Download de presentatie
De presentatie wordt gedownload. Even geduld aub

1
Bedside integrated care plans using wireless technology Dr. Tom Fiers, Christophe Jolie, Dirk Lemaitre

2
Integrated care plans Collection of all planned activities for a patient Visualized over a given time span Integrated means: Ordercommunication Nursing orders Medical orders Paramedical orders Medication Problems, Goals Observations A fully functional EPR is needed … Bedside access is needed …

3
Integrated care plans Objectives for the patient: Provide a high standard of care Objectives for the hospital Better visualisation of the care process Data availability & presence Better multidisciplinary care Better traceability Lowering administrative workload (eg MVG, MKG)
")
4
Observations Problems & Goals Integrated Care Plans EPR nursing orders Orders medication consultations Progress charting Integrated care plans

5
EPR & ordercommunication layers since 1996 Clinical pathways in preparation since 2001 Hospitalwide gathering and structuring of all existing procedures Multidisciplinary workgroups Creation of ordersets and multidisciplinary careplans Definition of observations, progress charting, problems & outcomes Creation specific for department, pathology or even physician in charge Design & implementation

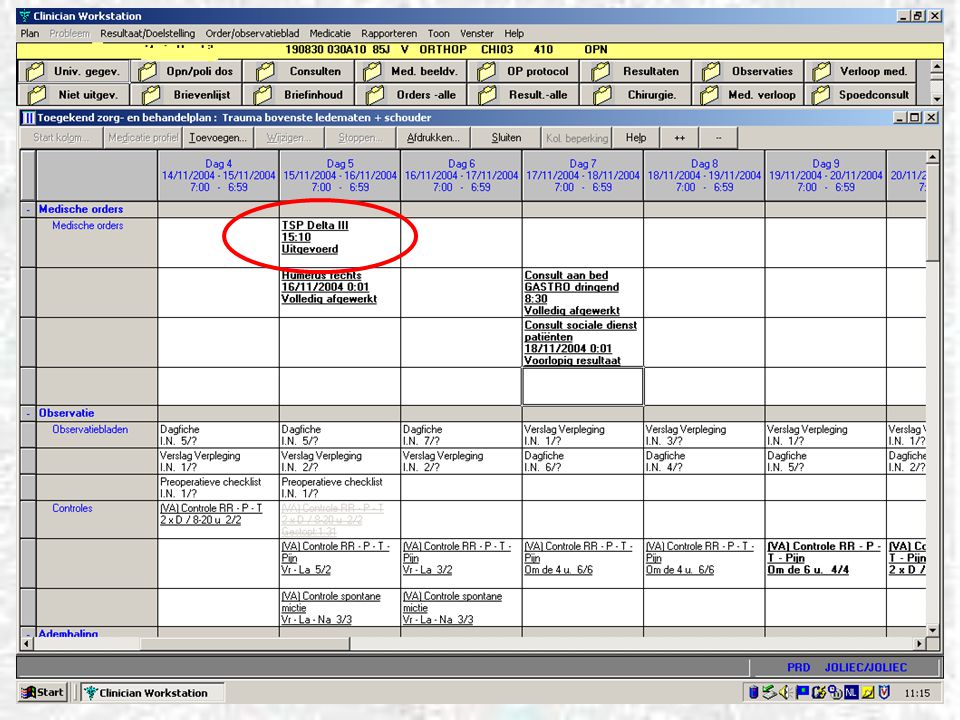
7
Medical orders: eg. operation

10
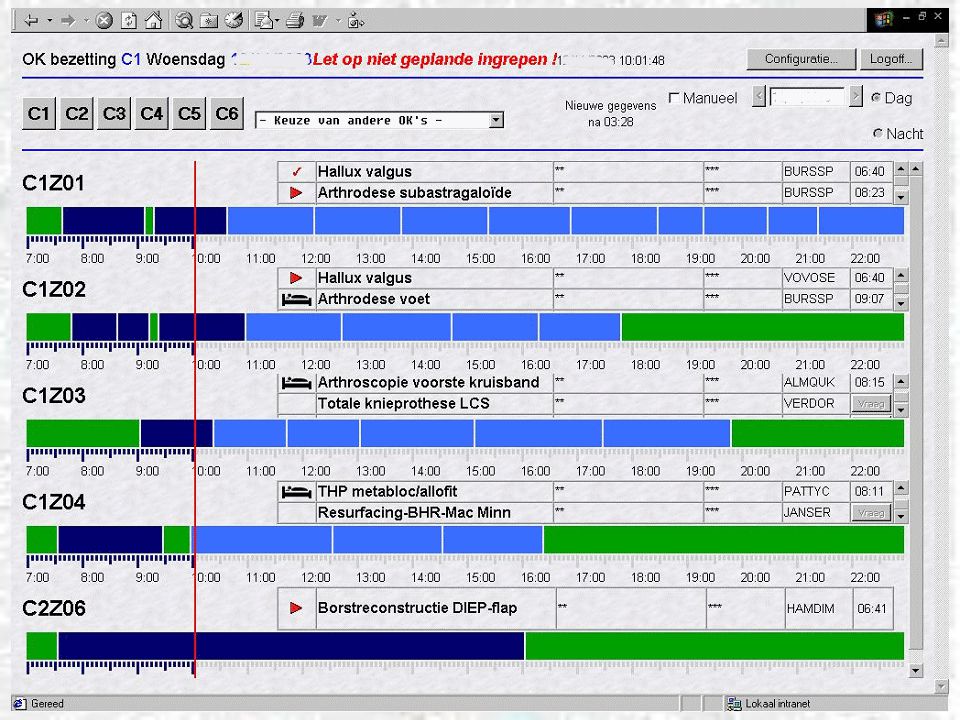
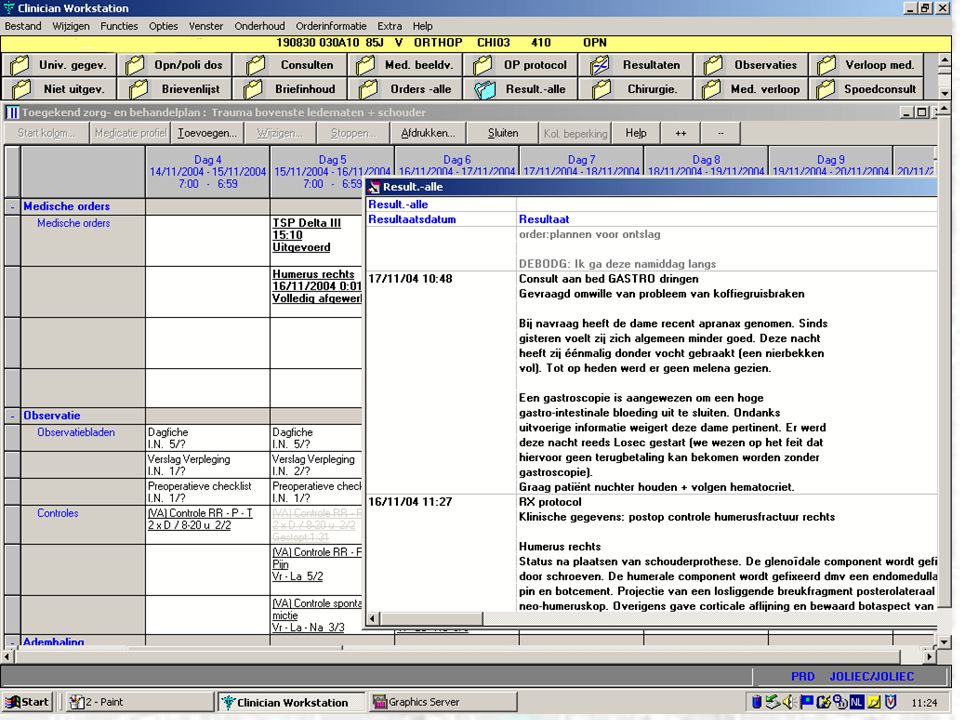
Consulting orders – worklists

14
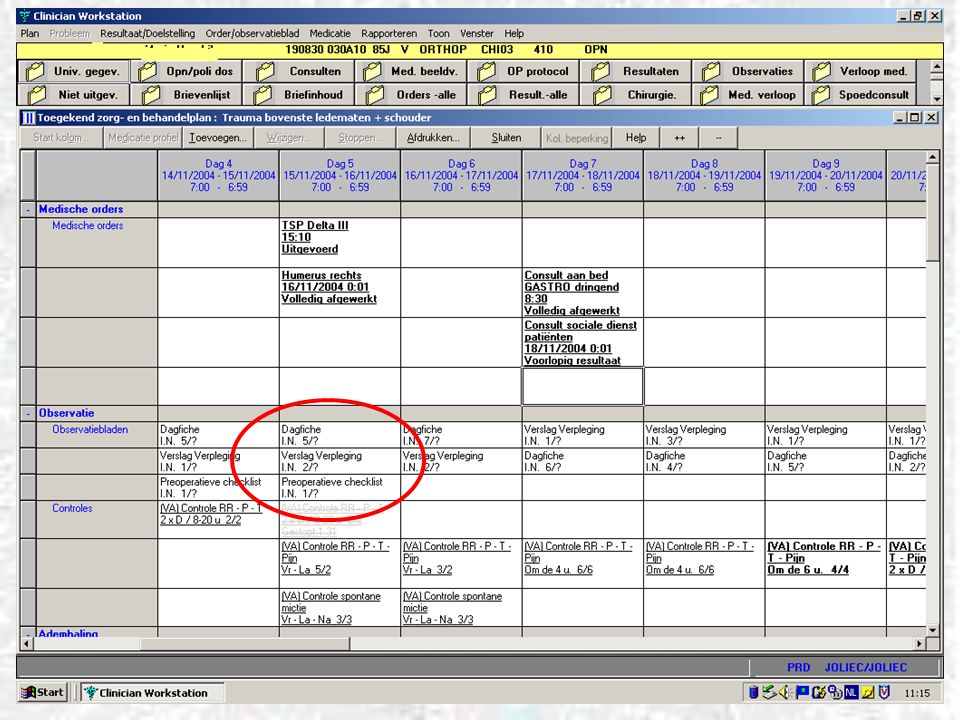
Observations

15
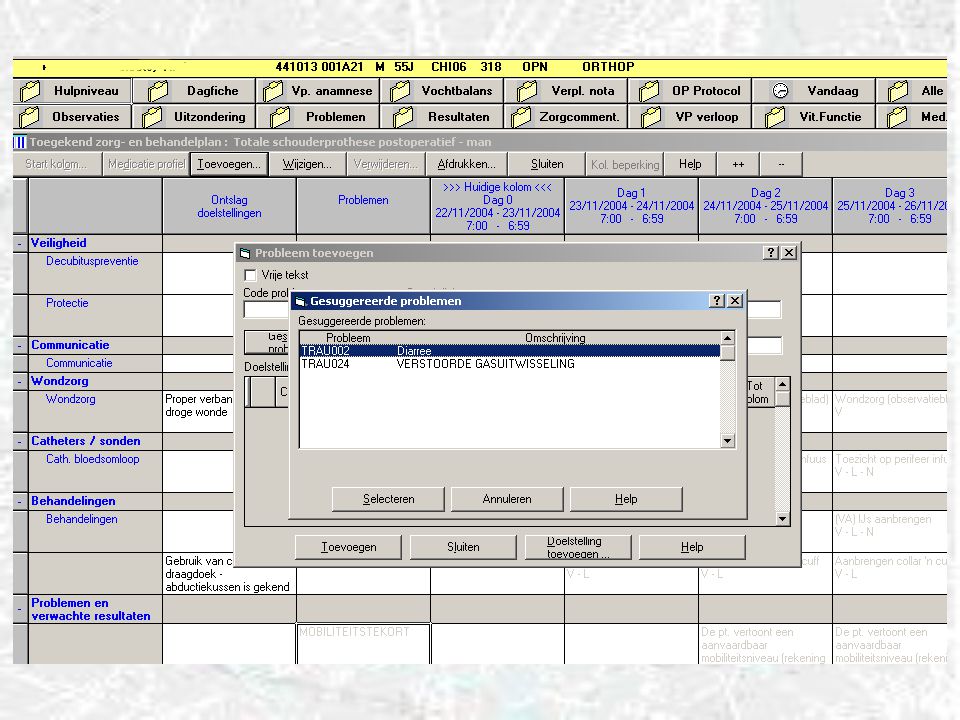
Problems & Objectives Observation (assessment) e.g. patient is agitated Nursing problem e.g. risk for acute disorientation Goal Prevent disorientation Orders e.g. reality orientation Nurse Observes and reports The SOFTWARE warns for possible problems and suggests the appropriate actions in order to prevent these Observation (assessment) e.g. patient is agitated
 e.g. patient is agitated.")
17
Problems & Objectives Observation (assessment) e.g. patient is agitated Nursing problem e.g. risk for acute disorientation Goal Prevent disorientation Orders e.g. reality orientation Nurse Observes and reports The SOFTWARE warns for possible problems and suggests the appropriate actions in order to prevent these Nursing problem e.g. risk for acute disorientation

19
Problems & Objectives Observation (assessment) e.g. patient is agitated Nursing problem e.g. risk for acute disorientation Goal Prevent disorientation Orders e.g. reality orientation Nurse Observes and reports The SOFTWARE warns for possible problems and suggests the appropriate actions in order to prevent these Orders e.g. reality orientation Goal Prevent disorientation

20
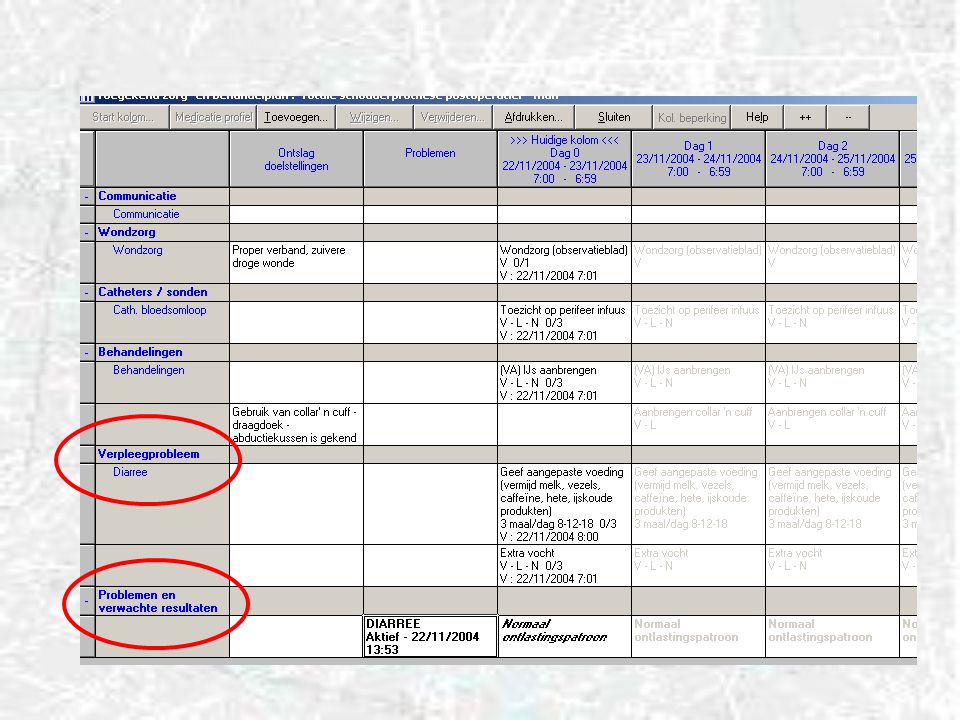
Problems & Objectives

22
Objectives achieved

23
Care plan merging

24
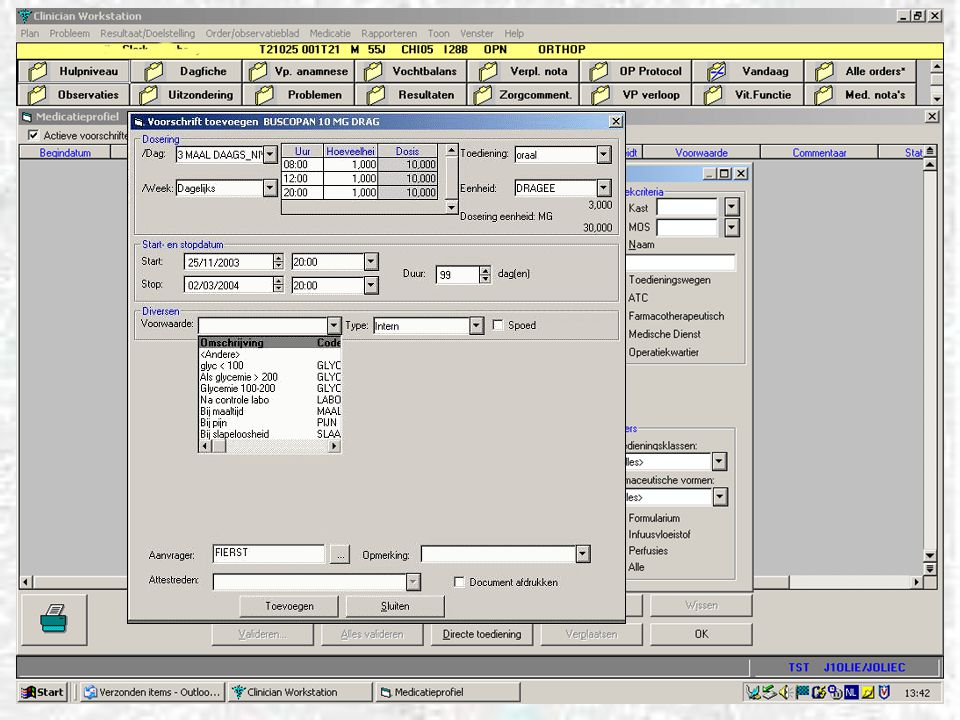
medic1

25
medic2

27
medic3

28
MVG & zorgzwaarte Codering mogelijk van: observaties problemen & doelstellingen verpleegorders medicatie

29
MVG & zorgzwaarte Item 1: zorgen aan patiënt met tracheacanule of endotracheale tube Item 2: zorgen mbt voeding en hydratatie per os Item 3: Sondevoeding Item 4: Zorgen mbt urinaire en/of faecale uitscheiding Item 5: Zorgen mbt hygiëne Item 6: Hulp bij dagkleding Item 7: Bijzondere mondzorg Item 8: Zorgen mbt mobiliteit Item 9: Decubituspreventie dmv wisselhouding Item 10: Zorg aan de gedesoriënteerde patiënt Item 11: Afzonderingsmaatregelen ter preventie van contaminatie Item 12: Verpleegkundig anamneseverslag Item 13: Zelfstandigheidstraining Item 14: Opvang emotionele crisis Item 15: Registratie vitale parameters Item 16: Registratie fysische parameters Item 17: Afnemen van bloedstaal Item 18: toezicht op tractie, gipsverband of externe fixator Item 19: Toediening van medicatie IM - SC - ID Item 20: Toediening van medicatie IV Item 21: Toezicht op IV infuus Item 22: Zorgen aan een chirurgische wonde Item 23: Zorgen aan een traumatische wonde UZ Gent EPR

30
Traumatologie : gedefinieerde klinische paden TRA001 Overname IZ TRA002 plan besmet materiaal BL conservatief TRA003 plan besmet materiaal OL operatief; pre- en postop. samen, TRA004 plan BHP; pre- en postop. Samen TRA005 plan heupprothese resurfacing; pre- en postop. Samen TRA006 plan korte opname knieletsel; pre- en postop. Samen TRA007 plan microchirurgie TRA008 plan tibia - fibula - voet spoedopname TRA009 plan trauma bekken lardinois spoedopname TRA010 plan trauma CWZ spoedopname TRA011 plan trauma femur spoedopname TRA012 Schouderprothese; pre- en postop. samen TRA013 Knieprothese; pre- en postop. Samen TRA014 Heupprothese; TRA015 plan besmet materiaal OL conservatief TRA016 plan besmet materiaal BL operatief; pre- en postop. Samen TRA017 plan revisie heupprothese spoedopname; TRA018 plan trauma bekken spoedopname; TRA019 plan trauma LWZ-TWZ spoedopname;

31
Pilot ward: Traumatology Pilot 3/2004 – 7/2004 Phased production startup on 6 beds Objectives Evaluate the training & workbooks Evaluate the WLAN bedside environment Validation of the software: ‘Nurseproof’ User-friendliness Feasibility Improvements to be made Improvements made 7-9/2004 Full ward in production since 10/2004

32
Set up Resource intensive process: 10 month pathway /ward Human resources: Standards coordinator, care plan coordinators & taskforce Care providers: Physicians, Nurses, Paramedical,… Helpdesk 7/7, 7-10pm + emergency support Eight to twelve hours of training / user Temporary extra staffing Bedside support IT: 5 portables on carts 2 portables on standards 3 fixed PC’s Setting up a WLAN

33
Wireless LAN in the hospital Options: DECT, 802.11 Problems: no open air, but: Concrete, elevator shafts, steel, isolation chambers, heavy equipment Importance of: Range Interference Security Cost

34
WLAN: Option 1: Data over DECT DECT: Digital Enhanced Cordless Telecommunications Plus: Network already installed (price), range Experiences: Acceptable speed using (expensive) Citrix metaframe Graphics intensive applications too slow Lots of initial small tweaking necessary to the DECT network Competition between voice & data channels Some unforseen roaming problems eg elevators Connection loss, about 2x/day
, range Experiences: Acceptable speed using (expensive) Citrix metaframe Graphics intensive applications too slow Lots of initial small tweaking necessary to the DECT network Competition between voice & data channels Some unforseen roaming problems eg elevators Connection loss, about 2x/day")
35
WLAN Option 2: 802.11 IEEE, 1999, Institute of Electrical and Electronics Engineers Suite of multiple standards: a,b,g,i,n,… 802.11a: 5Ghz, 54Mbps, small range 802.11b: 2.4Ghz, 11Mbps, acceptable range 802.11g: 2.4Ghz, 20+Mbps 802.11i: extra security (802.11n: higher throughput) WiFi alliance: interoperability Popular, giant installed user base Higher throughput: ok for graphics
 WiFi alliance: interoperability Popular, giant installed user base Higher throughput: ok for graphics")
36
802.11b/g Throughput decreases rapidly with range 150m theoretical, 10-15m in reality… 3-4 Antennas necessary / ward -> cost is an issue

37
802.11b/g Europe 13 channels, only 3 usable without interference at the same time Difficult to cover a hospital: 3D puzzle… 2.4Ghz range, channels 1-13

38
802.11b/g Needed in a hospital environment: Variable antenna strength Continuous broadcast (roaming) No router functionalities (roaming) Some tweaking necessary: Roaming switching vs available antennas Some packet patterns can disrupt connection Overall stable connections
 No router functionalities (roaming) Some tweaking necessary: Roaming switching vs available antennas Some packet patterns can disrupt connection Overall stable connections")
39
802.11 Security Hiding SSID Hiding Network identification MAC adress filtering WEP encryption (wired equivalent privacy) Static key Almost impossible to maintain in a large organization All in all not very secure… (<2 hours needed)
 Static key Almost impossible to maintain in a large organization All in all not very secure… (<2 hours needed)")
40
802.11 Security Better: WPA Wi-Fi Protected Access Parts of 802.11i standard Each packet uniquely encrypted (RC4) Ever changing key Strong authentication (802.1x) RADIUS server needed (Remote Authentication Dial-In User Service). Best: WPA2 (Wi-Fi Protected Access 2™) Full 802.11i compliancy WPA Compatible AES encryption (Advanced Encryption Standard), Rijndael algorithm, Joan Daemen and Vincent Rijmen Sept. 2004 Added security: Firewall between WLAN and LAN
 Full i compliancy WPA Compatible AES encryption (Advanced Encryption Standard), Rijndael algorithm, Joan Daemen and Vincent Rijmen Sept Added security: Firewall between WLAN and LAN.")
41
Status Stable 802.11b/g based WLAN Satisfying production results & user feedback Roll-out on thoracovascular surgery and plastic surgery 7th december Roll-out on revalidation dept. In february Roll-out planned on 3 further wards in 2005 2 internal medicine (>> problems & outcomes) 2 surgery (>> standard care plans)
 2 surgery (>> standard care plans).")
42
Conclusions Integrated care is about people, not technology The crucial importance of extensive preparation, training, on- site help and round the clock helpdesk support by people who understand the hospital are not to be underestimated EPR & WLAN technology have matured sufficiently to warrant paperless bedside integrated care implementations

Verwante presentaties







![Deltion College Engels C1 Spreken [Edu/003] thema “Oprah at Deltion” can-do : kan duidelijke, gedetailleerde beschrijving geven van complexe onderwerpen,](/8/2033280/big_thumb.jpg "Deltion College Engels C1 Spreken [Edu/003] thema “Oprah at Deltion” can-do : kan duidelijke, gedetailleerde beschrijving geven van complexe onderwerpen,>")







 Current Baseline (Version 6 – 27 Sept ’02) Endcap A/C.>")






