Download de presentatie
De presentatie wordt gedownload. Even geduld aub

1
Community acquired pneumonia CAP

2
3 vragen Wat is CAP? Wat doet NICE?
Waarom verteld het Havenziekenhuis iets daarover?

3
CAP Definitie CAP wordt gedefinieerd als een acute infectie van het longparenchym CAP ontstaat buiten het ziekenhuis en kan zich openbaren tot 72 uur na ziekenhuisopname. (NVALT Richtlijn Community Acquired pneumonia )
")
4
Symptomen CAP gaat gepaard met tenminste één van de volgende symptomen: Koorts, hoesten met of zonder sputumproductie en/of Verscherpt ademgeruis met of zonder crepiteren over de longen, pleurapijn, verwardheid en leukocytose boven 12 x 109/l Nieuwe afwijkingen op de thoraxfoto zijn obligaat. (NVALT Richtlijn Community Acquired pneumonia )
")
5
PSI score: pneumonie severity index Stap1
Leeftijd > 50 jaar Zijn er onderliggende ziekten aanwezig als: Maligniteit, Hartfalen, Cerebrovasculaire ziekten, Nierziekten, Leverziekten Of Zijn afwijkingen bij lichamelijk onderzoek aanwezig als: Veranderd bewustzijn, Polsfrequentie >125/ min, Ademfrequentie >30/ min, Systolische bloeddruk <90 mm Hg, Temperatuur <35ºC of > 40 ºC => Patiënt wordt ingedeeld in risicoklasse 2-5 afhankelijk van de score bij stap 2

6
PSI-score - Stap 2 Klasse 1 0,1 % Klasse 2 <70 punten (0,6%)
Man Leeftijd (jaren) in punten Vrouw Verpleeghuisbewoner +10 Maligniteit +30 Leverziekte +20 Hartfalen Cerebrovasculaire ziekte Nierziekte Verwardheid Ademfrequentie >30/ min. Systolische bloeddruk < 90 mm Hg Temperatuur < 35 ºC of > 40 ºC +15 Polsfrequentie >125 / min. Arteriële pH <7,35 Ureum >11,0 mmol/l Na <130 mmol/l Glucose >14,0 mmol/l Ht < 30% PaO2 < 60 mm Hg Pleuravocht Totaal * PSI-score - Stap 2 Klasse 1 0,1 % Klasse 2 <70 punten (0,6%) Klasse 3 71-90 punten (0,9%) Klasse 4 punten (9,3%) Klasse 5 Ernstige pneumonie >130 punten (27%mortaliteit)
 in punten. Vrouw. Verpleeghuisbewoner Maligniteit Leverziekte Hartfalen. Cerebrovasculaire ziekte. Nierziekte. Verwardheid. Ademfrequentie >30/ min. Systolische bloeddruk < 90 mm Hg. Temperatuur < 35 ºC of > 40 ºC Polsfrequentie >125 / min. Arteriële pH <7,35. Ureum >11,0 mmol/l. Na <130 mmol/l. Glucose >14,0 mmol/l. Ht < 30% PaO2 < 60 mm Hg. Pleuravocht. Totaal * PSI-score - Stap 2. Klasse 1. 0,1 % Klasse 2. <70 punten (0,6%) Klasse punten (0,9%) Klasse punten (9,3%) Klasse 5. Ernstige pneumonie. >130 punten (27%mortaliteit)")
7
Verwekker Streptococcus pneumoniae (30%) Haemophilus influenza (6%)
Mycoplasma pneumoniae (6%) Influenza A/B, parainfluenza Legionella spp, Staphylococcus aureus, Chlamydophila pneumoniae / psittaci, Mycobacterium Tuberculosis 40% - 50% onbekend
 Influenza A/B, parainfluenza. Legionella spp, Staphylococcus aureus, Chlamydophila pneumoniae / psittaci, Mycobacterium Tuberculosis. 40% - 50% onbekend.")
8
Bijzonderheden H1N1-Pneumonie
64% van die in het Ziekenhuis opgenomen patiënten ontwikkelen noodzaak voor machinale beademing 5 keer verhoogd risico om een severe ARDS te ontwikkelen 12% behandelt met ECMO 14% overlijden Infiltraten verbeteren laat > 10 dagen

9
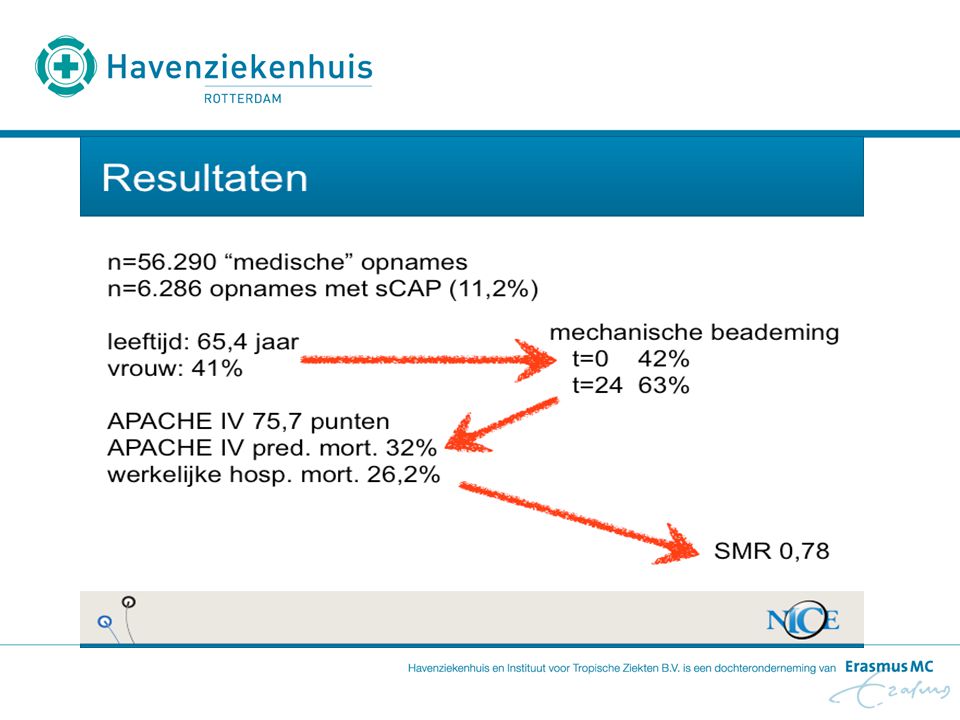
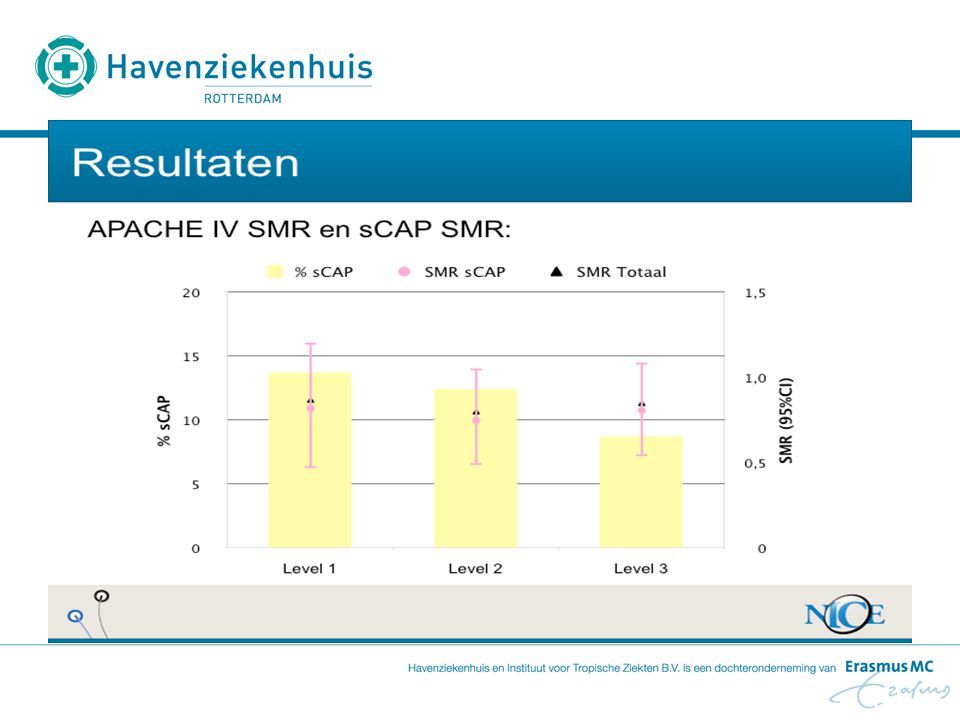
NICE SMR= standard mortality ratio Thema discussie bijeenkomst 2010:
CAP en Mortaliteit

12
Havenziekenhuis Volgens NICE
Is een klein algemeen ziekenhuis gespecialiseerd in Tropengeneeskunde en Reizigersziekte en Ouderengeneeskunde. Kleine level 1 IC met 3 beademingsbedden Afdelingen Longgeneeskunde, Interne Geneeskunde,Geriatrie, Chirurgie Op IC veel patiënten met exacerbatie COPD, pneumonie, pneumosepsis, urosepsis Volgens NICE is het Havenziekenhuis een van de drie ziekenhuizen in heel Nederland met de laagste mortaliteit bij behandeling van CAP

13
Overeenkomsten bij de drie best scorende intensive care afdelingen waren:
Antibioticatherapie (dubbeltherapie, vroegtijdig toedienen) Restrictief vochtbeleid (gebruik Pulmonaliskatheter) Beademen met 6ml/kg/ILG Laagdrempelige opname IC Patiënten niet te vroeg ontslag naar verpleegafdeling
 Restrictief vochtbeleid (gebruik Pulmonaliskatheter) Beademen met 6ml/kg/ILG. Laagdrempelige opname IC. Patiënten niet te vroeg ontslag naar verpleegafdeling.")
14
Behandeling in de praktijk
Hoe doen wij dat in de praktijk, wat ook overeen komt met de drie beste IC’s

15
Veel aandacht voor vroegtijdig toedienen Antibiotica (op verpleegafdeling/SEH/IC)
Binnen eerste 1-(2) uur! Gewaarborgd middels checklijsten: CAP protocol (SEH) Protocol ernstige sepsis (ziekenhuisbreed) Voordeel door onze werkstructuur Korte lijnen Intensivist/IC-team is betrokken op SEH/verpleegafdelingen Intensivist aanwezig bij interne overdracht Werken met niet-intensivist-specialisten op IC (wv 1xlongarts, 1xinfectioloog)
 uur! Gewaarborgd middels checklijsten: CAP protocol (SEH) Protocol ernstige sepsis (ziekenhuisbreed) Voordeel door onze werkstructuur. Korte lijnen. Intensivist/IC-team is betrokken op SEH/verpleegafdelingen. Intensivist aanwezig bij interne overdracht. Werken met niet-intensivist-specialisten op IC (wv 1xlongarts, 1xinfectioloog)")
16
Cumulative effective antimicrobial initiation following onset of septic shock-associated hypotension and associated survival (Kumar et al, CCM 2006) Figure 1. Cumulative effective antimicrobial initiation following onset of septic shock-associated hypotension and associated survival. The x-axis represents time (hrs) following first documentation of septic shock-associated hypotension. Black bars represent the fraction of patients surviving to hospital discharge for effective therapy initiated within the given time interval. The gray bars represent the cumulative fraction of patients having received effective antimicrobials at any given time point.
 Figure 1. Cumulative effective antimicrobial initiation following onset of septic shock-associated hypotension and associated survival. The x-axis represents time (hrs) following first documentation of septic shock-associated hypotension. Black bars represent the fraction of patients surviving to hospital discharge for effective therapy initiated within the given time interval. The gray bars represent the cumulative fraction of patients having received effective antimicrobials at any given time point.")
17
Het risico op overlijden stijgt continue om 7% per uur
bij uitstellen van het toedienen van effectieve antibiotica

18
Antibiotica ernstige CAP
Amoxicilline/Clavulaanzuur + Ciprofloxacine of Levofloxacine (SWAB richtlijn thuis opgelopen pneumonie 2005)
")
19
Non invasieve beademing
NIV

20
NIV Indicaties Hyperkapnische acute respiratoire insufficiëntie:
Exacerbatie COPD Hypoxemische acute respiratoire insufficiëntie: Cardiogeen longoedeem Immunsupprimmeerde patiënten

21
NIV Contra-indicaties Afwezige spontane ademhaling
Verlaagd bewustzijn met kans op aspiratie Ileus, gastrointestinale bloeding pH < 7,2

22
CAP en NIV Patiënten met COPD en pneumonie profiteren van NIV door
Minder aantal intubaties Verkorting van de IC-ligduur (Confalionieri et al, 2005) Bij succes van NIV is letaliteit laag, bij noodzaak voor intubatie hoog (Jolliet et al, 2001)
 Bij succes van NIV is letaliteit laag, bij noodzaak voor intubatie hoog. (Jolliet et al, 2001)")
23
Falen van NIV (Antonelli 2001)
Fig. 2. Causes of acute respiratory failure and frequency of NPPV failure. CPE cardiogenic pulmonary edema, Pulm Cont pulmonary contusion, Inh PN inhalation pneumonia, Atelect atelectasis, NP nosocomial pneumonia, ARDSp pulmonary acute respiratory distress syndrome, CAP community-acquired pneumonia, ARDSexp extrapulmonary acute respiratory distress syndrome, Pulm Fibr/PE pulmonary fibrosis or pulmonary embolism. Causes of extra-pulmonary ARDS are listed for groups that required and avoided intubation, respectively: abdominal sepsis and pancreatitis 11 and 12; post-surgical sepsis 15 and 3; transfusion of more than 6 units of blood within the previous 24 h of ICU admission 6 and 11; and fat embolism 0 and 1. For each subgroup, the column represents the number of patients, the dot represents the percentages of patients requiring intubation, and the line represents the 95% confidence intervals

24
Aandachtspunten Poging NIV bij patiënten met COPD
NIV niet te lang proberen als niet succesvol Maximaal 2,5 uur!

25
Falen NIV Optiflow zuurstofverneveling INTUBATIE
(high flow zuurstoftherapie) INTUBATIE met hoge zuurstofbehoefte, met slechte acceptatie van een masker mislukte NIV-poging, ontwennen van NIV met lastig secretie managment
 INTUBATIE. met hoge zuurstofbehoefte, met slechte acceptatie van een masker. mislukte NIV-poging, ontwennen van NIV. met lastig secretie managment.")
26
Invasieve beademing Longprotectief beademen:
Lage tidal volumes 6ml/kg/ILG Adequate PEEP Pmax <35mbar

27
Wat ik verder moet doen Let op het vloeistofbeleid
Maak gebruik hemodynamisch monitoring Hoofdeinde bed altijd >30-45 graden omhoog

28
Wat kan ik verder op een level 1 IC doen?
Wisselligging/Buikligging Geactiveerd proteïne C (Xigris) (Beta-Agonisten=Salmeterol)
 (Beta-Agonisten=Salmeterol)")
29
Verdere behandelingopties bij patiënten met ALI/ARDS
ECMO HFO-beademing Surfactant NO-beademing (Beta-Agonisten) Buikligging Voorbehouden hoger level IC
 Buikligging. Voorbehouden hoger level IC.")
30
Take home message I Antibiotica zo vroeg als mogelijk toedienen
Restrictief vloeistofbeleid Poging NIV Longprotectief beademen (6ml/kg/LG)
")
31
Take home message II Bewaak de tijd (tijd is outcome!)
Gebruik checklijsten (bundels) Blijf kritisch: weet je echt wat je doet of denk je alleen wat je aan het doen bent?
 Blijf kritisch: weet je echt wat je doet of denk je alleen wat je aan het doen bent")
32
Bedankt voor uw aandacht!

Verwante presentaties









 Belangenverstrengeling Geen>")




>")




