Download de presentatie
De presentatie wordt gedownload. Even geduld aub

1
Dr Johan Boie ……………………………………….
COPD update behandeling

4
COPD prevalentie en complicaties
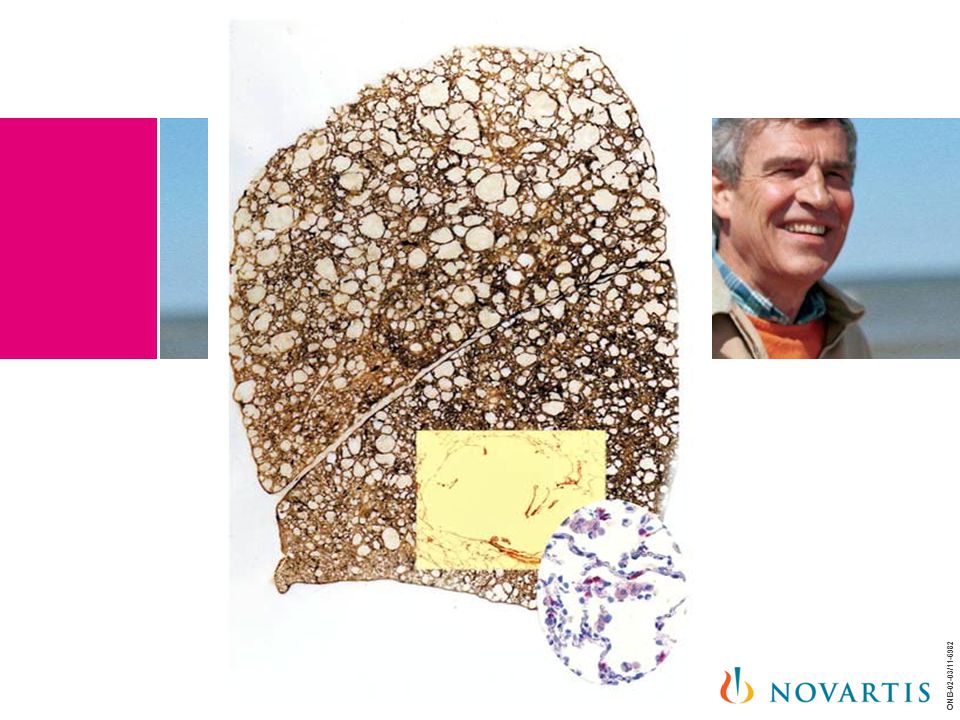
Chronisch obstructieve longziekten (COPD) vormen wereldwijd een belangrijke en toenemende oorzaak van morbiditeit en mortaliteit. Naast de langzaam progressieve luchtwegvernauwing dragen extrapulmonale manifestaties in belangrijke mate bij aan de klachten en ziektelast bij COPD. Sigarettenrook zelf, de belangrijkste oorzaak van vermijdbare mortaliteit in de westerse wereld, is gerelateerd aan een breed spectrum van rookgerelateerde aandoeningen. prof. dr. W. Janssens, dienst IG pneumologie, UZ Leuven campus Gasthuisberg
 vormen wereldwijd een belangrijke en toenemende oorzaak van morbiditeit en mortaliteit. Naast de langzaam progressieve luchtwegvernauwing dragen extrapulmonale manifestaties in belangrijke mate bij aan de klachten en ziektelast bij COPD. Sigarettenrook zelf, de belangrijkste oorzaak van vermijdbare mortaliteit in de westerse wereld, is gerelateerd aan een breed spectrum van rookgerelateerde aandoeningen. prof. dr. W. Janssens, dienst IG pneumologie, UZ Leuven campus Gasthuisberg.")
5
COPD complicaties Veranderingen in lichaamssamenstelling, zowel een afname in spiermassa (cachexie) als een toename in vetmassa (obesitas) zijn vaak geassocieerd aan COPD. Het risico op osteoporose is ook duidelijk verhoogd bij COPD. Hart- en vaatziekten zijn samen met longkanker verantwoordelijk voor een groot percentage sterfgevallen bij COPD: elke 10% afname in de 1-secondewaarde verhoogt de kans op cardiovasculaire mortaliteit met 28%. De pathogenese van deze extrapulmonale verwikkelingen is multifactorieel en de rol van systemische inflammatoire processen wordt uitgebreid bestudeerd. Diagnostiek en behandeling van deze extrapulmonale verschijnselen vormen een belangrijk onderdeel van een geïntegreerd zorgprogramma voor COPD-patiënten. Pentalfa”- project georganiseerd door de Faculteit Geneeskunde, K.U.Leuven (http: //
 als een toename in vetmassa (obesitas) zijn vaak geassocieerd aan COPD. Het risico op osteoporose is ook duidelijk verhoogd bij COPD. Hart- en vaatziekten zijn samen met longkanker verantwoordelijk voor een groot percentage sterfgevallen bij COPD: elke 10% afname in de 1-secondewaarde verhoogt de kans op cardiovasculaire mortaliteit met 28%. De pathogenese van deze extrapulmonale verwikkelingen is multifactorieel en de rol van systemische inflammatoire processen wordt uitgebreid bestudeerd. Diagnostiek en behandeling van deze extrapulmonale verschijnselen vormen een belangrijk onderdeel van een geïntegreerd zorgprogramma voor COPD-patiënten. Pentalfa - project georganiseerd door de Faculteit Geneeskunde, K.U.Leuven (http: //")
6
COPD MORBIDITEIT EN MORTALITEIT Berekeningen van de Wereldgezondheidsorganisatie (WHO) voorspellen dat COPD in het jaar 2020 wereldwijd de derde belangrijkste doodsoorzaak wordt en de vijfde oorzaak van morbiditeit. Nieuwe epidemiologische studies tonen bovendien duidelijk aan dat de prevalentie van matig COPD veel hoger moet geschat worden dan vroeger aanvaard werd

7
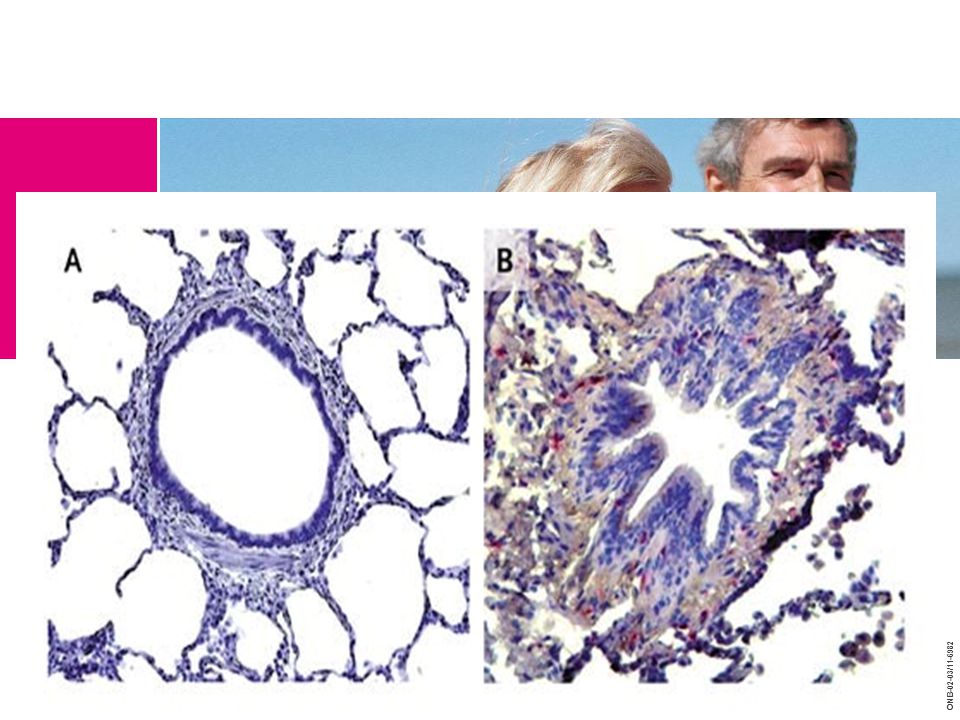
IMMUNOLOGIE VAN EERSTE STADIUM SIGARETTENROOKCONTACT Cigarette smoke injures epithelial cells, which release “danger signals” that act as ligands for toll-like receptors (TLRs) in the epithelium. These actions trigger the production of chemokines and cytokines, which results in an innate inflammation. Products from the inflammatory cells may injure the extracellular matrix, leading to the release of TLR ligands and consequent TLR activation, which will promote further inflammation, tissue injury, and the production of antigenic substances. This chain of events may cause dendritic cells to mature and migrate to local lymph organs, where, if the conditions are favorable, T-cell activation may result, with progression of the disease. If the innate inflammation in step 1 is minimized or controlled, the inflammation will not progress to adaptive immunity, and the disease may be arrested. These processes are typical of smokers who have neither COPD nor Gold stage 1. GM-CSF denotes granulocyte–macrophage colony-stimulating factor, HSP heat-shock protein, ICAM-1 intercellular adhesion molecule 1, MCP-1 monocyte chemoattractant protein 1, and TNF tumor necrosis factor. Manuel G. Cosio, M.D., Marina Saetta, M.D., and Alvar Agusti, M.D. N Engl J Med 2009; 360: June 4, 2009

8
Denken aan COPD Indacaterol (Onbrez®): structuur, overzicht van de klinische gegevens, praktische aspecten Bespreking: Onbrez® voor welke patiënten?
: structuur, overzicht van de klinische gegevens, praktische aspecten Bespreking: Onbrez® voor welke patiënten")
9
680.000 gevallen in België 50% gediagnosticeerd
Prevalentie ~6% Maximale schatting van het aantal gevallen van COPD Gediagnosticeerd en behandeld COPD Cegedim Strategic Data

10
Denken aan COPD ≥40 jaar + tabagisme
Bevestiging van de diagnose met spirometrie Vermindering van de risicofactoren Behandeling met bronchodilatatoren ≥40 jaar + tabagisme Kortademigheid Productieve hoest Verminderde activiteit Aangetaste slaapkwaliteit Verminderde levenskwaliteit Comorbiditeit Denken aan COPD

11
Normaal spirogram en spirogram bij een matig ernstig COPD
Spirometrie Normaal spirogram en spirogram bij een matig ernstig COPD Normaal spirogram en spirogram van matige COPD ESW FVC ESW/FVC Normaal CPOD ESW CPOD FVC ESW Normaal FVC Liter Seconden GOLD guidelines.

12
Patiënten vermijden dyspnoe door minder actief te worden
Inspanningsdyspnoe Sedentair leven om episodes van dyspnoe te vermijden Lagere levenskwaliteit en sociaal isolement Dyspnoea, or breathlessness is brought on by exertion, so patients often subconsciously adjust their lifestyles to reduce the intensity of this distressing symptom.1,2 However this more sedentary lifestyle leads to further deconditioning, which in turn aggravates dyspnoea, thus leading to a downward spiral or vicious circle of dyspnoea and inactivity which impacts activities of daily living. 3 As the disease progresses, the fear of dyspnoea-inducing activities may worsen, especially during and in the period following an exacerbation. 4 The distressing symptom of shortness of breath, decreased activity and perception of these abnormalities by the individual result in a reduction in health-related quality of life (which can be defined as “the gap between our expectations of health and our experience of it).”2,5 Early intervention with management strategies including structured rehabilitative exercise and pharmacotherapy may help to prevent this insidious spiral downwards. References 1. Gysels M et al. Access to services for patients with chronic obstructive pulmonary disease: the invisibility of breathlessness. J Pain Symptom Manage 2008;36:451–60. 2. ZuWallack R. How are you doing? What are you doing? Differing perspectives in the assessment of individuals with COPD. COPD 2007;4:293–7. 3. Reardon JZ et al. Functional Status and Quality of Life in Chronic Obstructive Pulmonary Disease. Am J Med 2006;119:32–37. 4. Pitta F et al. Physical activity and hospitalization for exacerbation of COPD. Chest 2006;129:536–44. 5. Jones PW. Issues concerning health-related quality of life in COPD. Chest 1995;107:187s–93s. Comorbiditeit (depressie, ...) 12
. 2,5. Early intervention with management strategies including structured rehabilitative exercise and pharmacotherapy may help to prevent this insidious spiral downwards. References. 1. Gysels M et al. Access to services for patients with chronic obstructive pulmonary disease: the invisibility of breathlessness. J Pain Symptom Manage 2008;36:451– ZuWallack R. How are you doing What are you doing Differing perspectives in the assessment of individuals with COPD. COPD 2007;4:293–7. 3. Reardon JZ et al. Functional Status and Quality of Life in Chronic Obstructive Pulmonary Disease. Am J Med 2006;119:32– Pitta F et al. Physical activity and hospitalization for exacerbation of COPD. Chest 2006;129:536– Jones PW. Issues concerning health-related quality of life in COPD. Chest 1995;107:187s–93s. Comorbiditeit. (depressie, ...) 12.")
13
Het ‘Michelin-effect’
Uit Normaal V O L U M E TIJD Inspanning COPD Beperking van de luchtstroom tijdens inspanning HYPERINFLATIE TOEGENOMEN DYSPNOE VERMINDERDE LONGCAPACITEIT

14
Bronchodilatatie bevordert de activiteitsgraad
Expiratoire luchtstroom Verwacht effect van een bronchodilatator Inspiratoire capaciteit Levens- kwaliteit Dyspnoe Uithoudingsvermogen bij inspanning COPD disease management guidelines state that that the aims of effective management include relief of dyspnea, improvement of exercise endurance, and improvement of health-related quality of life.1 Air trapping causes dyspnea, limits activity, and impairs health-related quality of life. SPIRIVA® improves airflow and reduces air trapping to relieve dyspnea and increase activity, which provides sustained improvements in HRQL. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. NHLBI/WHO workshop report Accessed: 14 November 2003. : toename : afname

15
Behandelingsklassen bij COPD
Bronchodilatator met een korte werkingsduur Bronchodilatator met een lange werkingsduur (inhalatie) Vaste combinatie (LABA+ICS) ICS monotherapie Salbutamol (Ventolin®) Salmeterol (Serevent®) Salmeterol + fluticason (Seretide®) Fluticason (Flixotide®) Ipratropium (atrovent) /Fenoterol (berotec) (Duovent®) Formoterol (Foradil® , Oxis® , ...) Formoterol + budesonide (Symbicort®) Budesonide (Miflonide® , Pulmicort®) Tiotropium (Spiriva®) Beclomethason (Beclophar® , Becotide®) Indacaterol (Onbrez®)
 Vaste combinatie. (LABA+ICS) ICS monotherapie. Salbutamol (Ventolin®) Salmeterol (Serevent®) Salmeterol + fluticason (Seretide®) Fluticason (Flixotide®) Ipratropium (atrovent) /Fenoterol (berotec) (Duovent®) Formoterol (Foradil® , Oxis® , ...) Formoterol + budesonide (Symbicort®) Budesonide (Miflonide® , Pulmicort®) Tiotropium (Spiriva®) Beclomethason (Beclophar® , Becotide®) Indacaterol (Onbrez®)")
16
Korte werkingsduur, lange werkingsduur, cortico
Korte werkingsduur, lange werkingsduur, cortico... Wanneer moeten ze worden voorgeschreven? GOLD guidelines.

17
Denken aan COPD Indacaterol (Onbrez®): structuur, overzicht van de klinische gegevens, praktische aspecten Bespreking: Onbrez® voor welke patiënten?
: structuur, overzicht van de klinische gegevens, praktische aspecten Bespreking: Onbrez® voor welke patiënten")
18
Ontwikkeling van een nieuwe bronchodilatator
voor de onderhoudsbehandeling van COPD Criteria voor de ontwikkeling van indacaterol Doeltreffendheid Snelheid Langere werkingsduur 24 uur continue bronchodilatatie Maakt één toediening per dag (o.d.) mogelijk Gunstig veiligheids- en tolerantieprofiel Gebruiksvriendelijke en doeltreffende inhalator Controlemechanismen
 mogelijk. Gunstig veiligheids- en tolerantieprofiel. Gebruiksvriendelijke en doeltreffende inhalator. Controlemechanismen.")
19
Indacaterol (Onbrez®): een nieuwe chemische entiteit
Structuur verschillend van formoterol en salmeterol Combinatie van de gewijzigde kop van formoterol met een rigieder, compacter en korter uiteinde dan bij salmeterol NH HO NH O OH OMe OMe O HN HN HN HN HO HO HO HO H N O O OH OH OH OH OH OH Formoterol Salmeterol

20
Indacaterol (Onbrez®): Verkrijgbaar in 150µg* & 300µg
* 150 µg : de gebruikelijke aanbevolen dosis

21
INERGIZE: het klinisch programma van indacaterol (selectie van studies)
DOSERINGEN COMPARATOREN DUUR AANTAL PATIENTEN INHANCE 150/300 μg o.d. Placebo Tiotropium 18 μg o.d. (open-label) 26 weken 1.683 INVOLVE 300/600 μg o.d. Placebo Formoterol 12 μg b.i.d. 52 weken 1.728 INLIGHT 1 150 μg o.d. Placebo 12 weken 416 INTIME Tiotropium 18 μg o.d. (dubbelblind) 14 dagen (cross-over studie) 169 INLIGHT 2 Placebo Salmeterol 50 µg b.i.d. 998 INDORSE* 150 μg/300 µg o.d. 414 INTENSITY Tiotropium 1.514 *Extensie van de INHANCE-studie N.B. Indacaterol 150 μg en 300 μg éénmaal per dag zijn goedgekeurd in de EU. De aanbevolen dosis is 150 μg éénmaal per dag en mag enkel op medisch advies verhoogd worden 21 21
 26 weken INVOLVE. 300/600 μg o.d. Placebo Formoterol 12 μg b.i.d. 52 weken INLIGHT μg o.d. Placebo. 12 weken INTIME. Tiotropium 18 μg o.d. (dubbelblind) 14 dagen (cross-over studie) 169. INLIGHT 2. Placebo Salmeterol 50 µg b.i.d INDORSE* 150 μg/300 µg o.d INTENSITY. Tiotropium *Extensie van de INHANCE-studie. N.B. Indacaterol 150 μg en 300 μg éénmaal per dag zijn goedgekeurd in de EU. De aanbevolen dosis is 150 μg éénmaal per dag en mag enkel op medisch advies verhoogd worden")
22
Inclusiecriteria van de belangrijkste studies
Mannen of vrouwen van minstens 40 jaar oud Tabagisme (minstens 20 pak-jaren) Klinische diagnose van matig of ernstig COPD ESW nà bronchodilatatie tussen <80% en ≥30% (II en III) van de voorspelde normaalwaarde en een Tiffeneau-index <70% Rekrutering niet beperkt tot patiënten met een beperkte reversibiliteit op bronchodilatatoren met een korte werkingsduur 22
 Klinische diagnose van matig of ernstig COPD. ESW nà bronchodilatatie tussen <80% en ≥30% (II en III) van de voorspelde normaalwaarde en een Tiffeneau-index <70% Rekrutering niet beperkt tot patiënten met een beperkte reversibiliteit op bronchodilatatoren met een korte werkingsduur. 22.")
23
Ontwikkeling van een nieuwe bronchodilatator
voor de onderhoudsbehandeling van COPD Criteria voor de ontwikkeling van indacaterol Doeltreffendheid Snelheid Langere werkingsduur 24 uur continue bronchodilatatie Maakt één toediening per dag (o.d.) mogelijk Gunstig veiligheids- en tolerantieprofiel Gebruiksvriendelijke en doeltreffende inhalator Controlemechanismen
 mogelijk. Gunstig veiligheids- en tolerantieprofiel. Gebruiksvriendelijke en doeltreffende inhalator. Controlemechanismen.")
24
Longfunctie na 26 weken: Indacaterol vs. Salmeterol
Salmeterol 50 µg b.i.d. Indacaterol 150 µg o.d. Verschil in ESW vs. placebo (dalwaarde) (ml) Klinische verbetering van de ESW (specificatie van het protocol) Dag 2 Week 12 Primair eindpunt Week 26 Dalwaarde: u tot u na inhalatie # p < 0,001 vs. placebo; ¶ p < 0,001 vs. Salmeterol INLIGHT 2 Kornmann et al. Eur Respir J 2011; 37: 273–279
 (ml) Klinische verbetering van de ESW (specificatie van het protocol) Dag 2. Week 12. Primair eindpunt. Week 26. Dalwaarde: u tot u na inhalatie. # p < 0,001 vs. placebo; ¶ p < 0,001 vs. Salmeterol. INLIGHT 2. Kornmann et al. Eur Respir J 2011; 37: 273–279.")
25
Longfunctie na 52 weken: Indacaterol vs. Formoterol
Placebo Formoterol 12 µg b.i.d. Indacaterol 300 µg o.d. 1.55 1.50 1.45 1.40 1.35 1.30 1.25 1.20 1.15 *** ††† † 1,48 *** ††† *** 1,45 *** 1,42 *** 1,44 1,38 1,31 * ESW (dalwaarde) (liter) 1,33 1,31 1,28 The primary efficacy analysis in the INVOLVE study (B2334) showed that treatment with indacaterol 300 or 600 µg once daily resulted in trough FEV1 values at week 12 that were significantly higher (1.48 L, p<0.001 in both groups) than in the placebo group (1.31 L). Secondary analyses also showed that trough FEV1 values were significantly higher in indacaterol recipients than in patients receiving formoterol and that the benefits were apparent as early as Day 2 and were sustained through 52 weeks. Reference Magnussen H, Paggiaro P, Jack D, Owen R, Higgins M, Kramer B. Bronchodilator treatment with indacaterol once-daily vs formoterol twice-daily in COPD: a 52-week study. Am J Respir Crit Care Med 2009;179:A6184 (+ Poster [Paggiaro et al]) Dahl R, Kolman P, Jack D, Owen R, Kramer B, Higgins M. Indacaterol once-daily provides sustained 24-hour bronchodilation over 52 weeks of treatment in COPD. Am J Respir Crit Care Med 2009;179:A4545. [CSR Table 11–5, Table 11–12] Dag 2 Week 12 Week 52 Primair eindpunt Dalwaarde: u tot u na inhalatie *p < 0,05, ***p < 0,001 vs. placebo; †p < 0,05, †††p < 0,001 vs. Formoterol INVOLVE Dahl et al. Thorax 2010; 65: 25
 (liter) 1,33. 1,31. 1,28. The primary efficacy analysis in the INVOLVE study (B2334) showed that treatment with indacaterol 300 or 600 µg once daily resulted in trough FEV1 values at week 12 that were significantly higher (1.48 L, p<0.001 in both groups) than in the placebo group (1.31 L). Secondary analyses also showed that trough FEV1 values were significantly higher in indacaterol recipients than in patients receiving formoterol and that the benefits were apparent as early as Day 2 and were sustained through 52 weeks. Reference. Magnussen H, Paggiaro P, Jack D, Owen R, Higgins M, Kramer B. Bronchodilator treatment with indacaterol once-daily vs formoterol twice-daily in COPD: a 52-week study. Am J Respir Crit Care Med 2009;179:A6184 (+ Poster [Paggiaro et al]) Dahl R, Kolman P, Jack D, Owen R, Kramer B, Higgins M. Indacaterol once-daily provides sustained 24-hour bronchodilation over 52 weeks of treatment in COPD. Am J Respir Crit Care Med 2009;179:A4545. [CSR Table 11–5, Table 11–12] Dag 2. Week 12. Week 52. Primair eindpunt. Dalwaarde: u tot u na inhalatie. *p < 0,05, ***p < 0,001 vs. placebo; †p < 0,05, †††p < 0,001 vs. Formoterol. INVOLVE. Dahl et al. Thorax 2010; 65:")
26
Longfunctie na 26 weken: Indacaterol vs. Tiotropium
Placebo Indacaterol 150 µg o.d. Tiotropium 18 µg o.d. Indacaterol 300 µg o.d. open label 1,55 1,50 1,45 1,40 1,35 1,30 1,25 1,20 *** ††† *** †† *** †† 1,48 *** *** † *** 1,45 1,46 1,46 1,44 *** *** 1,44 1,42 1,42 *** 1,40 ESW (dalwaarde) (liter) 1,34 1,28 1,26 B2335S CSR Tables 11–6 and 11–9 References Fogarty C, Worth H, Hébert J et al. Sustained 24-h bronchodilation with indacaterol once-daily in COPD: a 26-week efficacy and safety study. Am J Respir Crit Care Med 2009;179:A4547. Fogarty C, Hebert J, Iqbal A, Owen R, Higgins M, Kramer B. Indacaterol once-daily provides effective 24-h bronchodilation in COPD patients: a 26-week evaluation vs placebo and tiotropium. Abstract to be presented at ERS 2009 Dag 2 Week 12 Week 26 Primaire doelstelling Dalwaarde: u tot u na inhalatie Indacaterol-tiotropium worden op superioriteit vergeleken. Gegevens zijn kleinstekwadratengemiddelden ***p < 0,001 vs. placebo; †p < 0,05, ††p < 0,01, †††p < 0,001 vs. tiotropium INHANCE Donohue et al. AJRCCM 2010; 182: 26
 (liter) 1,34. 1,28. 1,26. B2335S CSR Tables 11–6 and 11–9. References. Fogarty C, Worth H, Hébert J et al. Sustained 24-h bronchodilation with indacaterol once-daily in COPD: a 26-week efficacy and safety study. Am J Respir Crit Care Med 2009;179:A4547. Fogarty C, Hebert J, Iqbal A, Owen R, Higgins M, Kramer B. Indacaterol once-daily provides effective 24-h bronchodilation in COPD patients: a 26-week evaluation vs placebo and tiotropium. Abstract to be presented at ERS Dag 2. Week 12. Week 26. Primaire doelstelling. Dalwaarde: u tot u na inhalatie. Indacaterol-tiotropium worden op superioriteit vergeleken. Gegevens zijn kleinstekwadratengemiddelden. ***p < 0,001 vs. placebo; †p < 0,05, ††p < 0,01, †††p < 0,001 vs. tiotropium. INHANCE. Donohue et al. AJRCCM 2010; 182:")
27
Indacaterol verhoogt de inspiratoire capaciteit
(gemiddelde maximale variatie in liter) D = 250 ml (p=0,0003) D = 317 ml (p=0,0033) 2,5 2,4 2,40 2,3 2,36 Placebo Indacaterol 300µg OD Inspiratoire capaciteit (liter) 2,2 2,1 2,15 2,0 2,05 1,9 Dag 1 Dag 14 Beeh et al. ERS 2009
 D = 250 ml. (p=0,0003) D = 317 ml. (p=0,0033) 2,5. 2,4. 2,40. 2,3. 2,36. Placebo. Indacaterol 300µg OD. Inspiratoire capaciteit (liter) 2,2. 2,1. 2,15. 2,0. 2,05. 1,9. Dag 1. Dag 14. Beeh et al. ERS")
28
Wat biedt indacaterol op klinisch vlak?
Expiratoire luchtstroom Onbrez® (indacaterol) Inspiratoire capaciteit Levens-kwaliteit Dyspnoe Uithoudingsvermogen bij inspanning : toename : afname
 Inspiratoire capaciteit Levens-kwaliteit Dyspnoe. Uithoudingsvermogen bij inspanning. : toename. : afname.")
29
Effect op de dyspnoe: Indacaterol vs Tiotropium op week 12
Patiënten met klinische verbetering van de dyspnoe (toename ≥1 punt op de TDI-score)* p<0,001 57,9% VERBETERING 50,1% TDI total scores showed a significantly greater reduction in dyspnea with indacaterol than with tiotropium (between-group difference 0.58, p<0.001). The analysis of the proportions of patients with a clinically relevant improvement in TDI total score showed that patients receiving indacaterol were significantly more likely (odds ratio 1.49) to achieve a clinically relevant improvement in dyspnea. Baseline dyspnea index (BDI) scores were 6.8 in both treatment groups. Reference Dunn LJ, et al. Blinded 12-week comparison of once-daily indacaterol and tiotropium in COPD. Presented at ACCP 2010. Tiotropium 18µg o.d. Indacaterol 150µg o.d. *: Een toename met ≥1 punt komt overeen met een klinisch relevante verbetering van de dyspnoe INTENSITY Dunn et al. INTENSITY trial presented at ACCP Chest. 2010; 138:719A
* p<0, ,9% VERBETERING. 50,1% TDI total scores showed a significantly greater reduction in dyspnea with indacaterol than with tiotropium (between-group difference 0.58, p<0.001). The analysis of the proportions of patients with a clinically relevant improvement in TDI total score showed that patients receiving indacaterol were significantly more likely (odds ratio 1.49) to achieve a clinically relevant improvement in dyspnea. Baseline dyspnea index (BDI) scores were 6.8 in both treatment groups. Reference. Dunn LJ, et al. Blinded 12-week comparison of once-daily indacaterol and tiotropium in COPD. Presented at ACCP Tiotropium. 18µg o.d. Indacaterol. 150µg o.d. *: Een toename met ≥1 punt komt overeen met een klinisch relevante verbetering van de dyspnoe. INTENSITY. Dunn et al. INTENSITY trial presented at ACCP Chest. 2010; 138:719A.")
30
Indacaterol: Effect op de inspanningstolerantie
Tijd van inspanningstolerantie (fietstest op 80% van de maximale capaciteit) D = 1,46 min (p=0,0032) 8,5 8,47 Placebo Indacaterol 300µg o.d. 8,0 = 0,52 min Tijd (minuten) 7,5 7,46 7,0 6,93 7,01 Dag 1 Dag 14 Beeh et al. ERS 2009
 D = 1,46 min. (p=0,0032) 8,5. 8,47. Placebo. Indacaterol 300µg o.d. 8,0. = 0,52 min. Tijd (minuten) 7,5. 7,46. 7,0. 6,93. 7,01. Dag 1. Dag 14. Beeh et al. ERS")
31
Levenskwaliteit: Respiratoire vragenlijst van St George (SGRQ) op week 12
Patiënten met een klinische verbetering van de levenskwaliteit (vermindering ≥4 punten op de SGRQ-score)* p<0,001 50,5% VERBETERING 42,5% SGRQ total scores demonstrated significantly better health status with indacaterol than with tiotropium. The improvement in SGRQ total score from baseline with indacaterol exceeded the minimal clinically important change (4 units). The analysis of the proportions of patients with a clinically relevant improvement in SGRQ total score showed that patients receiving indacaterol were significantly more likely (odds ratio 1.43) to achieve a clinically relevant improvement in health status. The baseline SGRQ scores were 42.3 (indacaterol group) and 42.7 (tiotropium group). Reference Dunn LJ, et al. Blinded 12-week comparison of once-daily indacaterol and tiotropium in COPD. Presented at ACCP 2010. 42.5 50.5 Tiotropium 18µg o.d. Indacaterol 150µg o.d. *: Een vermindering met ≥4 punten komt overeen met een klinisch relevante verbetering van de levenskwaliteit INTENSITY Dunn et al. INTENSITY trial presented at ACCP Chest. 2010; 138:719A
* p<0, ,5% VERBETERING. 42,5% SGRQ total scores demonstrated significantly better health status with indacaterol than with tiotropium. The improvement in SGRQ total score from baseline with indacaterol exceeded the minimal clinically important change (4 units). The analysis of the proportions of patients with a clinically relevant improvement in SGRQ total score showed that patients receiving indacaterol were significantly more likely (odds ratio 1.43) to achieve a clinically relevant improvement in health status. The baseline SGRQ scores were 42.3 (indacaterol group) and 42.7 (tiotropium group). Reference. Dunn LJ, et al. Blinded 12-week comparison of once-daily indacaterol and tiotropium in COPD. Presented at ACCP Tiotropium. 18µg o.d. Indacaterol. 150µg o.d. *: Een vermindering met ≥4 punten komt overeen met een klinisch relevante verbetering van de levenskwaliteit. INTENSITY. Dunn et al. INTENSITY trial presented at ACCP Chest. 2010; 138:719A.")
32
Levenskwaliteit St. George’s Respiratory Questionnaire (SGRQ)
Formoterol 12 μg b.i.d. Indacaterol 300 μg o.d. Week 4 Week 8 Week 24 Week 44 Week 52 -0,5 -1,0 -1,5 -2,0 -2,5 -3,0 -3,5 -4,0 -4,5 -5,0 VERBETERING Verschil in totale SGRQ-score vs. placebo -2,2 ** -2,8 -3,0 ** -3,3 ** -3,4 *** *** -4,0 B2335 CSR table Reference Magnussen H et al. Indacaterol once-daily improves health-related quality of life in COPD patients: a 52-week study. Abstract presented at ERS 2009. -4,4 *** -4,5 -4,6 -4,7 *** *** *** *** Een vermindering met ≥4 punten komt overeen met een klinisch relevante verbetering van de levenskwaliteit ***p ≤ 0,001, **p < 0,01 vs. placebo. INVOLVE Dahl et al. Thorax 2010; 65: 32

33
Dagen (%) zonder noodmedicatie: Indacaterol vs Tiotropium
Placebo Indacaterol 150µg o.d. Tiotropium 18µg o.d. Indacaterol 300µg o.d. (open label) +58 dagen* +42 dagen* 57,8%° # 56,7%° # 46,1% Dagen zonder noodmedicatie (%) 41,8% VERBETERING * Extrapolatie op jaarbasis in dagen ° p<0,001 vs. placebo; # p<0,001 vs. tiotropium INHANCE Donohue et al. AJRCCM 2010; 182:
 +58 dagen* +42 dagen* 57,8%° # 56,7%° # 46,1% Dagen zonder noodmedicatie (%) 41,8% VERBETERING. * Extrapolatie op jaarbasis in dagen. ° p<0,001 vs. placebo; # p<0,001 vs. tiotropium. INHANCE. Donohue et al. AJRCCM 2010; 182:")
34
Wat biedt indacaterol op klinisch vlak?
Expiratoire luchtstroom Onbrez® (indacaterol) Inspiratoire capaciteit Levenskwaliteit Dyspnoe Uithoudingsvermogen bij inspanning : toename : afname
 Inspiratoire capaciteit Levenskwaliteit Dyspnoe. Uithoudingsvermogen bij inspanning. : toename. : afname.")
35
Indacaterol verlengt de tijd tot de eerste exacerbatie (evaluatie na 52 weken vs. placebo)
Formoterol 12 μg Hazard ratio compared with placebo (95% CI) 0.77 (0.61, 0.98) 0.69 (0.54, 0.88) p value 0.030 0.003 0.034 100 80 60 40 20 Patiënten zonder exacerbatie (%) Exacerbations occurred in 133 (32.8%), 116 (29.3%), 126 (31.5%) and 145 (36.3%) patients in indacaterol 300 µg, indacaterol 600 µg, formoterol and and placebo groups respectively in the INVOLVE (B2334) study. Cox regression analysis of time to first COPD exacerbation showed statistical improvement for indacaterol 300, 600 µg and formoterol vs placebo, with hazard ratios of 0.77 (p=0.029), 0.69 (p=0.003) and 0.77 (p=0.034) respectively. The mean number of exacerbations per patient over 52 weeks were 0.52, 0.48, 0.46 and 0.58 for indacaterol 300 µg, indacaterol 600 µg, formoterol and and placebo groups respectively. COPD exacerbations were defined as onset/worsening of >1 respiratory symptom for >3 consecutive days requiring intensified treatment (e.g. steroids/antibiotics/oxygen), or hospitalization or emergency room visits. Note that the INVOLVE study was not specifically designed to investigate the effect of indacaterol compared with formoterol on exacerbations, and patients were not specifically selected to have a history of exacerbations. INVOLVE (B2334) is a Phase III study. Reference Buhl R et al. Indacaterol once-daily reduces COPD exacerbations over 52 weeks of treatment. Am J Respir Crit Care Med 2009;179:A6185 (+ Poster). Indacaterol 300 μg Indacaterol 600 μg Formoterol 12 μg Placebo Tijd tot de eerste exacerbatie (maanden) INVOLVE Dahl et al. Thorax 2010; 65: 35 35
 0.77 (0.61, 0.98) 0.69 (0.54, 0.88) p value Patiënten zonder exacerbatie (%) Exacerbations occurred in 133 (32.8%), 116 (29.3%), 126 (31.5%) and 145 (36.3%) patients in indacaterol 300 µg, indacaterol 600 µg, formoterol and and placebo groups respectively in the INVOLVE (B2334) study. Cox regression analysis of time to first COPD exacerbation showed statistical improvement for indacaterol 300, 600 µg and formoterol vs placebo, with hazard ratios of 0.77 (p=0.029), 0.69 (p=0.003) and 0.77 (p=0.034) respectively. The mean number of exacerbations per patient over 52 weeks were 0.52, 0.48, 0.46 and 0.58 for indacaterol 300 µg, indacaterol 600 µg, formoterol and and placebo groups respectively. COPD exacerbations were defined as onset/worsening of >1 respiratory symptom for >3 consecutive days requiring intensified treatment (e.g. steroids/antibiotics/oxygen), or hospitalization or emergency room visits. Note that the INVOLVE study was not specifically designed to investigate the effect of indacaterol compared with formoterol on exacerbations, and patients were not specifically selected to have a history of exacerbations. INVOLVE (B2334) is a Phase III study. Reference. Buhl R et al. Indacaterol once-daily reduces COPD exacerbations over 52 weeks of treatment. Am J Respir Crit Care Med 2009;179:A6185 (+ Poster). Indacaterol 300 μg Indacaterol 600 μg. Formoterol 12 μg Placebo Tijd tot de eerste exacerbatie (maanden) INVOLVE. Dahl et al. Thorax 2010; 65:")
36
Ontwikkeling van een nieuwe bronchodilatator
voor de onderhoudsbehandeling van COPD Criteria voor de ontwikkeling van indacaterol Doeltreffendheid Snelheid Langere werkingsduur 24 uur continue bronchodilatatie Maakt één toediening per dag (o.d.) mogelijk Gunstig veiligheids- en tolerantieprofiel Gebruiksvriendelijke en doeltreffende inhalator Controlemechanismen
 mogelijk. Gunstig veiligheids- en tolerantieprofiel. Gebruiksvriendelijke en doeltreffende inhalator. Controlemechanismen.")
37
5 minuten na de inhalatie
Klinische verbetering van de ESW binnen 5 minuten na de eerste inhalatie *** *** *** + 100 ml + 120 ml + 90 ml ** 1,50 + 50 ml 1,48 5 minuten na de inhalatie ESW (liter) 1,47 1,43 1,38 For the primary efficacy variable (FEV1 at 5 minutes post-dose), the least squares mean value for indacaterol 150 and 300 μg was higher than that for placebo by 100 and 120 mL, respectively (p<0.001).1 Such differences (i.e., ≥100 mL) have been described as ones that patients can perceive.2 References 1. Balint B et al. Onset of action of indacaterol in patients with COPD: a comparison with salbutamol and salmeterol/fluticasone. Int J COPD 2010; 5: 311–318. 2. Donohue JF. Minimal clinically important differences in COPD lung function. COPD 2005;2: Placebo (n = 88) Salmeterol/ fluticason (n = 88) Salbutamol (n = 86) Indacaterol 150 µg (n = 85) Indacaterol 300 µg (n = 87) INSURE Balint et al. International Journal of Chronic Obstructive Pulmonary Disease 2010:5; 311–318 ***p < 0,001, **p < 0,01 versus placebo
 1,47. 1,43. 1,38. For the primary efficacy variable (FEV1 at 5 minutes post-dose), the least squares mean value for indacaterol 150 and 300 μg was higher than that for placebo by 100 and 120 mL, respectively (p<0.001).1. Such differences (i.e., ≥100 mL) have been described as ones that patients can perceive.2. References. 1. Balint B et al. Onset of action of indacaterol in patients with COPD: a comparison with salbutamol and salmeterol/fluticasone. Int J COPD 2010; 5: 311– Donohue JF. Minimal clinically important differences in COPD lung function. COPD 2005;2: Placebo. (n = 88) Salmeterol/ fluticason. (n = 88) Salbutamol. (n = 86) Indacaterol. 150 µg. (n = 85) Indacaterol. 300 µg. (n = 87) INSURE. Balint et al. International Journal of Chronic Obstructive Pulmonary Disease 2010:5; 311–318. ***p < 0,001, **p < 0,01 versus placebo.")
38
Ontwikkeling van een nieuwe bronchodilatator
voor de onderhoudsbehandeling van COPD Criteria voor de ontwikkeling van indacaterol Doeltreffendheid Snelheid Langere werkingsduur 24 uur continue bronchodilatatie Maakt één toediening per dag (o.d.) mogelijk Gunstig veiligheids- en tolerantieprofiel Gebruiksvriendelijke en doeltreffende inhalator Controlemechanismen
 mogelijk. Gunstig veiligheids- en tolerantieprofiel. Gebruiksvriendelijke en doeltreffende inhalator. Controlemechanismen.")
39
24 uurs-profiel van de ESW op dag 14 van de behandeling
Indacaterol 300 µg q.d. Salmeterol 50 µg b.i.d. Placebo FEV1 (l) 1,6 1,5 1,4 1,3 1,2 1,1 Tijdstip (uren na dosistoediening) Indacaterol also provided superior bronchodilation compared to placebo across the 24-h assessment period at all post-baseline time points on Day 14 The FEV1 for indacaterol was again higher than that of salmeterol at all time points p < 0,001 voor indacaterol vs. placebo op elk tijdstip; p < 0,05 voor salmeterol vs. placebo op elk tijdstip; †p < 0,05 voor indacaterol vs. salmeterol INTEGRAL LaForce et al. Pulm PharmacolTher 2011; 24:
 1,6. 1,5. 1,4. 1,3. 1,2. 1,1. Tijdstip (uren na dosistoediening) Indacaterol also provided superior bronchodilation compared to placebo across the 24-h assessment period at all post-baseline time points on Day 14. The FEV1 for indacaterol was again higher than that of salmeterol at all time points. p < 0,001 voor indacaterol vs. placebo op elk tijdstip; p < 0,05 voor salmeterol vs. placebo op elk tijdstip; †p < 0,05 voor indacaterol vs. salmeterol. INTEGRAL. LaForce et al. Pulm PharmacolTher 2011; 24:")
40
Ontwikkeling van een nieuwe bronchodilatator
voor de onderhoudsbehandeling van COPD Criteria voor de ontwikkeling van indacaterol Doeltreffendheid Snelheid Langere werkingsduur 24 uur continue bronchodilatatie Maakt één toediening per dag (o.d.) mogelijk Gunstig veiligheids- en tolerantieprofiel Gebruiksvriendelijke en doeltreffende inhalator Controlemechanismen
 mogelijk. Gunstig veiligheids- en tolerantieprofiel. Gebruiksvriendelijke en doeltreffende inhalator. Controlemechanismen.")
41
Cardio- en cerebrovasculaire bijwerkingen
Cardio- en cerebrovasculaire bijwerkingen (%) bij patiënten die minstens 6 maanden met een bronchodilaterend b2-mimeticum werden behandeld (%) p=NS vs placebo p=NS vs placebo p=NS vs placebo Onbrez (alle dosissen samen) formoterol salmeterol placebo Onbrez® (alle dosissen) Formoterol Salmeterol Placebo Worth et al. Respir Med. 2011;105 : 41
 bij patiënten die minstens 6 maanden met een bronchodilaterend b2-mimeticum werden behandeld. (%) p=NS. vs placebo. p=NS. vs placebo. p=NS. vs placebo. Onbrez (alle dosissen samen) formoterol salmeterol placebo. Onbrez® (alle dosissen) Formoterol. Salmeterol. Placebo. Worth et al. Respir Med. 2011;105 :")
42
QTc: geen significant verschil versus placebo of tiotropium
Worth et al. Cardio- and cerebrovascular safety of indacaterol vs formoterol, salmeterol, tiotropium and placebo in COPD. Respir Med. 2011;105 :

43
Gemelde bijwerkingen over 12 maanden
(≥3%) in om het even welke behandelingsgroep Indacaterol 300 μg o.d. (N = 437) n (%) 600 μg o.d. (N = 425) n (%) Formoterol 12 μg b.i.d. (N = 434) n (%) Placebo (N = 432) n (%) Patiënten met (een) bijwerking(en) 310 (70,9) 276 (64,9) 283 (65,2) 267 (61,8) COPD 140 (32,0) 117 (27,5) 134 (30,9) 150 (34,7) Nasofaryngitis 73 (16,7) 80 (18,8) 62 (14,3) 56 (13,0) Hoest 32 (7,3) 27 (6,4) 17 (3,9) 19 (4,4) Bacteriële bovenste LWI 29 (6,6) 25 (5,9) 23 (5,3) 36 (8,3) Lage LWI 27 (6,2) 23 (5,4) 22 (5,1) Spierspasmen 12 (2,8) 6 (1,4) Bovenste LWI 21 (4,8) 20 (4,7) 18 (4,1) 11 (2,5) Hoofdpijn 21 (4,9) 15 (3,5) Influenza 19 (4,5) 13 (3,0) Virale bovenste LWI 8 (1,9) 9 (2,1) Dyspnoe Rugpijn 15 (3,4) Bronchitis 14 (3,2) 16 (3,8) References Novartis Data on File. B2334 study report, Table 12–3. Novartis Data on File. Summary of Clinical Safety, Table 2–5. INVOLVE Novartis Data on File LWI = Luchtweginfectie 43
 in om het even welke behandelingsgroep. Indacaterol. 300 μg o.d. (N = 437) n (%) 600 μg o.d. (N = 425) n (%) Formoterol 12 μg b.i.d. (N = 434) n (%) Placebo. (N = 432) n (%) Patiënten met (een) bijwerking(en) 310 (70,9) 276 (64,9) 283 (65,2) 267 (61,8) COPD. 140 (32,0) 117 (27,5) 134 (30,9) 150 (34,7) Nasofaryngitis. 73 (16,7) 80 (18,8) 62 (14,3) 56 (13,0) Hoest. 32 (7,3) 27 (6,4) 17 (3,9) 19 (4,4) Bacteriële bovenste LWI. 29 (6,6) 25 (5,9) 23 (5,3) 36 (8,3) Lage LWI. 27 (6,2) 23 (5,4) 22 (5,1) Spierspasmen. 12 (2,8) 6 (1,4) Bovenste LWI. 21 (4,8) 20 (4,7) 18 (4,1) 11 (2,5) Hoofdpijn. 21 (4,9) 15 (3,5) Influenza. 19 (4,5) 13 (3,0) Virale bovenste LWI. 8 (1,9) 9 (2,1) Dyspnoe. Rugpijn. 15 (3,4) Bronchitis. 14 (3,2) 16 (3,8) References. Novartis Data on File. B2334 study report, Table 12–3. Novartis Data on File. Summary of Clinical Safety, Table 2–5. INVOLVE. Novartis Data on File. LWI = Luchtweginfectie. 43.")
44
Ontwikkeling van een nieuwe bronchodilatator
voor de onderhoudsbehandeling van COPD Criteria voor de ontwikkeling van indacaterol Doeltreffendheid Snelheid Langere werkingsduur 24 uur continue bronchodilatatie Maakt één toediening per dag (o.d.) mogelijk Gunstig veiligheids- en tolerantieprofiel Gebruiksvriendelijke en doeltreffende inhalator Controlemechanismen
 mogelijk. Gunstig veiligheids- en tolerantieprofiel. Gebruiksvriendelijke en doeltreffende inhalator. Controlemechanismen.")
45
Inhalator Onbrez® Breezhaler®: geschikt voor alle COPD-patiënten
Compact & intuïtief gebruik Lage weerstand: geschikt voor alle COPD-patiënten, ook de patiënten met ernstige obstructie Zekerheid dat de inhoud van de capsule correct wordt geïnhaleerd Reference Pavkov R et al. Concept1 (a new single dose dry powder inhaler) Peak inspiratory flow rate study with COPD patients. Poster presented at Respiratory Drug Delivery 2008, May 11–15, Arizona, USA. Pavkov et al. Curr Med Res Opin 2010; 26:2527–2533 45 45
 Peak inspiratory flow rate study with COPD patients. Poster presented at Respiratory Drug Delivery 2008, May 11–15, Arizona, USA. Pavkov et al. Curr Med Res Opin 2010; 26:2527–")
46
Debiet van de luchtstroom (liter/min) Inspiratoire inspanning (kPa)
Vergelijking van de weerstand tegen de luchtstroom van Onbrez® Breezhaler® vs. andere inhalatoren 120 Toename van de weerstand Onbrez® Breezhaler® 100 Diskus® 80 Turbohaler® Handihaler® Debiet van de luchtstroom (liter/min) 60 Weerstand kPa1/2 l-1 min 40 Onbrez® Breezhaler® 2,2 10-2 Diskus® 2,7 10-2 20 Turbohaler® 3,4 10-2 Reference Singh D, et al. Dose delivery characterization of indacaterol following inhalation by COPD patients. American Thoracic Society (ATS) 2010 (poster). Handihaler® 5,1 10-2 2 4 6 8 10 Inspiratoire inspanning (kPa) Onbrez® Breezhaler® is een geregistreerd handelsmerk van Novartis; Diskus® is een geregistreerd handelsmerk van GlaxoSmithKline; Turbohaler® is een geregistreerd handelsmerk van AstraZeneca; Handihaler® is een geregistreerd handelsmerk van Boehringer Ingelheim. Singh et al. ATS 2010 46
 60. Weerstand. kPa1/2 l-1 min. 40. Onbrez® Breezhaler® 2,2 Diskus® 2,7 Turbohaler® 3,4 Reference. Singh D, et al. Dose delivery characterization of indacaterol following inhalation by COPD patients. American Thoracic Society (ATS) 2010 (poster). Handihaler® 5,1 Inspiratoire inspanning (kPa) Onbrez® Breezhaler® is een geregistreerd handelsmerk van Novartis; Diskus® is een geregistreerd handelsmerk van GlaxoSmithKline; Turbohaler® is een geregistreerd handelsmerk van AstraZeneca; Handihaler® is een geregistreerd handelsmerk van Boehringer Ingelheim. Singh et al. ATS")
47
Conclusies Consequent klinisch programma – directe vergelijkingen
Significante, consistente en klinische verbetering: Longfunctie (ESW, IC) Dyspnoe Uithoudingsvermogen bij inspanning Levenskwaliteit Vermindering van het gebruik van noodmedicatie Behoud van de doeltreffendheid van indacaterol gedurende de volledige duur van de studies (tot 52 weken in fase III) Geruststellend tolerantie- en veiligheidsprofiel. Geen toename van b2-specifieke cardiovasculaire neveneffecten vs. placebo Inhalator met een controlemechanisme
 Dyspnoe. Uithoudingsvermogen bij inspanning. Levenskwaliteit. Vermindering van het gebruik van noodmedicatie. Behoud van de doeltreffendheid van indacaterol gedurende de volledige duur van de studies (tot 52 weken in fase III) Geruststellend tolerantie- en veiligheidsprofiel. Geen toename van b2-specifieke cardiovasculaire neveneffecten vs. placebo. Inhalator met een controlemechanisme.")
48
Verpakking & Doseringen
Onbrez® = verpakkingen voor 30 dagen (30 capsules) 1 inhalatie per dag ‘s Morgens of ‘s avonds, naargelang de gewoonten van de patiënt 2 doseringen 150 µg : de gebruikelijke dosis In Duitsland wordt 80% van de patiënten met 150 µg behandeld 300 µg : maximale dosis Een verbetering van de dyspnoe werd in het bijzonder vastgesteld bij patiënten met ernstig COPD Prijs Publieksprijs: -22 % vs. tiotropium voor 30 dagen Identiek voor de 2 doseringen Terugbetaling B a posteriori zoals de rest van de klasse *Publieksprijs Onbrez® 150µg en 300µg : 39,11€; publieksprijs Spiriva® 50,09€
 1 inhalatie per dag. ‘s Morgens of ‘s avonds, naargelang de gewoonten van de patiënt. 2 doseringen. 150 µg : de gebruikelijke dosis. In Duitsland wordt 80% van de patiënten met 150 µg behandeld. 300 µg : maximale dosis. Een verbetering van de dyspnoe werd in het bijzonder vastgesteld bij. patiënten met ernstig COPD. Prijs. Publieksprijs: -22 % vs. tiotropium voor 30 dagen. Identiek voor de 2 doseringen. Terugbetaling. B a posteriori zoals de rest van de klasse. *Publieksprijs Onbrez® 150µg en 300µg : 39,11€; publieksprijs Spiriva® 50,09€")
49
Denken aan COPD Indacaterol (Onbrez®): structuur, overzicht van de klinische gegevens, praktische aspecten Bespreking: Onbrez® voor welke patiënten?
: structuur, overzicht van de klinische gegevens, praktische aspecten Bespreking: Onbrez® voor welke patiënten")
50
Matig tot zeer ernstig COPD
GOLD guidelines.

51
Voor welke patiënten? Nieuw gediagnosticeerde gevallen van COPD
Eerstelijnsonderhoudsbehandeling Behandelde COPD-patiënten die symptomatisch blijven Als toevoeging bij Tiotropium Bronchodilatator met een korte werkingsduur Als vervanging van Langwerkend b2-mimeticum Vaste combinatie (het inhalatiecorticosteroied in monotherapie behouden indien nodig) Tiotropium (bij intolerantie of onbevredigend effect)
 Tiotropium (bij intolerantie of onbevredigend effect)")
52
US-FDA Clinical Use - The FDA approved indacaterol maleate as a once-daily bronchodilator to prevent COPD symptoms, such as wheezing and breathlessness. - Dosage is 75 μg inhaled once daily every day, which should increase compliance relative to twice-daily inhalers. It is not intended for acute relief of COPD exacerbations. - Common adverse effects seen with use of indacaterol maleate are runny nose, cough, sore throat, headache, and nausea. It will carry a boxed warning that the risk for asthma-related death may be increased. There are several significant drug interactions. - Indacaterol maleate is pregnancy Category C. It should be used during labor only in those patients in whom the benefits clearly outweigh the risks, and caution is warranted when indacaterol maleate is administered to breast-feeding women. - Indacaterol maleate is not indicated for use in children. No adjustment of dosage is warranted in geriatric patients nor in patients with mild and moderate hepatic impairment. Original Page: Saved from Feeddler RSS Reader

53
Vragen?

54
Back-up

55
Hyperinflatie & Air Trapping
Normaal Hyperinflatie Mechanisch compressie-effect op de ademhalingsspieren Grotere inspanning vereist om te ademen Gevoel van dyspnoe en gedaalde inspanningstolerantie Air trapping affects patients with COPD. It results in an expansion of the chest wall, which places the respiratory muscles at a mechanical disadvantage.1 Air trapping limits the ability of patients to expand tidal volume when required, for example, during activity. This makes the patient feel breathless or dyspneic. Hyperinflation, resulting from air trapping, can be observed on standard X-rays. Note the wide intercostal spaces in this patient with COPD, which are caused by air trapping. O'Donnell DE, Webb K. The etiology of dyspnea during exercise in COPD. Pulmonary and Critical Care Update 14, Lesson 15. Accessed 24 February 2004.

56
INTENSITY – Longfunctie na 12 weken: Indacaterol vs. Tiotropium
Tiotropium 18 µg o.d. Indacaterol 150 µg o.d. +130 ml +120 ml Verschil in ESW vs. placebo (dalwaarde) (ml) Week 12 Primair eindpunt p < 0,001 voor non-inferioriteit (primair eindpunt) INTENSITY Dunn et al. INTENSITY trial presented at ACCP Chest. 2010; 138:719A
 (ml) Week 12. Primair eindpunt. p < 0,001 voor non-inferioriteit (primair eindpunt) INTENSITY. Dunn et al. INTENSITY trial presented at ACCP Chest. 2010; 138:719A.")
57
Indacaterol verbetert de ESW significant bij uiteenlopende types COPD-patiënten
Onafhankelijk van reversibiliteit met een bronchodilatator met een korte werkingsduur (SABA en SAMA) Vergelijkbaar bij patiënten < 65 jaar en ≥ 65 jaar Vergelijkbaar bij ex-rokers en rokers Vergelijkbaar bij gebruikers en niet-gebruikers van inhalatiecorticosteroieden (ICS)
 Vergelijkbaar bij patiënten < 65 jaar en ≥ 65 jaar. Vergelijkbaar bij ex-rokers en rokers. Vergelijkbaar bij gebruikers en niet-gebruikers van inhalatiecorticosteroieden (ICS)")
Verwante presentaties












 overgewicht.>")





>")
