Download de presentatie
De presentatie wordt gedownload. Even geduld aub

1
glycemiebeleid bij type 2 diabetes : “treat to target”
lesmodule Diabetes Project Aalst opgesteld door de werkgroep huisartsen-specialisten

2
Waarom scherpe HbA1c nastreven bij type 2 diabetes ?

3
goede glycemiecontrole complicaties
Improving the Prognosis of Patients with Type 2 Diabetes Slide 46. UKPDS: Association of Hyperglycaemia and Complications. Type 2 diabetes United Kingdom Prospective Diabetes Study (UKPDS) 60 50 Myocardial 40 infarction % Incidence per 1000 patient years The consequences of failure-based management approaches in diabetes can be severe, as inadequate control of blood glucose causes unnecessary exposure of patients to additional risk of microvascular and macrovascular complications. In UKPDS, increasing HbA1C from 6% to 9% approximately doubles the risk of a myocardial infarction. In addition, the risk of microvascular complications increases markedly as HbA1C rises. Management approaches which achieve near normal glycaemic control are likely to have the biggest impact in reducing the incidence of heart attacks. 30 Microvascular disease 20 10 <6 6-<7 7-<8 8-<9 9-<10 10+ Updated HbA1c (%) UKPDS 35. BMJ 2000; 321:
 Myocardial. 40. infarction. % Incidence per 1000 patient years. The consequences of failure-based management approaches in diabetes can be severe, as inadequate control of blood glucose causes unnecessary exposure of patients to additional risk of microvascular and macrovascular complications. In UKPDS, increasing HbA1C from 6% to 9% approximately doubles the risk of a myocardial infarction. In addition, the risk of microvascular complications increases markedly as HbA1C rises. Management approaches which achieve near normal glycaemic control are likely to have the biggest impact in reducing the incidence of heart attacks. 30. Microvascular. disease <6. 6-<7. 7-<8. 8-<9. 9-< Updated HbA1c (%) UKPDS 35. BMJ 2000; 321:")
4
goede glycemiecontrole complicaties
Improving the Prognosis of Patients with Type 2 Diabetes Slide 46. UKPDS: Association of Hyperglycaemia and Complications. Type 2 diabetes United Kingdom Prospective Diabetes Study (UKPDS) 60 HbA1c 7 à 7.5 % 50 Myocardial 40 infarction % Incidence per 1000 patient years The consequences of failure-based management approaches in diabetes can be severe, as inadequate control of blood glucose causes unnecessary exposure of patients to additional risk of microvascular and macrovascular complications. In UKPDS, increasing HbA1C from 6% to 9% approximately doubles the risk of a myocardial infarction. In addition, the risk of microvascular complications increases markedly as HbA1C rises. Management approaches which achieve near normal glycaemic control are likely to have the biggest impact in reducing the incidence of heart attacks. 30 Microvascular disease 20 10 <6 6-<7 7-<8 8-<9 9-<10 10+ Updated HbA1c (%) UKPDS 35. BMJ 2000; 321:
 60. HbA1c 7 à 7.5 % 50. Myocardial. 40. infarction. % Incidence per 1000 patient years. The consequences of failure-based management approaches in diabetes can be severe, as inadequate control of blood glucose causes unnecessary exposure of patients to additional risk of microvascular and macrovascular complications. In UKPDS, increasing HbA1C from 6% to 9% approximately doubles the risk of a myocardial infarction. In addition, the risk of microvascular complications increases markedly as HbA1C rises. Management approaches which achieve near normal glycaemic control are likely to have the biggest impact in reducing the incidence of heart attacks. 30. Microvascular. disease <6. 6-<7. 7-<8. 8-<9. 9-< Updated HbA1c (%) UKPDS 35. BMJ 2000; 321:")
5
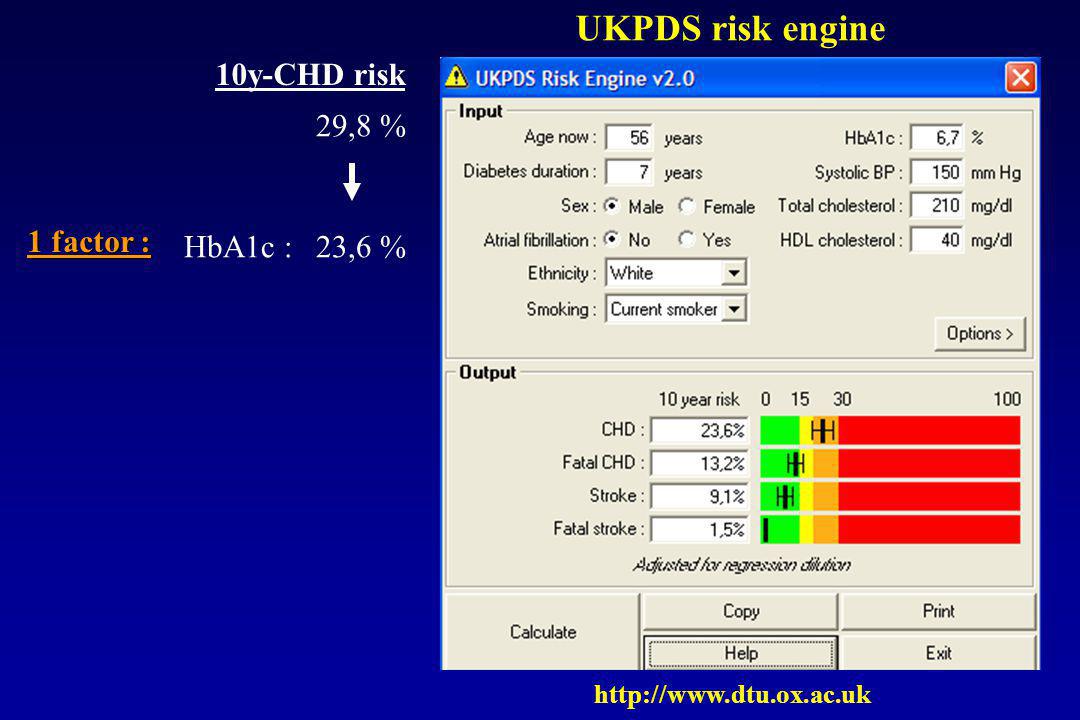
UKPDS risk engine

6
UKPDS risk engine 10y-CHD risk 29,8 %

7
UKPDS risk engine 10y-CHD risk 29,8 % 1 factor : HbA1c : 23,6 %
8
UKPDS risk engine 10y-CHD risk 29,8 % 1 factor : HbA1c : 23,6 %
smoking : 23,0 %

9
UKPDS risk engine 10y-CHD risk 29,8 % 1 factor : HbA1c : 23,6 %
smoking : 23,0 % BP : 27,7 %

10
UKPDS risk engine 10y-CHD risk 29,8 % 1 factor : HbA1c : 23,6 %
smoking : 23,0 % BP : 27,7 % lipids : 21,4 %

11
UKPDS risk engine 10y-CHD risk 29,8 % 1 factor : HbA1c : 23,6 %
smoking : 23,0 % BP : 27,7 % lipids : 21,4 % smoking, BP, lipids : 15,1 %

12
UKPDS risk engine 10y-CHD risk 29,8 % 1 factor : HbA1c : 23,6 %
smoking : 23,0 % BP : 27,7 % lipids : 21,4 % smoking, BP, lipids : 15,1 % idem + HbA1c : 11,8 %

13
goede glycemiecontrole complicaties
Improving the Prognosis of Patients with Type 2 Diabetes Slide 46. UKPDS: Association of Hyperglycaemia and Complications. Type 2 diabetes United Kingdom Prospective Diabetes Study (UKPDS) 60 HbA1c 7 à 7.5 % 50 Myocardial 40 infarction % Incidence per 1000 patient years The consequences of failure-based management approaches in diabetes can be severe, as inadequate control of blood glucose causes unnecessary exposure of patients to additional risk of microvascular and macrovascular complications. In UKPDS, increasing HbA1C from 6% to 9% approximately doubles the risk of a myocardial infarction. In addition, the risk of microvascular complications increases markedly as HbA1C rises. Management approaches which achieve near normal glycaemic control are likely to have the biggest impact in reducing the incidence of heart attacks. 30 Microvascular disease 20 10 <6 6-<7 7-<8 8-<9 9-<10 10+ Updated HbA1c (%) UKPDS 35. BMJ 2000; 321:
 60. HbA1c 7 à 7.5 % 50. Myocardial. 40. infarction. % Incidence per 1000 patient years. The consequences of failure-based management approaches in diabetes can be severe, as inadequate control of blood glucose causes unnecessary exposure of patients to additional risk of microvascular and macrovascular complications. In UKPDS, increasing HbA1C from 6% to 9% approximately doubles the risk of a myocardial infarction. In addition, the risk of microvascular complications increases markedly as HbA1C rises. Management approaches which achieve near normal glycaemic control are likely to have the biggest impact in reducing the incidence of heart attacks. 30. Microvascular. disease <6. 6-<7. 7-<8. 8-<9. 9-< Updated HbA1c (%) UKPDS 35. BMJ 2000; 321:")
14
naar welke glycemie streven om een bepaalde HbA1c te bereiken ?
Yki-Järvinen H, et al. Ann Intern Med 1999;130:389-96 nuchtere glycemie mg/dl

15
Combinatie orale antidiabetica + NPH of glargine
"Treat-to-Target" = haalbaar ! Combinatie orale antidiabetica + NPH of glargine 756 patients Mean FPG (mg/dL) level during study (both groups) Mean HbA1c (%) level during study (both groups) 9.0 8.5 8.0 7.5 7.0 6.5 250 200 150 120 100 8.6 7.5 7.1 6.9 206 175 159 142 135 128 121 118 117 153 135 125 116 5 10 15 20 5 10 15 20 Weeks in study Weeks in study “Treat-to-Target Trial” Riddle MC et al. Diab Care 2003;26:3080-6
 level during study. (both groups) Mean HbA1c (%) level during study. (both groups) Weeks in study. Weeks in study. Treat-to-Target Trial Riddle MC et al. Diab Care 2003;26:")
16
hypoglycemie : type 2 ≠ type 1 !

17
progressieve achteruitgang van de -cell functie bij type 2 diabetes
100 ? 80 60 -cell function (% ) 40 20 10 9 8 7 6 5 4 3 2 1 1 2 3 4 5 6 Years Adapted from UK Prospective Diabetes Study (UKPDS) Group. Diabetes 1995
 10. 9. 8. 7. 6. 5. 4. 3. 2. Years. Adapted from UK Prospective Diabetes Study (UKPDS) Group. Diabetes")
18
treat to target : HbA1c 7% 7%
Dieet en Lichaams- beweging Monotherapie (metformine voorkeur) Combinatie van Orale Antidiabetica Insuline +/- Orale Antidiabetica Current Treatment Paradigm This slide shows unpublished survey data from primary care physicians in the US. The figures on the arrow show the average values of fasting plasma glucose at which the physicians were prepared to intervene to intensify therapy with each type of regimen. Primary care physicians were more likely to intensify antidiabetic therapy at a time when control of glycaemia has already been lost Physicians tolerated higher severities of hyperglycaemia as the complexity of the antidiabetic regimen increased 7%
 Combinatie van Orale Antidiabetica. Insuline. +/- Orale Antidiabetica. Current Treatment Paradigm. This slide shows unpublished survey data from primary care physicians in the US. The figures on the arrow show the average values of fasting plasma glucose at which the physicians were prepared to intervene to intensify therapy with each type of regimen. Primary care physicians were more likely to intensify antidiabetic therapy at a time when control of glycaemia has already been lost. Physicians tolerated higher severities of hyperglycaemia as the complexity of the antidiabetic regimen increased. 7%")
19
treat to target : HbA1c 7% 7%
Leg aan patiënt bij de diagnose uit dat de pancreas verder gaat “verslijten” en dat de pilletjes geleidelijk zullen moeten opgedreven worden en uiteindelijk insuline nodig zal zijn ! Dieet en Lichaams- beweging Monotherapie (metformine voorkeur) Combinatie van Orale Antidiabetica Insuline +/- Orale Antidiabetica Current Treatment Paradigm This slide shows unpublished survey data from primary care physicians in the US. The figures on the arrow show the average values of fasting plasma glucose at which the physicians were prepared to intervene to intensify therapy with each type of regimen. Primary care physicians were more likely to intensify antidiabetic therapy at a time when control of glycaemia has already been lost Physicians tolerated higher severities of hyperglycaemia as the complexity of the antidiabetic regimen increased 7%
 Combinatie van Orale Antidiabetica. Insuline. +/- Orale Antidiabetica. Current Treatment Paradigm. This slide shows unpublished survey data from primary care physicians in the US. The figures on the arrow show the average values of fasting plasma glucose at which the physicians were prepared to intervene to intensify therapy with each type of regimen. Primary care physicians were more likely to intensify antidiabetic therapy at a time when control of glycaemia has already been lost. Physicians tolerated higher severities of hyperglycaemia as the complexity of the antidiabetic regimen increased. 7%")
20
Reageer op tijd ! 7% Dieet en Lichaams- beweging Monotherapie
(metformine voorkeur) Combinatie van Orale Antidiabetica Insuline +/- Orale Antidiabetica Current Treatment Paradigm This slide shows unpublished survey data from primary care physicians in the US. The figures on the arrow show the average values of fasting plasma glucose at which the physicians were prepared to intervene to intensify therapy with each type of regimen. Primary care physicians were more likely to intensify antidiabetic therapy at a time when control of glycaemia has already been lost Physicians tolerated higher severities of hyperglycaemia as the complexity of the antidiabetic regimen increased 7%
 Combinatie van Orale Antidiabetica. Insuline. +/- Orale Antidiabetica. Current Treatment Paradigm. This slide shows unpublished survey data from primary care physicians in the US. The figures on the arrow show the average values of fasting plasma glucose at which the physicians were prepared to intervene to intensify therapy with each type of regimen. Primary care physicians were more likely to intensify antidiabetic therapy at a time when control of glycaemia has already been lost. Physicians tolerated higher severities of hyperglycaemia as the complexity of the antidiabetic regimen increased. 7%")
21
Reageer op tijd ! 8% 7% Monotherapie (metformine voorkeur)
Combinatie van Orale Antidiabetica Insuline +/- Orale Antidiabetica 150 mg% 8 % Dieet en Lichaams- beweging 8% Current Treatment Paradigm This slide shows unpublished survey data from primary care physicians in the US. The figures on the arrow show the average values of fasting plasma glucose at which the physicians were prepared to intervene to intensify therapy with each type of regimen. Primary care physicians were more likely to intensify antidiabetic therapy at a time when control of glycaemia has already been lost Physicians tolerated higher severities of hyperglycaemia as the complexity of the antidiabetic regimen increased 7%

22
Reageer op tijd ! 9% 8% 7% Combinatie van Orale Antidiabetica Insuline
170 mg% 9 % Monotherapie (metformine voorkeur) 9% 150 mg% 8 % Dieet en Lichaams- beweging 8% Current Treatment Paradigm This slide shows unpublished survey data from primary care physicians in the US. The figures on the arrow show the average values of fasting plasma glucose at which the physicians were prepared to intervene to intensify therapy with each type of regimen. Primary care physicians were more likely to intensify antidiabetic therapy at a time when control of glycaemia has already been lost Physicians tolerated higher severities of hyperglycaemia as the complexity of the antidiabetic regimen increased 7%
 9% 150 mg% 8 % Dieet en Lichaams- beweging. 8% Current Treatment Paradigm. This slide shows unpublished survey data from primary care physicians in the US. The figures on the arrow show the average values of fasting plasma glucose at which the physicians were prepared to intervene to intensify therapy with each type of regimen. Primary care physicians were more likely to intensify antidiabetic therapy at a time when control of glycaemia has already been lost. Physicians tolerated higher severities of hyperglycaemia as the complexity of the antidiabetic regimen increased. 7%")
23
Reageer op tijd ! 10% 9% 8% 7% 220 mg% 10 % Insuline
+/- Orale Antidiabetica 220 mg% 10 % Combinatie van Orale Antidiabetica 10% 170 mg% 9 % Monotherapie (metformine voorkeur) 9% 150 mg% 8 % Dieet en Lichaams- beweging 8% Current Treatment Paradigm This slide shows unpublished survey data from primary care physicians in the US. The figures on the arrow show the average values of fasting plasma glucose at which the physicians were prepared to intervene to intensify therapy with each type of regimen. Primary care physicians were more likely to intensify antidiabetic therapy at a time when control of glycaemia has already been lost Physicians tolerated higher severities of hyperglycaemia as the complexity of the antidiabetic regimen increased 7%
 9% 150 mg% 8 % Dieet en Lichaams- beweging. 8% Current Treatment Paradigm. This slide shows unpublished survey data from primary care physicians in the US. The figures on the arrow show the average values of fasting plasma glucose at which the physicians were prepared to intervene to intensify therapy with each type of regimen. Primary care physicians were more likely to intensify antidiabetic therapy at a time when control of glycaemia has already been lost. Physicians tolerated higher severities of hyperglycaemia as the complexity of the antidiabetic regimen increased. 7%")
24
Hoe praktisch organiseren ?

25
praktisch reageer zodra HbA1c > 7.5 %
optimaliseer levens-stijlmaatregelen optimaliseer orale antidiabetica overweeg glycemie zelfcontrole

26
klasse generische naam producten biguaniden metformine Glucophage®, Metformax®, Merck-metformine® gliniden repaglinide NovoNorm® sulphonylurea gliclazide Diamicron®, Merck-Gliclazide® glipizide Glibenese®, Minidiab® gliquidone Glurenorm® glibenclamide Bevoren®, Daonil®, Euglucon® gliclazide L.A. Uni diamicron® glimepiride Amarylle® glitazones pioglitazone Actos® rosiglitazone Avandia® glucosidase remmers acarbose Glucobay®

27
klasse generische naam producten biguaniden metformine Glucophage®, Metformax®, Merck-metformine® gliniden repaglinide NovoNorm® sulphonylurea gliclazide Diamicron®, Merck-Gliclazide® glipizide Glibenese®, Minidiab® gliquidone Glurenorm® glibenclamide Bevoren®, Daonil®, Euglucon® gliclazide L.A. Uni diamicron® glimepiride Amarylle® glitazones pioglitazone Actos® rosiglitazone Avandia® glucosidase remmers acarbose Glucobay®

28
klasse generische naam producten biguaniden metformine Glucophage®, Metformax®, Merck-metformine® gliniden repaglinide NovoNorm® sulphonylurea gliclazide Diamicron®, Merck-Gliclazide® glipizide Glibenese®, Minidiab® gliquidone Glurenorm® glibenclamide Bevoren®, Daonil®, Euglucon® gliclazide L.A. Uni diamicron® glimepiride Amarylle® glitazones pioglitazone Actos® rosiglitazone Avandia® glucosidase remmers acarbose Glucobay®

29
hoe keuze maken ? werkingskracht werkingsmechanisme gevaar voor hypo’s contraïndicaties tolerantie gebruiksgemak Leer met enkele producten werken !

30
+ sulfonylurea gliniden - glucosidaseremmers insuline glucose
biguaniden + glitazones glimepiride (Amaryl) : = langwerkend sulfonylureum (bindt op ander deel van SU-receptor ) => vooral maaltijd gerelateerde breektabl/ 2 mg : beginnen met ½/d, zo nodig tot 2/d (Z tot 3/d) onmiddellijk voor of tijdens ontbijt (30’ voor maaltijd nemen geen beter effect) max. effect pas na > 14d (zoals bij andere SU) geen ervaring met ernstige nier- of leverschade FI : andere prod. met eiwitbinding repaglinide (NovoNorm) : sluit ATP afhankelijke K-kanalen in de Mb van de beta-cel / doeleiwit verschillend van SU => depolarisatie => influx Ca => insulinesecretie voordelen : snelle resorptie => mag onm. voor mlt ingenomen worden T1/2 1u => weinig laattijdige hypo's, minder hyperinsulinisme (mogelijk beter voor complicaties) vooral hepatische klaring via CyP3A4 / < 8% renaal => mag gebruikt worden bij NI, niet bij LI start mg, max 4 mg bij elke mlt (tabl mg) FI : CyP3A4 remmers (azoles, erytro, mibefradil) / inductoren (rifampycine, fenytoine) ? combinatie met SU zinvol ? vrij duur glitazones : zwakke glycemie en 1/4 primair falen, G , TG HDL maar LDL , cave leverinsuff., bruikbaar bij NI duur ++ werkingsmechanisme (nog niet goed gekend) : PPAR activatie => lipolyse (vandaar G ) => FFA => hep.glucoseprod en gluc.verbruik spieren
 : = langwerkend sulfonylureum (bindt op ander deel van SU-receptor ) => vooral maaltijd gerelateerde breektabl/ 2 mg : beginnen met ½/d, zo nodig tot 2/d (Z tot 3/d) onmiddellijk voor of tijdens ontbijt (30’ voor maaltijd nemen geen beter effect) max. effect pas na > 14d (zoals bij andere SU) geen ervaring met ernstige nier- of leverschade. FI : andere prod. met eiwitbinding. repaglinide (NovoNorm) : sluit ATP afhankelijke K-kanalen in de Mb van de beta-cel / doeleiwit verschillend van SU. => depolarisatie => influx Ca => insulinesecretie. voordelen : snelle resorptie => mag onm. voor mlt ingenomen worden. T1/2 1u => weinig laattijdige hypo s, minder hyperinsulinisme (mogelijk beter voor complicaties) vooral hepatische klaring via CyP3A4 / < 8% renaal => mag gebruikt worden bij NI, niet bij LI. start mg, max 4 mg bij elke mlt (tabl mg) FI : CyP3A4 remmers (azoles, erytro, mibefradil) / inductoren (rifampycine, fenytoine) combinatie met SU zinvol vrij duur. glitazones : zwakke glycemie en 1/4 primair falen, G , TG HDL maar LDL , cave leverinsuff., bruikbaar bij NI duur ++ werkingsmechanisme (nog niet goed gekend) : PPAR activatie => lipolyse (vandaar G ) => FFA => hep.glucoseprod en gluc.verbruik spieren ")
31
+ sulfonylurea gliniden - glucosidaseremmers insuline glucose
hypo's ! insuline - glucosidaseremmers glucose biguaniden + glitazones glimepiride (Amaryl) : = langwerkend sulfonylureum (bindt op ander deel van SU-receptor ) => vooral maaltijd gerelateerde breektabl/ 2 mg : beginnen met ½/d, zo nodig tot 2/d (Z tot 3/d) onmiddellijk voor of tijdens ontbijt (30’ voor maaltijd nemen geen beter effect) max. effect pas na > 14d (zoals bij andere SU) geen ervaring met ernstige nier- of leverschade FI : andere prod. met eiwitbinding repaglinide (NovoNorm) : sluit ATP afhankelijke K-kanalen in de Mb van de beta-cel / doeleiwit verschillend van SU => depolarisatie => influx Ca => insulinesecretie voordelen : snelle resorptie => mag onm. voor mlt ingenomen worden T1/2 1u => weinig laattijdige hypo's, minder hyperinsulinisme (mogelijk beter voor complicaties) vooral hepatische klaring via CyP3A4 / < 8% renaal => mag gebruikt worden bij NI, niet bij LI start mg, max 4 mg bij elke mlt (tabl mg) FI : CyP3A4 remmers (azoles, erytro, mibefradil) / inductoren (rifampycine, fenytoine) ? combinatie met SU zinvol ? vrij duur glitazones : zwakke glycemie en 1/4 primair falen, G , TG HDL maar LDL , cave leverinsuff., bruikbaar bij NI duur ++ werkingsmechanisme (nog niet goed gekend) : PPAR activatie => lipolyse (vandaar G ) => FFA => hep.glucoseprod en gluc.verbruik spieren
 : = langwerkend sulfonylureum (bindt op ander deel van SU-receptor ) => vooral maaltijd gerelateerde breektabl/ 2 mg : beginnen met ½/d, zo nodig tot 2/d (Z tot 3/d) onmiddellijk voor of tijdens ontbijt (30’ voor maaltijd nemen geen beter effect) max. effect pas na > 14d (zoals bij andere SU) geen ervaring met ernstige nier- of leverschade. FI : andere prod. met eiwitbinding. repaglinide (NovoNorm) : sluit ATP afhankelijke K-kanalen in de Mb van de beta-cel / doeleiwit verschillend van SU. => depolarisatie => influx Ca => insulinesecretie. voordelen : snelle resorptie => mag onm. voor mlt ingenomen worden. T1/2 1u => weinig laattijdige hypo s, minder hyperinsulinisme (mogelijk beter voor complicaties) vooral hepatische klaring via CyP3A4 / < 8% renaal => mag gebruikt worden bij NI, niet bij LI. start mg, max 4 mg bij elke mlt (tabl mg) FI : CyP3A4 remmers (azoles, erytro, mibefradil) / inductoren (rifampycine, fenytoine) combinatie met SU zinvol vrij duur. glitazones : zwakke glycemie en 1/4 primair falen, G , TG HDL maar LDL , cave leverinsuff., bruikbaar bij NI duur ++ werkingsmechanisme (nog niet goed gekend) : PPAR activatie => lipolyse (vandaar G ) => FFA => hep.glucoseprod en gluc.verbruik spieren ")
32
+ sulfonylurea gliniden - glucosidaseremmers insuline glucose
biguaniden + glitazones glimepiride (Amaryl) : = langwerkend sulfonylureum (bindt op ander deel van SU-receptor ) => vooral maaltijd gerelateerde breektabl/ 2 mg : beginnen met ½/d, zo nodig tot 2/d (Z tot 3/d) onmiddellijk voor of tijdens ontbijt (30’ voor maaltijd nemen geen beter effect) max. effect pas na > 14d (zoals bij andere SU) geen ervaring met ernstige nier- of leverschade FI : andere prod. met eiwitbinding repaglinide (NovoNorm) : sluit ATP afhankelijke K-kanalen in de Mb van de beta-cel / doeleiwit verschillend van SU => depolarisatie => influx Ca => insulinesecretie voordelen : snelle resorptie => mag onm. voor mlt ingenomen worden T1/2 1u => weinig laattijdige hypo's, minder hyperinsulinisme (mogelijk beter voor complicaties) vooral hepatische klaring via CyP3A4 / < 8% renaal => mag gebruikt worden bij NI, niet bij LI start mg, max 4 mg bij elke mlt (tabl mg) FI : CyP3A4 remmers (azoles, erytro, mibefradil) / inductoren (rifampycine, fenytoine) ? combinatie met SU zinvol ? vrij duur glitazones : zwakke glycemie en 1/4 primair falen, G , TG HDL maar LDL , cave leverinsuff., bruikbaar bij NI duur ++ werkingsmechanisme (nog niet goed gekend) : PPAR activatie => lipolyse (vandaar G ) => FFA => hep.glucoseprod en gluc.verbruik spieren geen hypo's !
 : = langwerkend sulfonylureum (bindt op ander deel van SU-receptor ) => vooral maaltijd gerelateerde breektabl/ 2 mg : beginnen met ½/d, zo nodig tot 2/d (Z tot 3/d) onmiddellijk voor of tijdens ontbijt (30’ voor maaltijd nemen geen beter effect) max. effect pas na > 14d (zoals bij andere SU) geen ervaring met ernstige nier- of leverschade. FI : andere prod. met eiwitbinding. repaglinide (NovoNorm) : sluit ATP afhankelijke K-kanalen in de Mb van de beta-cel / doeleiwit verschillend van SU. => depolarisatie => influx Ca => insulinesecretie. voordelen : snelle resorptie => mag onm. voor mlt ingenomen worden. T1/2 1u => weinig laattijdige hypo s, minder hyperinsulinisme (mogelijk beter voor complicaties) vooral hepatische klaring via CyP3A4 / < 8% renaal => mag gebruikt worden bij NI, niet bij LI. start mg, max 4 mg bij elke mlt (tabl mg) FI : CyP3A4 remmers (azoles, erytro, mibefradil) / inductoren (rifampycine, fenytoine) combinatie met SU zinvol vrij duur. glitazones : zwakke glycemie en 1/4 primair falen, G , TG HDL maar LDL , cave leverinsuff., bruikbaar bij NI duur ++ werkingsmechanisme (nog niet goed gekend) : PPAR activatie => lipolyse (vandaar G ) => FFA => hep.glucoseprod en gluc.verbruik spieren geen hypo s !")
33
klasse generische naam producten biguaniden metformine Glucophage®, Metformax®, Merck-metformine® gliniden repaglinide NovoNorm® sulphonylurea gliclazide Diamicron®, Merck-Gliclazide® glipizide Glibenese®, Minidiab® gliquidone Glurenorm® glibenclamide Bevoren®, Daonil®, Euglucon® gliclazide L.A. Uni diamicron® glimepiride Amarylle® glitazones pioglitazone Actos® rosiglitazone Avandia® glucosidase remmers acarbose Glucobay®

34
metformine 1ste keuze, want geen hypo’s geen gewichtstoename
bewezen effect op harde eindpunten (evidence based medicine) bij obese (insuline resistente) patiënten gunstiger effect op cardiovasculaire outcome dan sulfonylurea of insuline (verbetering van het ‘metabool syndroom’)
 bij obese (insuline resistente) patiënten gunstiger effect op cardiovasculaire outcome dan sulfonylurea of insuline (verbetering van het ‘metabool syndroom’)")
35
metformine maar gastro-intestinale intolerantie (± 1 patiënt op 20) dosis niet te snel minder goede klaring van lactaat niet gebruiken in situaties die lactaatacidose kunnen veroorzaken - nierinsufficiëntie (creat > 1.5 mg/dl) - ernstige hartdecompensatie (rec. longoedeem) - ernstige COPD (rec. resp. insufficiëntie) - ernstig leverlijden (levercirrhose Child C) - stoppen avond voor chirurgische ingreep, iv. contrastonderzoek
 - ernstige hartdecompensatie (rec. longoedeem) - ernstige COPD (rec. resp. insufficiëntie) - ernstig leverlijden (levercirrhose Child C) - stoppen avond voor chirurgische ingreep, iv. contrastonderzoek.")
36
metformine : praktisch
eerste keuze (zeker bij obese patiënten) let op voor contraïndicaties (bij start, en tijdens R/) mag vroeg worden opgestart (geen hypoglycemie) lage startdosis, langzaam opdrijven (per wk) vb. Metformax 850 ½-0-0 ½-0-½ ½-½-½ 1-½-½ 1-½-1 1-1-1
 let op voor contraïndicaties (bij start, en tijdens R/) mag vroeg worden opgestart (geen hypoglycemie) lage startdosis, langzaam opdrijven (per wk) vb. Metformax 850 ½-0-0 ½-0-½ ½-½-½ 1-½-½ 1-½-1 ")
37
klasse generische naam producten biguaniden metformine Glucophage®, Metformax®, Merck-metformine® gliniden repaglinide NovoNorm® sulphonylurea gliclazide Diamicron®, Merck-Gliclazide® glipizide Glibenese®, Minidiab® gliquidone Glurenorm® glibenclamide Bevoren®, Daonil®, Euglucon® gliclazide L.A. Uni diamicron® glimepiride Amarylle® glitazones pioglitazone Actos® rosiglitazone Avandia® glucosidase remmers acarbose Glucobay®

38
insuline secretagogen : sulfonylurea, gliniden
2 de keuze, als metformine niet verdragen of gecontraïndiceerd bewezen gunstig effect op harde eindpunten (evidence based medicine)
")
39
sulfonylurea en gliniden : praktisch
niet te vroeg opstarten, want gevaar voor hypoglycemie keuze : - beginnende DM : kortwerkend product - gevorderde DM : langwerkend product - ingekrompen nierfunctie : Glurenorm®, Novonorm® lage startdosis, langzaam opdrijven vb. Gliclazide 0-0-½ … dagkurves nodig om dosis af te stellen

40
klasse generische naam producten biguaniden metformine Glucophage®, Metformax®, Merck-metformine® gliniden repaglinide NovoNorm® sulphonylurea gliclazide Diamicron®, Merck-Gliclazide® glipizide Glibenese®, Minidiab® gliquidone Glurenorm® glibenclamide Bevoren®, Daonil®, Euglucon® gliclazide L.A. Uni diamicron® glimepiride Amarylle® glitazones pioglitazone Actos® rosiglitazone Avandia® glucosidase remmers acarbose Glucobay®

41
glitazones veelbelovend want verbeteren het metabool syndroom
nog geen studies met harde eindpunten werken niet onmiddellijk (duurt enkele weken) veiligheid op lange termijn niet duidelijk : gewichtstoename, hartdecompensatie erg duur ( 15 x duurder dan metformine) enkel terugbetaald in combinatietherapie
 veiligheid op lange termijn niet duidelijk : gewichtstoename, hartdecompensatie. erg duur ( 15 x duurder dan metformine) enkel terugbetaald in combinatietherapie.")
42
glitazones praktisch indicaties :
metformine gecontraïndiceerd of niet verdragen HbA1c > 7.5 % onder max. dosis van een insuline secretagoog praktisch : terugbetaling aanvragen 1 x per dag verwacht geen onmiddellijk effect cave hartdecompensatie : volg gewicht, oedemen (patiënteducatie !!)
")
43
Progressive decline of -cell function in UKPDS
100 ? 80 60 -cell function (% ) 40 20 10 9 8 7 6 5 4 3 2 1 1 2 3 4 5 6 Years Adapted from UK Prospective Diabetes Study (UKPDS) Group. Diabetes 1995
 10. 9. 8. 7. 6. 5. 4. 3. 2. Years. Adapted from UK Prospective Diabetes Study (UKPDS) Group. Diabetes")
44
combinatietherapie : secretagoog + product dat gevoeligheid aan insuline verbetert
klasse generische naam producten biguaniden metformine Glucophage®, Metformax®, Merck-metformine® gliniden repaglinide NovoNorm® sulphonylurea gliclazide Diamicron®, Merck-Gliclazide® glipizide Glibenese®, Minidiab® gliquidone Glurenorm® glibenclamide Bevoren®, Daonil®, Euglucon® gliclazide L.A. Uni diamicron® glimepiride Amarylle® glitazones pioglitazone Actos® rosiglitazone Avandia®

45
combinatieproduct ? Glucovance® = glibenclamide 2.5 / 5 + metformine 500 mg bij beginnende DM2 om meteen de 2 defecten (insuline resistentie, verminderde ß-celfunctie) aan te pakken ? meer kans op hypoglycemie dan bij metformine monotherapie bij gevorderde DM2 om de therapietrouw te verbeteren ? kan ook bij combinatie van langwerkend SU en metformine : - Glucovance 5/500 mg : Amarylle 4 mg en Glucophage 850 mg 1-0-1 als je het gebruikt : ken de samenstelling
 aan te pakken meer kans op hypoglycemie dan bij metformine monotherapie. bij gevorderde DM2 om de therapietrouw te verbeteren kan ook bij combinatie van langwerkend SU en metformine : - Glucovance 5/500 mg : Amarylle 4 mg en Glucophage 850 mg als je het gebruikt : ken de samenstelling.")
46
oefening

47
casus patiënt met pas ontdekte DM2 HbA1c 9 % creat 0.9 mg/dl
welke therapie ? hoe opbouwen ? wat als patiënt metformine niet verdraagt ? wat als creat 2.3 mg/dl ?

48
casus patiënt met DM2 HbA1c 8.3 % creat 0.9 mg/dl
huidige behandeling : metformine 850 mg 1-0-1 welke aanpassing ? hoe opbouwen ?

49
casus patiënt met DM2 HbA1c 8.3 % creat 1.8 mg/dl
huidige behandeling : gliclazide 80 mg 1-0-2 welke aanpassing ? hoe opbouwen ? wat als patiënt bekend is met hartdecompensatie ?

Verwante presentaties








>")










