Download de presentatie
De presentatie wordt gedownload. Even geduld aub

1
Diuretica Robert Rutsaert

2
Indicaties -hypertensie -hartfalen, longoedeem
-oedeem (chronische nierinsufficiëntie, nefrotisch syndroom, levercirrose) -idiopatisch cyclisch oedeem -urolithiase (renale hypercalciurie) -(Menière, hoogteziekte, glaucoom)
 -idiopatisch cyclisch oedeem. -urolithiase (renale hypercalciurie) -(Menière, hoogteziekte, glaucoom)")
4
Nevenwerkingen -hypokaliëmie -hypomagnesemie -(orthostatische) hypotensie -hyperuricemie, jicht -diabetes mellitus (~K+) -hyperlipidemie -impotentie -hyponatremie -pancreatitis -allergische reacties: interstitiële nefritis, hematologische afwijkingen, huidreacties, -doofheid -(cholecystitis?) -(lithiumintoxicatie)
 hypotensie -hyperuricemie, jicht -diabetes mellitus (~K+) -hyperlipidemie -impotentie -hyponatremie -pancreatitis -allergische reacties: interstitiële nefritis, hematologische afwijkingen, huidreacties, -doofheid -(cholecystitis ) -(lithiumintoxicatie)")
5
Nevenwerkingen Kaliumsparende diuretica
Spironolactone hyperkaliëmie gynecomastie, pijnlijk (20%) impotentie cyclusstoornissen maaglast Canrenoaat (Soldactone) metaboliet van spironolactone Eplerenon (Inspra) minder endocriene afwijkingen duur CYP3A4 interferenties
 impotentie. cyclusstoornissen. maaglast. Canrenoaat (Soldactone) metaboliet van spironolactone. Eplerenon (Inspra) minder endocriene afwijkingen. duur. CYP3A4 interferenties.")
6
Hypokaliëmie -kaliuretisch, kaliumverlies uit myocardcel -reduceert antihypertensief effect -> diabetes, tubulusbeschadiging, ritmestoornissen, plotse dood (ook <betablokkers) -dosisafhankelijk -onderschat door staalartefact -+hypomagnesemie -QT (< quinolones, macroliden, psychotropica, ...) ; digitalis -risico milde hypertensie vs. hypokaliëmie!
 -dosisafhankelijk -onderschat door staalartefact -+hypomagnesemie -QT (< quinolones, macroliden, psychotropica, ...) ; digitalis -risico milde hypertensie vs. hypokaliëmie!")
8
Hyperkaliëmie NI ; e-GFR <(30)-40ml/min/1,73m²
Cave: NSAID, trimethoprim (co-trimoxazol), ACE-inhibitoren, sartanen of renine-inhibitoren
, ACE-inhibitoren, sartanen of renine-inhibitoren.")
9
Hyponatremie ouderen, lage BMI thiaziden > loopdiuretica
euvolemisch (cfr. SIADH), geconcentreerde urine bij correctie hoog risico op osmotisch demyelinisatiesyndroom beter niet bij bierdrinkers, psychogene polydipsie niet opnieuw
, geconcentreerde urine. bij correctie hoog risico op osmotisch demyelinisatiesyndroom. beter niet bij bierdrinkers, psychogene polydipsie. niet opnieuw.")
10
Nevenwerkingen If a little is good more must be better

11
Hypertensie BD = CO x SVR = (HRxSV) x (SVR)
 x (SVR)")
12
Hypertensie BD = CO x SVR = (HRxSV) x (SVR) op korte termijn: SV/CO
na 6-tal weken: SVR An interesting feature of the hemodynamic effects of thiazide diuretics is that although the early reduction of BP is associated with a fall in cardiac output, this becomes converted after approximately 1 month to a fall in total peripheral resistance and a rise in cardiac output, back to pretreatment levels Shah S, Khatri I. Freis ED. Am Heart J 1978;95:

13
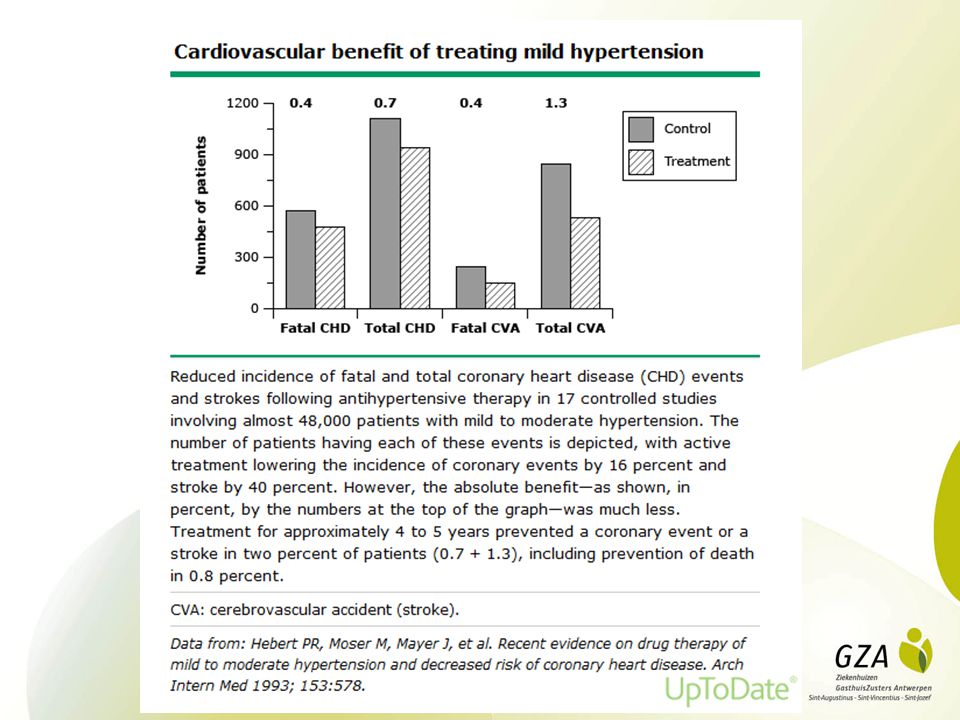
Effects of treatment on morbidity in hypertension
Effects of treatment on morbidity in hypertension. Results on patients with diastolic blood pressures averaging 115 through 129mmHg JAMA 202, , 1967

14
ALLHAT >55j, hypertensie + 1 risicofactor N = 33357
JAMA, 288, 23:2981, 2002

15
ALLHAT chlortalidone (12,5-25mg), amlodipine (2,5-10mg), lisinopril (10-40mg/d) vergelijkbaar qua CIHL, niet-fataal AMI geen hogere cardiale sterfte met amlodipine minder hartfalen en CVA met chlortalidone meer nieuw hartfalen met amlodipine > chlortalidone meer gecombineerde cardiovasculaire eindpunten met lisinopril > chlortalidone (CVA, hartfalen) chlortalidone ook beter bij diabetici JAMA, 288, 23:2981, 2002
 chlortalidone ook beter bij diabetici. JAMA, 288, 23:2981,")
16
Should we prescribe diuretics for patients with prediabetes and hypertension
ALLHAT normale basale glycemie na 4j, diabetes (nuchtere glycemie >123mg/dl): chlortalidone 11,6% amlodipine 9,8% lisinopril 8,1% (niet K-sparend) Arroll B, BMJ, 2008,337,13:1415
: chlortalidone 11,6% amlodipine 9,8% lisinopril 8,1% (niet K-sparend) Arroll B, BMJ, 2008,337,13:1415.")
17
Hypertensie NICE: cardiovasculaire eindpunten diuretica vs ACEi: minder CVA diuretica vs CEB: minder hartfalen CV outcome beter ondanks diabetes

18
Hydrochlorothiazide; dose-related blood pressure-lowering effect
Blood pressure-lowering efficacy of monotherapy with thiazide diuretics for primary hypertension Vijaya M Musini Cochrane Hypertension Group 29 MAY 2014 Hydrochlorothiazide; dose-related blood pressure-lowering effect 6.25 mg 4/2 mmHg 12.5 mg 6/3 mmHg 25 mg 8/3 mmHg 50 mg/d 11/5 mmHg for other thiazide drugs, the lowest doses studied lowered blood pressure maximally and higher doses did not lower it more greater effect on systolic than on diastolic blood pressure pulse pressure -4 to 6 mmHg > 3 mmHg pulse pressure reduction achieved by ACE inhibitors, ARBs and renin inhibitors > 2 mmHg pulse pressure reduction with non-selective beta-blockers thiazides did not increase withdrawals due to adverse effects in these short-term trials but there is a high risk of bias for that outcome.

19
Thiaziden meerdere studies outcome chlortalidone > HCTZ
bij dezelfde dosis is chlortalidone 1,5 to 2x krachtiger dan HCTZ 12,5 to 25 mg HCTZ < 12,5-25mg chlortalidone (ALLHAT) langer werkend, tragere renale excretie beschikbaarheid?
 langer werkend, tragere renale excretie. beschikbaarheid")
20
amiloride and triamterene no trials when used alone
Blood pressure lowering efficacy of potassium-sparing diuretics (that block the epithelial sodium channel) for primary hypertension Balraj S Heran Cochrane Hypertension Group 14 NOV 2012 amiloride and triamterene no trials when used alone 6 trials when added as a second drug at low doses: no blood pressure lowering effect
 for primary hypertension Balraj S Heran Cochrane Hypertension Group 14 NOV amiloride and triamterene. no trials when used alone. 6 trials when added as a second drug at low doses: no blood pressure lowering effect.")
21
thiazides as second-line drug = first-line drug
Blood pressure lowering efficacy of diuretics as second-line therapy for primary hypertension Jenny MH Chen Cochrane Hypertension Group 7 OCT 2009 thiazides as second-line drug = first-line drug BP lowering effect of thiazides is additive loop diuretics similar blood pressure lowering effect at 1 times the recommended starting dose

22
Indapamide interessante molecule vrijwel onveranderlijk hypokaliëmie
diureticum, natriuretisch, proximaal segment van de distale tubulus convolutus vasculair effect, inhibitie cardiovasculaire reactiviteit op pressor stimulus vrijwel onveranderlijk hypokaliëmie risico/baten?

23
ZOUT cave zout in geneesmiddelen
Cochrane review : "modest" reduction in salt intake on blood pressure over four weeks or more. 22 trials, hypertension (n = 999) BP -5,39/2,82 mmHg baseline median 24-hour urine sodium excretion was 162 mmol (9,5 g salt) and the mean reduction in the active arms was 75 mmol (4,4 g salt), target daily sodium intake of 87 mmol (equivalent to 2000 mg of sodium or 5 g of salt) reasonable. ZA dieet : 5-6g zout/d cave zout in geneesmiddelen
 BP -5,39/2,82 mmHg. baseline median 24-hour urine sodium excretion was 162 mmol (9,5 g salt) and the mean reduction in the active arms was 75 mmol (4,4 g salt), target daily sodium intake of 87 mmol (equivalent to 2000 mg of sodium or 5 g of salt) reasonable. ZA dieet : 5-6g zout/d. cave zout in geneesmiddelen.")
24
Therapieresistente hypertensie
dd: witte jas hypertensie, pseudohypertensie, slechte therapietrouw, secundaire hypertensie, zout Systolische bloeddruk ≥ 140 mmHg 3 antihypertensiva van verschillende klassen inclusief een diureticum In adequate dosering Toevoegen van furosemide of spironolactone

25
Blood pressure lowering efficacy of loop diuretics for primary hypertension Vijaya M Musini Cochrane Hypertension Group 15 AUG 2012 -limited number of published RCTs -effect is modest (-8/-4 mmHg) -no differences between different loop diuretics -dose ranging effects could not be evaluated -no good estimate of the incidence of harms associated with loop diuretics because of the short duration of the trials and the lack of reporting of adverse effects in many of the trials.
 -no differences between different loop diuretics -dose ranging effects could not be evaluated -no good estimate of the incidence of harms associated with loop diuretics because of the short duration of the trials and the lack of reporting of adverse effects in many of the trials.")
26
Diuretica bij hartfalen

27
Diuretics for heart failure Rajaa F Faris Cochrane Heart Group 15 FEB 2012
Chronic heart failure conventional diuretics reduce the risk of death and worsening heart failure compared to placebo (-80 deaths /1000 treated) compared to active control, diuretics appear to improve exercise capacity (+28-33%)
 compared to active control, diuretics appear to improve exercise capacity (+28-33%)")
28
Loopdiuretica krachtiger, sneller werkend, korter werkend
Schematic representation of the transport mechanisms in the thick ascending limb of the loop of Henle. The Na-K-ATPase pump in the basolateral (peritubular) membrane pumps sodium (Na) out of, and potassium (K) into, the cell. This creates a low intracellular Na concentration which drives many of the cell's reabsorptive processes. The entry of filtered sodium chloride (NaCl) into the cells is mediated by an electroneutral Na-K-2Cl (NKCC2) cotransporter in the apical (luminal) membrane. This is also called the furosemide sensitive cotransporter. The energy for this process is provided by the favorable inward electrochemical gradient for Na (the intracellular Na concentration is very low and the cell interior is electronegative). The inward movement of K and Cl occurs against their electrochemical gradients and is powered by the inward movement of Na into the cell. The reabsorbed Na which has entered the cell is pumped out by the Na-K-ATPase pump. The concentration of K in the filtrate and tubular fluid is much lower than that of Na and Cl, and much of the reabsorbed K recycle back into the lumen through K channels (ROMK) in the apical membrane to allow continued NaCl reabsorption. This movement of cationic K into the lumen plus the flux of reabsorbed Cl out of the cell into the peritubular capillary (via Cl channels) causes the lumen to become more positively charged compared with the cell and peritubular space. This lumen electropositivity creates an electrical gradient that promotes the passive reabsorption of cations—Na, calcium (Ca), and magnesium (Mg)—via the paracellular pathway between the cells. The most important Cl channels in these cells are ClC-Kb. Also present but not as critical are the ClC-Ka channels. Each of these Cl channels requires interaction with a small protein called barttin to function normally. The single Cl channel shown in the figure represents both intact ClC-Ka and ClC-Kb channels. Schematic representation of the transport mechanisms in the thick ascending limb of the loop of Henle. The Na-K-ATPase pump in the basolateral (peritubular) membrane pumps sodium (Na) out of, and potassium (K) into, the cell. This creates a low intracellular Na concentration which drives many of the cell's reabsorptive processes. The entry of filtered sodium chloride (NaCl) into the cells is mediated by an electroneutral Na-K-2Cl (NKCC2) cotransporter in the apical (luminal) membrane. This is also called the furosemide sensitive cotransporter. The energy for this process is provided by the favorable inward electrochemical gradient for Na (the intracellular Na concentration is very low and the cell interior is electronegative). The inward movement of K and Cl occurs against their electrochemical gradients and is powered by the inward movement of Na into the cell. The reabsorbed Na which has entered the cell is pumped out by the Na-K-ATPase pump. The concentration of K in the filtrate and tubular fluid is much lower than that of Na and Cl, and much of the reabsorbed K recycle back into the lumen through K channels (ROMK) in the apical membrane to allow continued NaCl reabsorption. This movement of cationic K into the lumen plus the flux of reabsorbed Cl out of the cell into the peritubular capillary (via Cl channels) causes the lumen to become more positively charged compared with the cell and peritubular space. This lumen electropositivity creates an electrical gradient that promotes the passive reabsorption of cations—Na, calcium (Ca), and magnesium (Mg)—via the paracellular pathway between the cells. The most important Cl channels in these cells are ClC-Kb. Also present but not as critical are the ClC-Ka channels. Each of these Cl channels requires interaction with a small protein called barttin to function normally. The single Cl channel shown in the figure represents both intact ClC-Ka and ClC-Kb channels. Loopdiuretica krachtiger, sneller werkend, korter werkend prolongatum (duurder) sterk eiwitgebonden, tubulaire secretie compensatoire mechanismen: RAAS, ADH
 membrane pumps sodium (Na) out of, and potassium (K) into, the cell. This creates a low intracellular Na concentration which drives many of the cell s reabsorptive processes. The entry of filtered sodium chloride (NaCl) into the cells is mediated by an electroneutral Na-K-2Cl (NKCC2) cotransporter in the apical (luminal) membrane. This is also called the furosemide sensitive cotransporter. The energy for this process is provided by the favorable inward electrochemical gradient for Na (the intracellular Na concentration is very low and the cell interior is electronegative). The inward movement of K and Cl occurs against their electrochemical gradients and is powered by the inward movement of Na into the cell. The reabsorbed Na which has entered the cell is pumped out by the Na-K-ATPase pump. The concentration of K in the filtrate and tubular fluid is much lower than that of Na and Cl, and much of the reabsorbed K recycle back into the lumen through K channels (ROMK) in the apical membrane to allow continued NaCl reabsorption. This movement of cationic K into the lumen plus the flux of reabsorbed Cl out of the cell into the peritubular capillary (via Cl channels) causes the lumen to become more positively charged compared with the cell and peritubular space. This lumen electropositivity creates an electrical gradient that promotes the passive reabsorption of cations—Na, calcium (Ca), and magnesium (Mg)—via the paracellular pathway between the cells. The most important Cl channels in these cells are ClC-Kb. Also present but not as critical are the ClC-Ka channels. Each of these Cl channels requires interaction with a small protein called barttin to function normally. The single Cl channel shown in the figure represents both intact ClC-Ka and ClC-Kb channels. Schematic representation of the transport mechanisms in the thick ascending limb of the loop of Henle. The Na-K-ATPase pump in the basolateral (peritubular) membrane pumps sodium (Na) out of, and potassium (K) into, the cell. This creates a low intracellular Na concentration which drives many of the cell s reabsorptive processes. The entry of filtered sodium chloride (NaCl) into the cells is mediated by an electroneutral Na-K-2Cl (NKCC2) cotransporter in the apical (luminal) membrane. This is also called the furosemide sensitive cotransporter. The energy for this process is provided by the favorable inward electrochemical gradient for Na (the intracellular Na concentration is very low and the cell interior is electronegative). The inward movement of K and Cl occurs against their electrochemical gradients and is powered by the inward movement of Na into the cell. The reabsorbed Na which has entered the cell is pumped out by the Na-K-ATPase pump. The concentration of K in the filtrate and tubular fluid is much lower than that of Na and Cl, and much of the reabsorbed K recycle back into the lumen through K channels (ROMK) in the apical membrane to allow continued NaCl reabsorption. This movement of cationic K into the lumen plus the flux of reabsorbed Cl out of the cell into the peritubular capillary (via Cl channels) causes the lumen to become more positively charged compared with the cell and peritubular space. This lumen electropositivity creates an electrical gradient that promotes the passive reabsorption of cations—Na, calcium (Ca), and magnesium (Mg)—via the paracellular pathway between the cells. The most important Cl channels in these cells are ClC-Kb. Also present but not as critical are the ClC-Ka channels. Each of these Cl channels requires interaction with a small protein called barttin to function normally. The single Cl channel shown in the figure represents both intact ClC-Ka and ClC-Kb channels. Loopdiuretica. krachtiger, sneller werkend, korter werkend. prolongatum (duurder) sterk eiwitgebonden, tubulaire secretie. compensatoire mechanismen: RAAS, ADH.")
29
Loopdiuretica furosemide: bioavailability 50% bumetamide: bioavailability 95%, piek na 0,5-2u; eiwitbinding 95%; t1/2 1-1,5u; tubulaire excretie minder hyponatremie dan thiaziden U Na/K > thiaziden

30
Rate of furosemide excretion vs increase in sodium excretion in normals (solid line) and patients with heart failure (HF; dashed line). Patients with HF show relative resistance at a given rate of diuretic excretion due to increased sodium reabsorption in other nephron segments. BraterDC, Kidney Int 1984; 26:183

31
Loopdiuretica normal renal function:
IV: diuresis begins with as little as 10 mg of furosemide; maximal effect with 40 mg given intravenously po: maximum dose is 80 mg since its bioavailability is only about 50 percent, although there is substantial interpatient and intrapatient variability equivalent maximal doses are 1 mg for bumetamide and 15 to 20 mg for either oral or intravenous torasemide since these agents are almost completely absorbed all of the loop diuretics produce the same response if given at equipotent doses going above these maximum doses will produce little or no further diuresis but may increase the risk of side effects the maximum effective diuretic dose differs in patients with heart failure, advanced cirrhosis, or renal failure.

32
Diureticaresistentie
worsening renal function during diuresis with a progressively reduced an inadequate response to diuretic drugs diuretic resistance has been described as a component of "cardio-renal syndrome" poorer outcomes (increased morbidity and mortality) in both chronic and acute decompensated heart failure
 in both chronic and acute decompensated heart failure.")
33
Acuut longoedeem -R/afterloadreductie (Cedocard 3mg IV)
-furosemide IV mg -25% blijkt ondervuld

34
Diuretic strategies in patients with acute decompensated heart failure
Felker MG,NEJM, 2011; 364/9:

35
geen verschil tussen continu infuus en bolussen alsook lage en hoge dosissen zowel voor effect als veiligheid in primaire eindpunten in tegenstelling tot eerdere kleine studies: continue infusie beter effect en minder nierfunctiedaling verklaring placebo continu infuus: langer plat liggen: op zich diurese zou bevorderen bolusgroep hogere dosis gekregen dan continue groep hoge dosis: snellere verbetering dyspnoe meer vocht- en gewichtsverlies meer nierinsuffuciëntie

36
Nierinsufficiëntie klassiek thiaziden tot e-GFR 50 ml/min/1,73m²
try and error kaliumsparende tot e-GFR (30)-40 ml/min/1,73m² toevoegen loopdiureticum in dialyse furosemide tot 2x500mg + chlortalidone 100mg/d (‘comfortdiurese’)
-40 ml/min/1,73m². toevoegen loopdiureticum. in dialyse furosemide tot 2x500mg + chlortalidone 100mg/d (‘comfortdiurese’)")
37
Zwangerschap -oedeem = cosmetisch probleem -diuretica af te raden
methyldopa, labetalol, nifedipine postpartum is lage dosis thiazide geen probleem voor borstvoeding

38
Diuretics for preventing pre-eclampsia David Churchill Cochrane Pregnancy and Childbirth Group 24 JAN 2007 no clear benefits with the level of adverse effects found, the use of diuretics for the prevention of pre-eclampsia and its complications cannot be recommended.

39
Levercirrose cave hypokaliëmie spironolactone (ev. + loopdiureticum)
cave hepatorenaal syndroom

40
Idiopatisch cyclisch oedeem
-etiologie onbekend (capillair lek, hormonaal) -klinisch weinig afwijkingen, CVD normaal -eetstoornis? refeeding oeddem? -diuretica-abusus (hypokaliëmie,nierinsufficiëntie) -ZA dieet, diuretica stoppen 3-4 weken -z.n. lage dosis spironolactone, continu
 -klinisch weinig afwijkingen, CVD normaal. -eetstoornis refeeding oeddem -diuretica-abusus (hypokaliëmie,nierinsufficiëntie) -ZA dieet, diuretica stoppen 3-4 weken. -z.n. lage dosis spironolactone, continu.")
41
Zwarten low renin hypertensie
calciumantagonisten >diuretica> ACEi/sartanen-betablokkers

42
Urolithiase zoutarm dieet + thiazide
toename Na-reabsorptie in proximale tubulus gekoppeld aan Ca-reabsorptie cave hypercalcemie (bv. bij fruste hyperparathyreoïdie)
")
43
Besluit onmisbaar ook bij hypertensie laag gedoseerd
kaliumsparend tot e-GFR 40 +zoutbeperking combinatietherapie

47
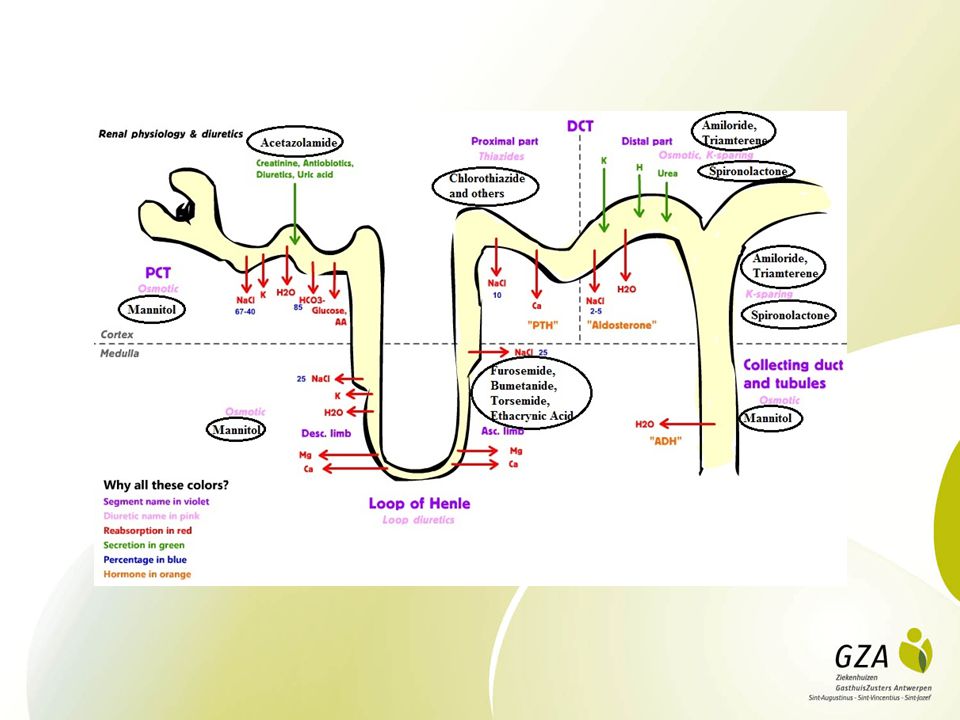
Acetazolamide - Diamox
Proximal tubular diuretics decrease Na+ reabsorption.308 Drugs that work at the site (some of these agents work at other sites as well) include mannitol, an osmotic diuretic, acetazolamide (a carbonic anhydrase inhibitor) and organomercurials. acetazolamide (a carbonic anhydrase inhibitor) The enzyme, carbonic anhydrase exhibits the following characteristics: Its major location is the luminal proximal tubule membrane. Carbonic anhydrase catalyzes dehydration of carbonic acid, H2CO3 , required for bicarbonate reabsorption Blockade of carbonic anhydrase activity induces a sodium bicarbonate diuresis, which reduces body bicarbonate levels Carbonic anhydrase inhibitors are unsubstituted sulfonamides which are bacteriostatic. These agents promote alkaline diuresis and a hyperchloremic metabolic acidosis. Prototype drug: acetazolamide (Diamox) Acetazolamide: (Diamox) is well absorbed orally and is excreted by tubular secretion, at the proximal tubule. In renal insufficiency a dose reduction is appropriate. At maximal carbonic anhydrase inhibition, a 45% inhibition of bicarbonate reabsorption is observed. This level of inhibition results in significant bicarbonate loss and a hyperchloremic metabolic acidosis. Acetazolamide (Diamox) administration causes a reduction in aqueous humor and cerebrospinal fluid production Clinical Application: Glaucoma: Because acetazolamide decreases the rate of aqueous humor production, a decline in intraocular pressure occurs. Management of glaucoma is the most common indication for use of carbonic anhydrase inhibitors. Dorzolamide (Trusopf), another carbonic anhydrase inhibitor exhibits no diuretic or systemic metabolic effect; however, administration of this agent causes a reduction in intraocular pressure. Urinary Alkalinization: Increased uric acid and cystine solubility by alkalinizing the urine (by increasing bicarbonate excretion) For prophylaxis of uric acid renal stones, bicarbonate administration (baking soda) may be required Metabolic Alkalosis: Results from: Decreased total potassium with reduced vascular volume High mineralocorticoid levels These conditions are usually managed by treating the underlying causes; however, in certain clinical settings acetazolamide may assist in correcting alkalosis {e.g. alkalosis due to excessive diuresis in CHF patients} Acute Mountain Sickness: Symptoms: weakness, insomnia, headache, nausea, dizziness {rapid ascension of all of 3000 meters}; symptoms -- usually mild In serious cases: life-threatening cerebral or pulmonary edema Acetazolamide reduces the rate of CSF formation and decreases cerebral spinal fluid pH. Prophylaxis against acute mountain sickness may be appropriate Other Uses: Some role in management of epilepsy Hypokalemia periodic paralysis Increase urinary phosphate excretion during severe hyperphosphatemia. Toxicity: Hyperchloremic metabolic acidosis Due to reduction of body bicarbonate stores Renal stones: Bicarbonate loss is associated with: Phosphaturia Hypercalciuria (calcium salts, relatively insoluble at alkaline pH) Renal potassium loss: Increased sodium bicarbonate in the collecting tubule increases the lumen-negative electrical potential -- enhances potassium excretion Counteracted by potassium chloride administration Others: Drowsiness, parathesias Accumulation in renal failure (CNS toxicity) Hypersensitivity reactions Contraindications: Hepatic cirrhosis Urinary alkalinization will decrease ammonium ion trapping, increasing the likelihood of hepatic encephalopathy. Most proximal tubular agents are not particularly effective when administered as monotherapy. The distal tubule, including the loop of Henle ascending limb, has substantial capability to increase sodium reabsorption rate. As a result, increased sodium load as a result of diuretic activity upstream from the distal tubule can be compensated for by distal tubular transport mechanisms. For this reason, proximal tubular site of action agents are often combined with other drugs.
 include mannitol, an osmotic diuretic, acetazolamide (a carbonic anhydrase inhibitor) and organomercurials. acetazolamide (a carbonic anhydrase inhibitor) The enzyme, carbonic anhydrase exhibits the following characteristics: Its major location is the luminal proximal tubule membrane. Carbonic anhydrase catalyzes dehydration of carbonic acid, H2CO3 , required for bicarbonate reabsorption. Blockade of carbonic anhydrase activity induces a sodium bicarbonate diuresis, which reduces body bicarbonate levels. Carbonic anhydrase inhibitors are unsubstituted sulfonamides which are bacteriostatic. These agents promote alkaline diuresis and a hyperchloremic metabolic acidosis. Prototype drug: acetazolamide (Diamox) Acetazolamide: (Diamox) is well absorbed orally and is excreted by tubular secretion, at the proximal tubule. In renal insufficiency a dose reduction is appropriate. At maximal carbonic anhydrase inhibition, a 45% inhibition of bicarbonate reabsorption is observed. This level of inhibition results in significant bicarbonate loss and a hyperchloremic metabolic acidosis. Acetazolamide (Diamox) administration causes a reduction in aqueous humor and cerebrospinal fluid production. Clinical Application: Glaucoma: Because acetazolamide decreases the rate of aqueous humor production, a decline in intraocular pressure occurs. Management of glaucoma is the most common indication for use of carbonic anhydrase inhibitors. Dorzolamide (Trusopf), another carbonic anhydrase inhibitor exhibits no diuretic or systemic metabolic effect; however, administration of this agent causes a reduction in intraocular pressure. Urinary Alkalinization: Increased uric acid and cystine solubility by alkalinizing the urine (by increasing bicarbonate excretion) For prophylaxis of uric acid renal stones, bicarbonate administration (baking soda) may be required. Metabolic Alkalosis: Results from: Decreased total potassium with reduced vascular volume. High mineralocorticoid levels. These conditions are usually managed by treating the underlying causes; however, in certain clinical settings acetazolamide may assist in correcting alkalosis {e.g. alkalosis due to excessive diuresis in CHF patients} Acute Mountain Sickness: Symptoms: weakness, insomnia, headache, nausea, dizziness {rapid ascension of all of 3000 meters}; symptoms -- usually mild. In serious cases: life-threatening cerebral or pulmonary edema. Acetazolamide reduces the rate of CSF formation and decreases cerebral spinal fluid pH. Prophylaxis against acute mountain sickness may be appropriate. Other Uses: Some role in management of epilepsy. Hypokalemia periodic paralysis. Increase urinary phosphate excretion during severe hyperphosphatemia. Toxicity: Hyperchloremic metabolic acidosis. Due to reduction of body bicarbonate stores. Renal stones: Bicarbonate loss is associated with: Phosphaturia. Hypercalciuria (calcium salts, relatively insoluble at alkaline pH) Renal potassium loss: Increased sodium bicarbonate in the collecting tubule increases the lumen-negative electrical potential -- enhances potassium excretion. Counteracted by potassium chloride administration. Others: Drowsiness, parathesias. Accumulation in renal failure (CNS toxicity) Hypersensitivity reactions. Contraindications: Hepatic cirrhosis. Urinary alkalinization will decrease ammonium ion trapping, increasing the likelihood of hepatic encephalopathy. Most proximal tubular agents are not particularly effective when administered as monotherapy. The distal tubule, including the loop of Henle ascending limb, has substantial capability to increase sodium reabsorption rate. As a result, increased sodium load as a result of diuretic activity upstream from the distal tubule can be compensated for by distal tubular transport mechanisms. For this reason, proximal tubular site of action agents are often combined with other drugs.")
48
DIURETICA

49
ZOUT This article summarizes the evidence behind updates to the 2013 and 2014 Canadian Hypertension Education Program (CHEP) guidelines. * We review the evidence leading to changes to the recommendations for sodium intake and the threshold for starting pharmacotherapy in older adults. * We also review the evidence behind two new recommendations regarding target blood pressure levels in patients with coronary artery disease and the use of resistance exercise by patients with hypertension. Summary of updated recommendations * In older adult patients (age ≥ 80 yr) who do not have diabetes or end organ damage, the systolic blood pressure threshold for starting drug therapy Is 160 mm Hg or higher (revised recommendation, 2014, grade C). The target for systolic blood pressure should be less than 150 mm Hg (new recommendation, 2013, grade C). * When decreasing systolic blood pressure to target levels in patients with established coronary artery disease (especially if isolated systolic hypertension is present), be cautious when the diastolic blood pressure Is ≤ 60 mm Hg because of concerns that myocardial Ischemia might be exacerbated (new recommendation, 2014, grade D). * For patients who do not have hypertension or who have stage 1 hypertension (I.e., systolic pressure mm Hg, diastolic pressure mm Hg), the use of resistance or weight training (such as free weight lifting, fixed-weight lifting, or handgrip exercise) does not adversely Influence blood pressure (revised recommendation, 2013, grade D). * To decrease blood pressure, consider reducing sodium Intake toward 2000 mg (5 g salt or 87 mmol sodium) per day (revised recommendation, 2014, grade A).
 who do not have diabetes or end organ damage, the systolic blood pressure threshold for starting drug therapy Is 160 mm Hg or higher (revised recommendation, 2014, grade C). The target for systolic blood pressure should be less than 150 mm Hg (new recommendation, 2013, grade C). * When decreasing systolic blood pressure to target levels in patients with established coronary artery disease (especially if isolated systolic hypertension is present), be cautious when the diastolic blood pressure Is ≤ 60 mm Hg because of concerns that myocardial Ischemia might be exacerbated (new recommendation, 2014, grade D). * For patients who do not have hypertension or who have stage 1 hypertension (I.e., systolic pressure mm Hg, diastolic pressure mm Hg), the use of resistance or weight training (such as free weight lifting, fixed-weight lifting, or handgrip exercise) does not adversely Influence blood pressure (revised recommendation, 2013, grade D). * To decrease blood pressure, consider reducing sodium Intake toward 2000 mg (5 g salt or 87 mmol sodium) per day (revised recommendation, 2014, grade A).")
50
Loop of Henle diuretics represent the most potent diuretic drugs and act by inhibiting active NaCl transport in the medullary ascending limb.308 The maximal diuretic effect corresponds to about 20%-25% of the filtered sodium load. Examples of loop diuretics include furosemide, torsemide, bumetanide, and ethacrynic acid. Because of their efficacy in blocking Na+ ion transport, these agents are routinely used for managing fluid retention/overload associated with heart failure. Agents include: Furosemide (Lasix) Bumetanide (Bumex) Torsemide (Demadex) Ethycrinic acid --no longer in use because of toxicity. Mechanism of action: Inhibition of NaCl reabsorption in the thick ascending limb of the loop of Henle Inhibit the Na/K/2Cl transport system in the luminal membrane Reduction in sodium chloride reabsorption Decreases normal lumen-positive potential (secondary to potassium recycling) Positive lumen potential: drives divalent cationic reabsorption (calcium magnesium) Therefore, loop diuretics increase magnesium and calcium excretion. Hypomagnesemia may occur in some patients. Hypocalcemia does not usually develop because calcium is reabsorbed in the distal convoluted tubule. {in circumstances that result in hypercalcemia, calcium excretion can be enhanced by administration of loop diuretics with saline infusion} Since a significant percentage of filtered NaCl is absorbed by the thick ascending limb of loop of Henle, diuretics acting at this site are highly effective Loop diuretics--Properties: rapidly absorbed following oral administration (may be administered by IV) Acts rapidly Eliminated by a renal secretion and glomerular filtration (half-life -- depend on renal function) Co-administration of drugs that inhibit weak acid secretion (e.g. probenecid or indomethacin) may alter loop diuretic clearance. Other effects: Furosemide: increases renal blood flow; blood flow redistribution within the renal cortex Furosemide decreases pulmonary congestion and the left ventricular filling pressure in congestive heart failure (CHF) -- prior to an increase in urine output. Clinical uses: Major uses: Acute pulmonary edema Acute hypercalcemia Management of edema Other uses: Hyperkalemia: Loop diuretics increase potassium excretion Effect increased by concurrent administration of NaCl and water. Acute renal failure: May increase rate of urine flow and increase potassium excretion. May convert oligouric to non-oligouric failure {easier clinical management} Renal failure duration is not affected Anion overload: Bromide, chloride, iodide: all reabsorbed by the thick ascending loop: Systemic toxicity may be reduced by decreasing reabsorption Concurrent administration of sodium chloride and fluid is required to prevent volume depletion Toxicity: Hypokalemia metabolic alkalosis: Increased delivery of NaCl and water to the collecting duct increases potassium and proton secretion-- causing a hypokalemic metabolic alkalosis In managed by potassium replacement and by ensuring adequate fluid intake Ototoxicity: Dose-related hearing loss (in usually reversible) Ototoxicity more common: With decreased renal function With concurrent administration of other ototoxic drugs such as aminoglycosides Hyperuricemia: May cause gout Loop diuretics cause increased uric acid reabsorption in the proximal tubule, secondary to hypovolemic states. Hypomagnesemia: loop diuretics cause: Reduction in sodium chloride reabsorption Decreases normal lumen-positive potential (secondary to potassium recycling) Positive lumen potential: drives divalent cationic reabsorption (calcium magnesium) Therefore, loop diuretics increase magnesium and calcium excretion. Reversed by oral magnesium administration Allergic reactions: Furosemide: skin rash, eosinophilia, interstitial nephritis(less often) Other toxicities: Dehydration (may be severe) Hyponatremia (less common than with thiazides thought may occur in patients who increased water intake in response to a hypovolemic thirst) Hypercalcemia may occur in severe dehydration and if a hypercalcemia condition {e.g. oat cell long carcinoma} is also present. Loopdiuretica
 Bumetanide (Bumex) Torsemide (Demadex) Ethycrinic acid --no longer in use because of toxicity. Mechanism of action: Inhibition of NaCl reabsorption in the thick ascending limb of the loop of Henle. Inhibit the Na/K/2Cl transport system in the luminal membrane. Reduction in sodium chloride reabsorption. Decreases normal lumen-positive potential (secondary to potassium recycling) Positive lumen potential: drives divalent cationic reabsorption (calcium magnesium) Therefore, loop diuretics increase magnesium and calcium excretion. Hypomagnesemia may occur in some patients. Hypocalcemia does not usually develop because calcium is reabsorbed in the distal convoluted tubule. {in circumstances that result in hypercalcemia, calcium excretion can be enhanced by administration of loop diuretics with saline infusion} Since a significant percentage of filtered NaCl is absorbed by the thick ascending limb of loop of Henle, diuretics acting at this site are highly effective. Loop diuretics--Properties: rapidly absorbed following oral administration (may be administered by IV) Acts rapidly. Eliminated by a renal secretion and glomerular filtration (half-life -- depend on renal function) Co-administration of drugs that inhibit weak acid secretion (e.g. probenecid or indomethacin) may alter loop diuretic clearance. Other effects: Furosemide: increases renal blood flow; blood flow redistribution within the renal cortex. Furosemide decreases pulmonary congestion and the left ventricular filling pressure in congestive heart failure (CHF) -- prior to an increase in urine output. Clinical uses: Major uses: Acute pulmonary edema. Acute hypercalcemia. Management of edema. Other uses: Hyperkalemia: Loop diuretics increase potassium excretion. Effect increased by concurrent administration of NaCl and water. Acute renal failure: May increase rate of urine flow and increase potassium excretion. May convert oligouric to non-oligouric failure {easier clinical management} Renal failure duration is not affected. Anion overload: Bromide, chloride, iodide: all reabsorbed by the thick ascending loop: Systemic toxicity may be reduced by decreasing reabsorption. Concurrent administration of sodium chloride and fluid is required to prevent volume depletion. Toxicity: Hypokalemia metabolic alkalosis: Increased delivery of NaCl and water to the collecting duct increases potassium and proton secretion-- causing a hypokalemic metabolic alkalosis. In managed by potassium replacement and by ensuring adequate fluid intake. Ototoxicity: Dose-related hearing loss (in usually reversible) Ototoxicity more common: With decreased renal function. With concurrent administration of other ototoxic drugs such as aminoglycosides. Hyperuricemia: May cause gout. Loop diuretics cause increased uric acid reabsorption in the proximal tubule, secondary to hypovolemic states. Hypomagnesemia: loop diuretics cause: Reduction in sodium chloride reabsorption. Decreases normal lumen-positive potential (secondary to potassium recycling) Positive lumen potential: drives divalent cationic reabsorption (calcium magnesium) Therefore, loop diuretics increase magnesium and calcium excretion. Reversed by oral magnesium administration. Allergic reactions: Furosemide: skin rash, eosinophilia, interstitial nephritis(less often) Other toxicities: Dehydration (may be severe) Hyponatremia (less common than with thiazides thought may occur in patients who increased water intake in response to a hypovolemic thirst) Hypercalcemia may occur in severe dehydration and if a hypercalcemia condition {e.g. oat cell long carcinoma} is also present. Loopdiuretica.")
51
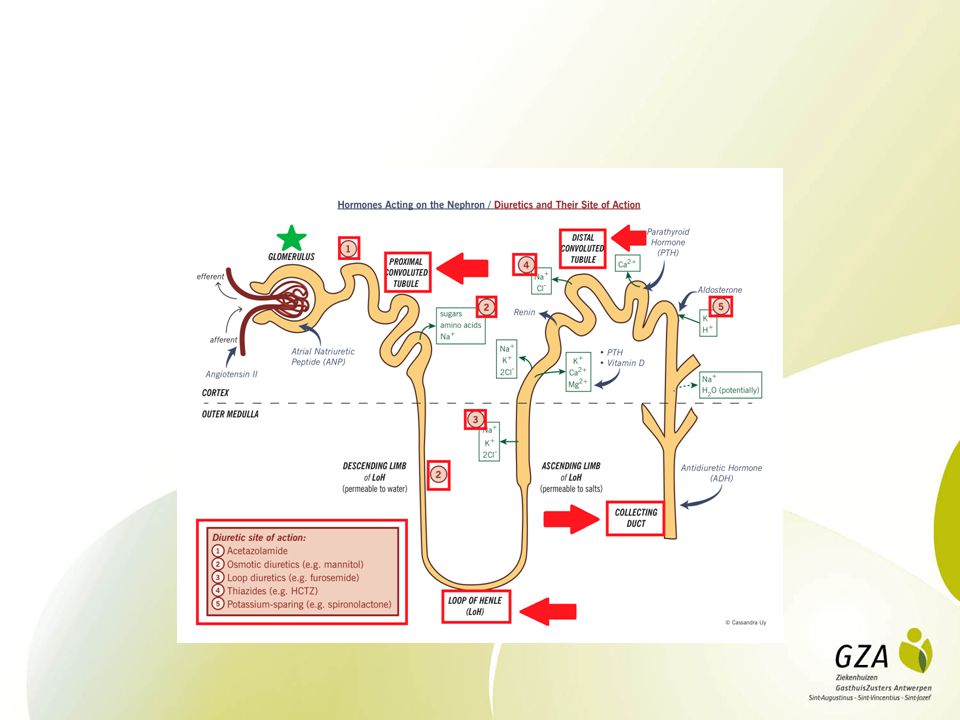
Distal tubular diuretics include both K+ -sparing and K+ -non-sparing agents.308
Among the K+ -non-sparing drugs are thiazide diuretics, chlorthalidone (Hygroton), and metazolone (Mykrox). These agents reduce Na+ absorption in the cortical segment of the ascending limb of the loop of Henle and distal convoluted tubule. Since distal tubular diuretics act proximal to the distal site of K+ secretion, these drugs increase urinary K+excretion. Resulting hypokalemia is an noteworthy clinical consequence and may require treatment. As noted earlier, hyperkalemia may precipitate life-threatened ventricular tachyarrhythmias, the likelihood of which is increased by cardiac glycoside or other positive inotropic agent therapy. By contrast, there are a number of K+-sparing agents including triamterine, amiloride, and aldosterone antagonists such as spirolactone and eplerenone.308 Triamterine and amiloride inhibit K+ secretion independent of adrenal function; however, spirolactone and eplerenone activity depend on both circulating aldosterone and an intact adrenal cortex. K+ -sparing agents lack sufficient potency to be used as monotherapy but can attenuate or eliminate K+ loss (and thus hypokalemia) associated with diuretics acting more proximal locations. Two major, common consequences of diuretic treatment are K+ loss and volume depletion.308 Frequently used agent such as thiazide diuretics, metazolone, and loop diuretics are associated with these adverse effects. Volume depletion can cause hypotension and hypoperfusion. With hypoperfusion, inadequate blood flow to critical organs may cause severe end-organ damage. Reduced renal function may also occur even in the presence of hypervolemia. Reduced kidney perfusion may manifest by an increase in both blood urea nitrogen (BUN) and serum creatinine levels. Worsening of kidney function may be expected in about a third of patients exhibiting acute, decompensated heart failure. Serious renal hypoperfusion itself can precipitate intrinsic renal failure associated with acute tubular necrosis, in addition to prerenal azotemia.308 Prerenal azotemia is associated with high blood levels of nitrogen-containing chemicals such as urea, creatinine, etc. due to inadequate glomerular filtration rates, specifically resulting from renal hypoperfusion. The BUN: creatinine ratio in prerenal azotemia may be >20. Heart failure patient should be evaluated and monitored for both hyperkalemia and hypokalemia. Either condition can precipitate cardiac excitability and/or conduction changes which may lead to sudden death.329,330 In an effort to maintain organ perfusion during heart failure, activation of both sympathetic nervous system and renin-angiotensin system can cause hypokalemia.329,331,332 As noted above, many drugs used in management of heart failure can change K+ serum levels.329,333 Serum potassium levels should be in the mmol/L range. Small decreases in serum K+ increase risk associated with antiarrhythmic drug and cardiac glycoside treatment330,334; furthermore, small increases in serum K+ may prevent use of treatments known to extend life.335 In some patient subsets, low serum K+ may require supplementation of potassium and magnesium; whereas, in other patient subsets, especially those taking angiotensin-converting enzyme inhibitors (ACE inhibitors), either as monotherapy or in combination with aldosterone antagonists, potassium salts may be both unnecessary and potentially harmful.329 Hyponatremias can occur due to impaired water excretion, secondary to chronic heart failure.308 Increased NaCl excretion by commonly used diuretics in heart failure management can either cause or worsen hyponatremic in patients with advanced heart failure, absent fluid intake restriction. Water restriction may be used to manage symptomatic hyponatremia. Carbonic anhydrase inhibitors, e.g. acetazolamide administration may result in a metabolic acidosis due to reduced H+ ion secretion.308 Thiazide and loop diuretic administration may cause metabolic alkalosis, secondary to Na+, Cl-, and K+ excretion with bicarbonate retention.308
, and metazolone (Mykrox). These agents reduce Na+ absorption in the cortical segment of the ascending limb of the loop of Henle and distal convoluted tubule. Since distal tubular diuretics act proximal to the distal site of K+ secretion, these drugs increase urinary K+excretion. Resulting hypokalemia is an noteworthy clinical consequence and may require treatment. As noted earlier, hyperkalemia may precipitate life-threatened ventricular tachyarrhythmias, the likelihood of which is increased by cardiac glycoside or other positive inotropic agent therapy. By contrast, there are a number of K+-sparing agents including triamterine, amiloride, and aldosterone antagonists such as spirolactone and eplerenone.308. Triamterine and amiloride inhibit K+ secretion independent of adrenal function; however, spirolactone and eplerenone activity depend on both circulating aldosterone and an intact adrenal cortex. K+ -sparing agents lack sufficient potency to be used as monotherapy but can attenuate or eliminate K+ loss (and thus hypokalemia) associated with diuretics acting more proximal locations. Two major, common consequences of diuretic treatment are K+ loss and volume depletion.308. Frequently used agent such as thiazide diuretics, metazolone, and loop diuretics are associated with these adverse effects. Volume depletion can cause hypotension and hypoperfusion. With hypoperfusion, inadequate blood flow to critical organs may cause severe end-organ damage. Reduced renal function may also occur even in the presence of hypervolemia. Reduced kidney perfusion may manifest by an increase in both blood urea nitrogen (BUN) and serum creatinine levels. Worsening of kidney function may be expected in about a third of patients exhibiting acute, decompensated heart failure. Serious renal hypoperfusion itself can precipitate intrinsic renal failure associated with acute tubular necrosis, in addition to prerenal azotemia.308. Prerenal azotemia is associated with high blood levels of nitrogen-containing chemicals such as urea, creatinine, etc. due to inadequate glomerular filtration rates, specifically resulting from renal hypoperfusion. The BUN: creatinine ratio in prerenal azotemia may be >20. Heart failure patient should be evaluated and monitored for both hyperkalemia and hypokalemia. Either condition can precipitate cardiac excitability and/or conduction changes which may lead to sudden death.329,330. In an effort to maintain organ perfusion during heart failure, activation of both sympathetic nervous system and renin-angiotensin system can cause hypokalemia.329,331,332. As noted above, many drugs used in management of heart failure can change K+ serum levels.329,333. Serum potassium levels should be in the mmol/L range. Small decreases in serum K+ increase risk associated with antiarrhythmic drug and cardiac glycoside treatment330,334; furthermore, small increases in serum K+ may prevent use of treatments known to extend life.335. In some patient subsets, low serum K+ may require supplementation of potassium and magnesium; whereas, in other patient subsets, especially those taking angiotensin-converting enzyme inhibitors (ACE inhibitors), either as monotherapy or in combination with aldosterone antagonists, potassium salts may be both unnecessary and potentially harmful.329. Hyponatremias can occur due to impaired water excretion, secondary to chronic heart failure.308. Increased NaCl excretion by commonly used diuretics in heart failure management can either cause or worsen hyponatremic in patients with advanced heart failure, absent fluid intake restriction. Water restriction may be used to manage symptomatic hyponatremia. Carbonic anhydrase inhibitors, e.g. acetazolamide administration may result in a metabolic acidosis due to reduced H+ ion secretion.308. Thiazide and loop diuretic administration may cause metabolic alkalosis, secondary to Na+, Cl-, and K+ excretion with bicarbonate retention.308.")
54
Authors' conclusions We found predominantly moderate quality evidence that all-cause mortality is similar when first-line RAS inhibitors are compared to other first-line antihypertensive agents. First-line thiazides caused less HF and stroke than first-line RAS inhibitors.

55
Dosis largest reduction in blood pressure at a half-standard dose
only modestly greater reductions in systolic and diastolic blood pressures at standard or twice-standard doses average fall in systolic blood pressure over 24 hours with half-standard, standard, and twice-standard doses was 7.1, 9.1, and 10.9 mmHg with data from all classes combined and 7.4, 8.8, and 10.3 mmHg with a thiazide diuretic with thiazide diuretics, calcium channel blockers, and beta blockers, the rate of symptomatic and metabolic adverse effects increased significantly with standard or twice-standard doses compared to half-standard doses after the initial dose, going to higher doses produced on average relatively small further reductions in blood pressure at the price of an increasing rate of adverse effects. As a result, we generally limit dose titration to one step with a given antihypertensive drug (eg, 12,5 to 25 mg of chlortalidone)
")
56
Schematic representation of the transport mechanisms in the distal tubule. The Na-K-ATPase pump in the basolateral (peritubular) membrane pumps sodium (Na) out of, and potassium (K) into, the cell. This creates a low intracellular Na concentration which drives many of the cell's reabsorptive processes. The entry of filtered Na and chloride (Cl) into the cell is mediated by a neutral Na-Cl cotransporter NCCT in the apical (luminal) membrane. This cotransporter is inhibited by thiazide diuretics. The energy for this process is provided by the favorable inward electrochemical gradient for Na (the intracellular Na concentration is very low and the cell interior is electronegative). The reabsorbed Na which has entered the cell is pumped out by the Na-K-ATPase pump. The reabsorbed Cl exits via a chloride channel. This is the ClC-Kb channel which requires interaction with a small protein called barttin to function normally. The distal tubule is also a major site of active calcium (Ca) reabsorption. Ca enters the cell via a Ca transporter that is probably a Ca channel. Reabsorbed Ca combines with a vitamin D-induced Ca binding protein (Ca-BP), moves across the cell, and is then extruded at the basolateral membrane by a Ca-ATPase (not shown) and a 3Na:1Ca exchanger that also uses the energy provided by the favorable inward electrochemical gradient for Na.
 membrane pumps sodium (Na) out of, and potassium (K) into, the cell. This creates a low intracellular Na concentration which drives many of the cell s reabsorptive processes. The entry of filtered Na and chloride (Cl) into the cell is mediated by a neutral Na-Cl cotransporter NCCT in the apical (luminal) membrane. This cotransporter is inhibited by thiazide diuretics. The energy for this process is provided by the favorable inward electrochemical gradient for Na (the intracellular Na concentration is very low and the cell interior is electronegative). The reabsorbed Na which has entered the cell is pumped out by the Na-K-ATPase pump. The reabsorbed Cl exits via a chloride channel. This is the ClC-Kb channel which requires interaction with a small protein called barttin to function normally. The distal tubule is also a major site of active calcium (Ca) reabsorption. Ca enters the cell via a Ca transporter that is probably a Ca channel. Reabsorbed Ca combines with a vitamin D-induced Ca binding protein (Ca-BP), moves across the cell, and is then extruded at the basolateral membrane by a Ca-ATPase (not shown) and a 3Na:1Ca exchanger that also uses the energy provided by the favorable inward electrochemical gradient for Na..")
57
●Patients with generalized edema (due for example to heart failure, the nephrotic syndrome, or renal disease) are typically treated with daily therapy. At a given dose, net sodium loss occurs for only one to two weeks before a new steady state is achieved; in this setting, sodium intake and excretion are again equal as the effect of the diuretic is balanced by activation of counterregulatory factors that promote sodium retention, such as the renin-angiotensin system. However, selected patients with mild edema who comply with dietary sodium restriction can be treated with intermittent therapy as needed.

58
Inleiding DOSE trial: Diuretic Optimization Strategies Evaluation
National Heart, Lung and Blood Institute Heart Failure Clinical Research Network Clinical trial Prospectief, gerandomiseerd, dubbel blind gecontroleerde studie Exclusie: Systolische BD < 90 mmHg Serum creatinine > 3mg/dl Nood aan IV vasodilatators of inotropica (andere dan digoxine)
")
59
Studie Inclusie: < 24uur presenteren mat acuut hartfalen
Minstens 1 vd volgende symptomen: Dyspnoe Orthopnoe Oedeem En 1 vd volgende tekens: Ronchi Perifere oedemen Ascites Stuwing op rx thorax

60
Inleiding Acuut hartfalen Gebreken ikv diuretische behandeling:
Frequentste oorzaak van hospitalisatie pt > 65j Standaard behandeling: diuretica Gebreken ikv diuretische behandeling: Guidelines zijn vooral expert opion => sterke variabiliteit zowel in dosage als toedieningsvorm Hoge dosages potentieel schadelijk: Activatie RAAS en sympatisch ZS Elektrolytstoornissen Achteruitgang nierfunctie Toedieningsvorm: Farmacokinetische en dynamische data: continu > intermittent bolussen MAAR studies hierover waren klein en hadden onvoldoende power

61
Studie Opzet: 2 groepen Lage dosis: totale dagelijkse IV dosis = eigen totale orale diuretica in furosemide equivalente Hoge dosis: totale dagelijkse IV dosis = 2,5 x eigen totale orale diuretica in furosemide equivalente IV therapie Bolussen om de 12uur Continue Dubbelblind: alle pt krijgen zowel continu infuus en bolussen met fysiologisch als placebo follow up biomarkers: creatinine, BNP en cystatine C Follow up gedurende 60dagen

62
Studie Eindpunten: Primaire: Secundaire
Globale assesment van symptomen ahv VAS tot 72uur serum creatinine tot 72uur Secundaire Dyspnoe ahv VAS Verandering in lichaamsgewicht Netto vochtverlies Ratio van pt vrij van congestie (CVS < 8cm, geen orthopnoe) op 72uur Achteruitgang nf (toename crea > 0,3mg/dl) Achteruitgang of aanhoudend hartfalen Verandering in biomarkers op 72uur, op 7dagen of op moment van ontslag en op dag 60 Overlijden, rehospitalisatie, spoed consulten, aantal gehospitaliseerde dagen. Studie
 op 72uur. Achteruitgang nf (toename crea > 0,3mg/dl) Achteruitgang of aanhoudend hartfalen. Verandering in biomarkers op 72uur, op 7dagen of op moment van ontslag en op dag 60. Overlijden, rehospitalisatie, spoed consulten, aantal gehospitaliseerde dagen. Studie.")
63
Secondary End Points for Each Treatment Comparison.
Felker GM et al. N Engl J Med 2011;364:

64
Discussie Eerdere studie: hoge dosis diuretica => achteruitgang nf => slechtere outcome Hoge dosis: frequenter achteruitgang nf op korte termijn, op 60 dagen geen verschil Recent studies: transiënte achteruitgang nf geen effect zou hebben op outcome na ontslag. Beperkingen: Chronische pt die ambulant reeds hoge dosissen Zegt niets over nieuwe diagnose Vele pt kregen reeds diuretica in periode voor randomisatie en mogelijkheid tot aanpassen dosis na 48uur

65
Increase in urinary sodium excretion (UNa) after intravenous bumetanide, given as a continuous infusion (solid line) or as a bolus (dashed line), in patients with stable chronic kidney disease. The continuous infusion produced a 30 percent greater increase in sodium excretion than bolus therapy due to a more favorable rate of diuretic excretion. In addition, the natriuretic response declined over time with both regimens. With the bolus, for example, the peak natriuretic response to the second dose was 25 percent less than that to the first. Rudy DW,Ann Intern Med 1991; 115:360

66
furosemide, furosemide prolongatum bumetamide torasemide chlortalidone
acetazolamide ethacrynezuur furosemide, furosemide prolongatum bumetamide torasemide chlortalidone hydrochlorothiazide triamterene amiloride spironolactone canrenol eplerone vaptanen combinaties: amiloride 5mg + furosemide 40mg amiloride 5mg + HCTZ 50mg (Moduretic) spironolactone 25mg+HCTZ25mg HCTZ 25mg + triamterene 50mg (Dytenzide) amiloride 5mg+HCTZ50mg
 spironolactone 25mg+HCTZ25mg. HCTZ 25mg + triamterene 50mg (Dytenzide) amiloride 5mg+HCTZ50mg.")
Verwante presentaties












>")







![Deltion College Engels B2 Spreken/presentaties/subvaardigheid lezen [Edu/003] thema: Holland – coffee shops and euthanasia? can-do : kan een duidelijk.](/10/2833741/big_thumb.jpg "Deltion College Engels B2 Spreken/presentaties/subvaardigheid lezen [Edu/003] thema: Holland – coffee shops and euthanasia? can-do : kan een duidelijk.>")
. Lancet 1996;348:>")
![Deltion College Engels B1 Gesprekken voeren [Edu/006] thema: Look, it says ‘No smoking’… can-do : kan minder routinematige zaken regelen © Anne Beeker.](/10/2924527/big_thumb.jpg "Deltion College Engels B1 Gesprekken voeren [Edu/006] thema: Look, it says ‘No smoking’… can-do : kan minder routinematige zaken regelen © Anne Beeker.>")