulse width (µsec) duration of each stimulus
Therapeutic effect is optimised by adjusting stimulation parameters for both leads Pulse width (µsec) duration of each stimulus Amplitude (Volts) intensity of stimulation All aspects of the electrical field can be adjusted to maximise the therapeutic effect of Activa® Therapy. The polarity of each electrode can be altered (negative, positive or off) , the neurostimulator can be changed to positive or off, and the amplitude, pulse width and rate of the electrical pulses can be adjusted for both leads. Amplitude is the intensity of the stimulation, measured in volts (V). Pulse width is the duration of each pulse, measured in microseconds (µs). Rate (frequency) is the number of pulses delivered each second, measured in Herz (Hz) or pulses per second (pps). The KinetraTM neurostimulator has two available programs: one for the left side and one for the right side. Amplitude and pulse width can be independently adjusted for both programs. Rate cannot be independently adjusted, i.e. one setting determines the rate for both programs. Rate (Hertz) number of pulses per second
 duration of each stimulus. Amplitude. (Volts) intensity of stimulation. All aspects of the electrical field can be adjusted to maximise the therapeutic effect of Activa® Therapy. The polarity of each electrode can be altered (negative, positive or off) , the neurostimulator can be changed to positive or off, and the amplitude, pulse width and rate of the electrical pulses can be adjusted for both leads. Amplitude is the intensity of the stimulation, measured in volts (V). Pulse width is the duration of each pulse, measured in microseconds (µs). Rate (frequency) is the number of pulses delivered each second, measured in Herz (Hz) or pulses per second (pps). The KinetraTM neurostimulator has two available programs: one for the left side and one for the right side. Amplitude and pulse width can be independently adjusted for both programs. Rate cannot be independently adjusted, i.e. one setting determines the rate for both programs. Rate (Hertz) number of pulses per second.")
6
…

7
Bakay R. and Starr P., Pallidal surgery for the treatment of PD and movement disorders, 1998, Krauss, Grossman and Jankovic

8
Bakay R. and Starr P., Pallidal surgery for the treatment of PD and movement disorders, 1998, Krauss, Grossman and Jankovic

9
Bakay R. and Starr P., Pallidal surgery for the treatment of PD and movement disorders, 1998, Krauss, Grossman and Jankovic

10
Before After

11
Indicatie 1: Motorische complicaties
Ziekte van Parkinson (normale MRI, > 5 jaar ziekteduur) Combinatie van ernstige on/off fluctuaties EN dyskinesieën, niet controleerbaar met medicatie Ernstige on/off fluctuaties zonder dyskinesieën, indien hogere dopaminerge dosissen psychotische symptomen induceren Levodopa-responsiviteit, gedocumenteerd door levodopa-test Geen dementie Geen voorgeschiedenis van ernstige psychiatrische of gedragsmatige dysfunctie Goede algemene gezondheid Geen algemene chirurgische contra-indicaties Realistische verwachtingen: - Quantitatieve toename van ‘best on’ tijd - Minder dyskinesieën, maar verder geen kwalitatieve verbetering van ‘best on’ Prof. W. Vandenberghe
 Combinatie van ernstige on/off fluctuaties EN dyskinesieën, niet controleerbaar met medicatie. Ernstige on/off fluctuaties zonder dyskinesieën, indien hogere dopaminerge dosissen psychotische symptomen induceren. Levodopa-responsiviteit, gedocumenteerd door levodopa-test. Geen dementie. Geen voorgeschiedenis van ernstige psychiatrische of gedragsmatige dysfunctie. Goede algemene gezondheid. Geen algemene chirurgische contra-indicaties. Realistische verwachtingen: - Quantitatieve toename van ‘best on’ tijd. - Minder dyskinesieën, maar verder geen kwalitatieve verbetering van ‘best on’ Prof. W. Vandenberghe.")
12
Indicatie 2: Levodopa-resistente tremor
PD tremor is soms medicatieresistent en invaliderend Uitgesproken verbetering van medicatieresistente PD tremor door DBS (uitzondering op de regel van levodopa-responsiviteit) Geen dementie Geen voorgeschiedenis van ernstige psychiatrische of gedragsmatige dysfunctie Goede algemene gezondheid Geen algemene chirurgische contra-indicaties Realistische verwachtingen Prof. W. Vandenberghe
 Geen dementie. Geen voorgeschiedenis van ernstige psychiatrische of gedragsmatige dysfunctie. Goede algemene gezondheid. Geen algemene chirurgische contra-indicaties. Realistische verwachtingen. Prof. W. Vandenberghe.")
14
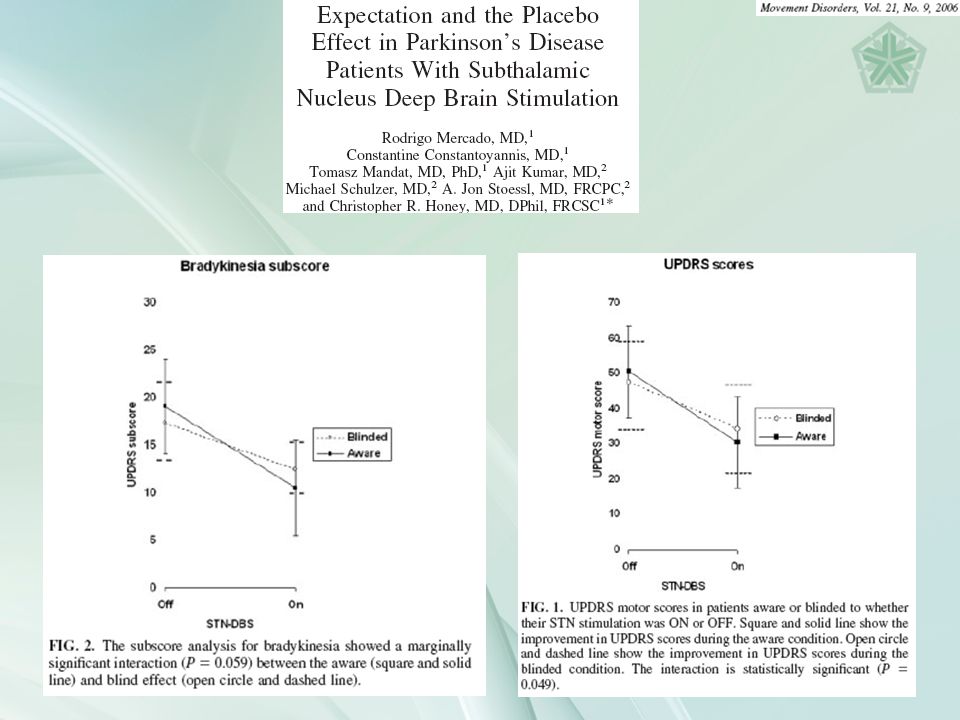
UPDRS = Unified Parkinson’s Disease Rating Scale
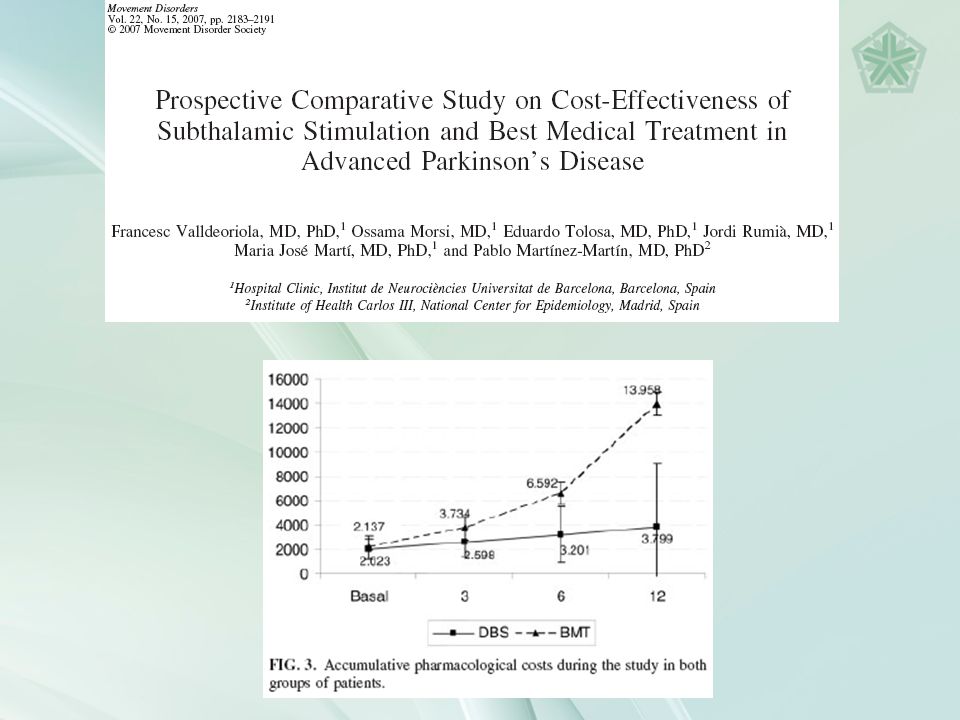
AIMS = Abnormal Involutary Movement Scale BMT = Best Medical Treatment

22
Conclusions Evidence-based medicine :
DBS is worthwhile in patients suffering from severe Parkinson’s disease, and who meet the inclusion criteria The advantages outweigh the possible risks and disadvantages It is cost-effective

Verwante presentaties