Download de presentatie
De presentatie wordt gedownload. Even geduld aub

1
Nieuwe orale anticoagulantia
Algemene informatie niveau 3 Ed Wiltink, ziekenhuisapotheker/klinisch farmacoloog Een initiatief van de Stuurgroep keten Antistollingsbehandeling versie 1, december 2015

2
Naamgeving Apixaban, dabigatran, edoxaban en rivaroxaban zijn orale anti- stollingsmiddelen die aanvankelijk onder de naam Nieuwe Orale AntiCoagulantia (NOAC’s) bekend zijn geworden Toen het nieuwe eraf was is de naam gewijzigd in Direct Werkende Orale AntiCoagulantia (DOAC’s) Tegenwoordig is de naam NOAC’s weer terug: Niet-VKA Orale AntiCoagulantia In deze presentatie worden een aantal basisgegevens van deze nieuwe middelen gepresenteerd
 bekend zijn geworden. Toen het nieuwe eraf was is de naam gewijzigd in Direct Werkende Orale AntiCoagulantia (DOAC’s) Tegenwoordig is de naam NOAC’s weer terug: Niet-VKA Orale AntiCoagulantia. In deze presentatie worden een aantal basisgegevens van deze nieuwe middelen gepresenteerd.")
3
Nadelen huidige anticoagulantia
Heparine Toediening parenteraal (sc, iv) Nauwe therapeutische breedte Labcontrole noodzakelijk (aPTT) Bij langdurig gebruik risico op osteoporose Laag moleculaire heparines geen 100% werkzaam antidotum beschikbaar Optreden HIT(T) syndroom daling trombocyten na dgn sterk verhoogd tromboserisico Coumarine derivaten Grote verschillen in respons Nauwe therapeutische breedte Labcontrole noodzakelijk (INR) Duur intrede werking Genetische variatie (CYP450/VKORC1) Vele interacties Niet toepassen in de zwangerschap Invloed ziekteproces Optreden bijwerkingen (huidnecrose) Therapietrouw
 Nauwe therapeutische breedte. Labcontrole noodzakelijk (aPTT) Bij langdurig gebruik risico op. osteoporose. Laag moleculaire heparines geen 100% werkzaam antidotum beschikbaar. Optreden HIT(T) syndroom. daling trombocyten na dgn. sterk verhoogd tromboserisico. Coumarine derivaten. Grote verschillen in respons. Nauwe therapeutische breedte. Labcontrole noodzakelijk (INR) Duur intrede werking. Genetische variatie (CYP450/VKORC1) Vele interacties. Niet toepassen in de zwangerschap. Invloed ziekteproces. Optreden bijwerkingen (huidnecrose) Therapietrouw.")
4
Het ideale anticoagulans
Vaste orale dosering (1 of 2 dd) Voorspelbaar effect Geen interacties met andere geneesmiddelen en/of voedingsstoffen Monitoring mogelijk maar niet noodzakelijk Antidotum beschikbaar Minstens even effectief en veilig als de in gebruik zijnde middelen Zijn de NOAC’s het ideale anticoagulans ?
 Voorspelbaar effect. Geen interacties met andere geneesmiddelen en/of. voedingsstoffen. Monitoring mogelijk maar niet noodzakelijk. Antidotum beschikbaar. Minstens even effectief en veilig als de in gebruik zijnde. middelen. Zijn de NOAC’s het ideale anticoagulans")
5
Ongefracrioneerde heparine is een indirecte remmer van Factor Xa and trombine
VII TF VIIa Initiation X IX Propagation Xa IXa Indirect inhibition by UFH via antithrombin II Protrombine AT Inactive factor Active factor Transformation Catalysis This slide shows a simplified model of the coagulation pathway. Different anticoagulants target different points in the coagulation pathway. UFH acts via antithrombin to inhibit Factor Xa and thrombin. UFH inhibits Factor Xa and thrombin in a 1:1 ratio. IIa Thrombin Clot formation Fibrinogen Fibrin

6
LMWH is een indirecte remmer van Factor Xa en trombine
VII TF VIIa Initiation X IX Propagation Xa IXa Indirect inhibition by LMWH via antithrombin II Protrombin AT Inactive factor Active factor Transformation Catalysis This slide shows a simplified model of the coagulation pathway. Different anticoagulants target different points in the coagulation pathway. LMWH acts via antithrombin to inhibit Factor Xa and thrombin. LMWH inhibits Factor Xa and thrombin in a different ratio compared with UFH. The ratio of inhibition of Factor Xa and thrombin is different depending on which LMWH is used. IIa Thrombin Clot formation Fibrinogen Fibrin

7
VKAs inhibit the synthesis of coagulation Factors II, VII, IX, and X
Vitamine K antagonisten (VKAs) hebben meerdere aangrijpingspunten in de stollingscascade VII VKA Initiation TF VIIa VKA X IX Propagation Xa IXa VKAs inhibit the synthesis of coagulation Factors II, VII, IX, and X II VKA Inactive factor This slide shows a simplified model of the coagulation pathway. Different anticoagulants target different point in the coagulation pathway. VKAs such as warfarin inhibit the vitamin-K-dependent synthesis of Factors II, VII, IX and X as well as numerous other proteins. Active factor Transformation IIa Catalysis Thrombin Clot formation Fibrinogen Fibrin
 hebben meerdere aangrijpingspunten in de stollingscascade. VII. VKA. Initiation. TF. VIIa. VKA. X. IX. Propagation. Xa. IXa. VKAs inhibit the synthesis of coagulation Factors II, VII, IX, and X. II. VKA. Inactive factor. This slide shows a simplified model of the coagulation pathway. Different anticoagulants target different point in the coagulation pathway. VKAs such as warfarin inhibit the vitamin-K-dependent synthesis of Factors II, VII, IX and X as well as numerous other proteins. Active factor. Transformation. IIa. Catalysis. Thrombin. Clot formation. Fibrinogen. Fibrin.")
8
Fondaparinux is een indirecte Factor Xa remmer
VII TF VIIa Initiation X IX Propagation Xa IXa Indirect inhibition by fondaparinux via antithrombin AT II Inactive factor Active factor Transformation Catalysis This slide shows a simplified model of the coagulation pathway. Different anticoagulants target different point in the coagulation pathway. Fondaparinux is an indirect Factor Xa inhibitor, which acts via antithrombin. It does not inhibit thrombin directly. IIa Thrombin Clot formation Fibrinogen Fibrin

9
Directe trombineremmers
VII TF VIIa Initiation X IX Propagation Xa IXa Direct thrombin inhibition - Hirudin - Argatroban - Bivalirudin - Dabigatran II Inactive factor Active factor Transformation Catalysis This slide shows a simplified model of the coagulation pathway. Different anticoagulants target different point in the coagulation pathway. Thrombin activity is central to both the intrinsic and extinsic pathways. Direct thrombin inhibitors are able to inhibit fibrin-bound and free thrombin. They do not bind to plasma proteins and therefore produce a predictable anticoagulant response. Several specific inhibitors of thrombin, such as lepirudin, bivalirudin and argatroban, are available for clinical use. However, they require parenteral administration, have limited indications and are expensive.1 The direct thrombin inhibitor ximelagatran was withdrawn from the market due to safety concerns. Dabigatran binds to the active site of thrombin by hydrophobic interaction,2 preventing the cleavage of fibrinogen to fibrin, and blocking the final step of the coagulation pathway.1 References 1. Spyropoulos AC et al. Expert Opin Investig Drugs 2007;16:431–40. 2. Hauel NH et al. J Med Chem 2002;45:1757–66. IIa Thrombin Clot formation Fibrinogen Fibrin

10
Directe remmers van Factor Xa
Initiation TF VIIa X IX Xa IXa Propagation Prothrombin II Inactive factor Active factor Transformation Catalysis Direct Factor Xa inhibition Rivaroxaban Apixaban Edoxaban This slide shows a simplified model of the coagulation pathway. Different anticoagulants target different point in the coagulation pathway. Factor Xa and thrombin are the only components of the coagulation cascade common to both the extrinsic and intrinsic coagulation pathways. Factor Xa is an attractive target for therapeutic interventions and several direct Factor Xa inhibitors are in development. Reference Spyropoulos AC. Expert Opin Investig Drugs 2007;16:431–40. IIa Thrombin Clot formation Fibrinogen Fibrin Adapted from Spyropoulos AC. Expert Opin Investig Drugs 2007;16:431–40.

11
Direct werkende orale anticoagulantia
Anti-Xa activiteit: apixaban, edoxaban en rivaroxaban Anti-IIa activiteit: dabigatran

12
Farmacokinetische gegevens
Apixaban (Xa) Dabigatran (IIa) Rivaroxaban (Xa) Edoxaban (Xa) Merknaam Eliquis® Dabigatran® Xarelto® Lixiana® Pro-drug nee ja Halfwaardetijd (uur) 12 (8 – 15) 13 (11 – 22) 11 (9 – 13) Tmax (uur) 1 - 3 1,25 - 3 2 - 4 1 - 2 Renale klaring ~ 25% 80 % 66% , waarvan de helft als inactieve metabolieten 35% Orale biologische beschikbaarheid ~ 66% 6,5% 80% 62% Betrokken CYP enzymen metabolisering CYP3A4 geen CYP3A4 en CYP2J2 CYP3A4/5 Plasma eiwitbinding 87% % 55% Verdelingsvolume (l) 21 50 107
 Dabigatran (IIa) Rivaroxaban (Xa) Edoxaban (Xa) Merknaam. Eliquis® Dabigatran® Xarelto® Lixiana® Pro-drug. nee. ja. Halfwaardetijd (uur) 12 (8 – 15) 13 (11 – 22) 11 (9 – 13) Tmax (uur) , Renale klaring. ~ 25% 80 % 66% , waarvan de helft als inactieve metabolieten. 35% Orale biologische beschikbaarheid. ~ 66% 6,5% 80% 62% Betrokken CYP enzymen metabolisering. CYP3A4. geen. CYP3A4 en CYP2J2. CYP3A4/5. Plasma eiwitbinding. 87% % 55% Verdelingsvolume (l)")
13
Invloed van de nierfunctie op de halfwaardetijd
eGFR (ml/min.) T½ (uur) Dabigatran 80 51-80 30-50 < 30 13 (11-22) 15 (12-34) 18 (13-23) 27 (22-35) Rivaroxaban > 30 11 (9-13) Apixaban > 25 12 (8-15) Edoxaban > 50
 T½ (uur) Dabigatran < (11-22) 15 (12-34) 18 (13-23) 27 (22-35) Rivaroxaban. > (9-13) Apixaban. > (8-15) Edoxaban. >")
14
Indicaties en doseringen
Apixaban Dabigatran Rivaroxaban Edoxaban Merknaam Eliquis® Pradaxa® Xarelto® Lixiana® Beschikbare orale vormen tabl. 2,5 en 5 mg caps en mg tabl. 2,5, 10, 15 en mg tabl. 15, 30 en 60 mg Indicaties Preventie VTE 2 dd 2,5 mg 1 dd 220 mg 1 dd 10 mg --- Behandeling VTE 2 dd 10 mg, daarna mg 2 dd (3 mnd.) 2 dd 150 mg 2 dd 15 mg (21 dagen), daarna 1 dd 20 mg 1 dd 60 mg Preventie recidiverende VTE 2 dd 2,5 mg na 6 mnd. antistollingsbehandeling Preventie CVA bij AF 2 dd 5 mg 1 dd 20 mg Preventie atherosclerotische complicaties na ACS Bij nierfunctiestoornissen dienen de doseringen te worden aangepast (zie tabel)
 2 dd 150 mg. 2 dd 15 mg (21 dagen), daarna 1 dd 20 mg. 1 dd 60 mg. Preventie recidiverende VTE. 2 dd 2,5 mg na 6 mnd. antistollingsbehandeling. Preventie CVA bij AF. 2 dd 5 mg. 1 dd 20 mg. Preventie atherosclerotische complicaties na ACS. Bij nierfunctiestoornissen dienen de doseringen te worden aangepast (zie tabel)")
15
Dosisaanpassing bij nierfunctieverlies
eGFR (ml/min.) apixaban dabigatran rivaroxaban Preventie VTE 2 dd 2,5 mg 1x 75 mg, dan 1 dd 150 mg 1 dd 10 mg Behandeling VTE 2 dd 10 mg, dan 2 dd 5 mg 2 dd 110 mg 2 dd 15 mg dan 1 dd 15 mg Preventie recidiverende VTE 2 dd 2,5 mg na 6 mnd. antistollingsbehandeling 2 dd 15 mgdan 1 dd 15 mg Preventie CVA 2 dd 5 mg 1 dd 15 mg Preventie complicaties ACS --- voorzichtig doseren contra-indicatie 2 dd 2.5 2 dd 2.5 mg Voor edoxaban geldt 1 dd 30 mg voor alle geregistreerde indicaties
 apixaban. dabigatran. rivaroxaban Preventie VTE. 2 dd 2,5 mg. 1x 75 mg, dan 1 dd 150 mg. 1 dd 10 mg. Behandeling VTE. 2 dd 10 mg, dan 2 dd 5 mg. 2 dd 110 mg. 2 dd 15 mg dan 1 dd 15 mg. Preventie recidiverende VTE. 2 dd 2,5 mg na 6 mnd. antistollingsbehandeling. 2 dd 15 mgdan 1 dd 15 mg. Preventie CVA. 2 dd 5 mg. 1 dd 15 mg. Preventie complicaties ACS voorzichtig doseren. contra-indicatie. 2 dd dd 2.5 mg Voor edoxaban geldt 1 dd 30 mg voor alle geregistreerde indicaties.")
16
Interacties Apixaban Dabigatran Rivaroxaban Edoxaban
Potente CYP3A4 remmers of aanjagers van CYP3A4 P-gp remmers of aanjagers Potente CYP3A4 remmers of aanjagers van CYP3A4 of P-gp remmers De volgende middelen worden beschouwd als potente CYP3A4 remmers: Vb: ketoconazol, claritromycine, ritonavir en atazanavir deze verhogen de spiegel van apixaban De volgende middelen worden beschouwd als aanjager van CYP3A4: Vb: rifampicine, fenytoïne, carbamazepine, fenobarbital Deze verlagen de spiegel van apixaban Sterke P-gp remmers o.a. ciclosporine, ketoconazol, itraconazol, tacrolimus zijn gecontra-indiceerd P-gp inductoren zoals: rifampicine, carbamazepine, St. Janskruid of fenytoine kunnen leiden tot een verlaagde spiegel van dabigatran Zie onder apixaban Zie onder dabigatran Combinatie van CYP3A4 en P-gp beïnvloedende geneesmiddelen kan een interacterend effect versterken of verzwakken Bij gelijktijdig gebruik van edoxaban met ciclosporine, dronedarone, erytromycine of ketoconazol is dosisverlaging tot eenmaal daags 30 mg nodig. Noot: deze tabel geeft slechts een indicatie en geen volledig overzicht van alle interacties !

17
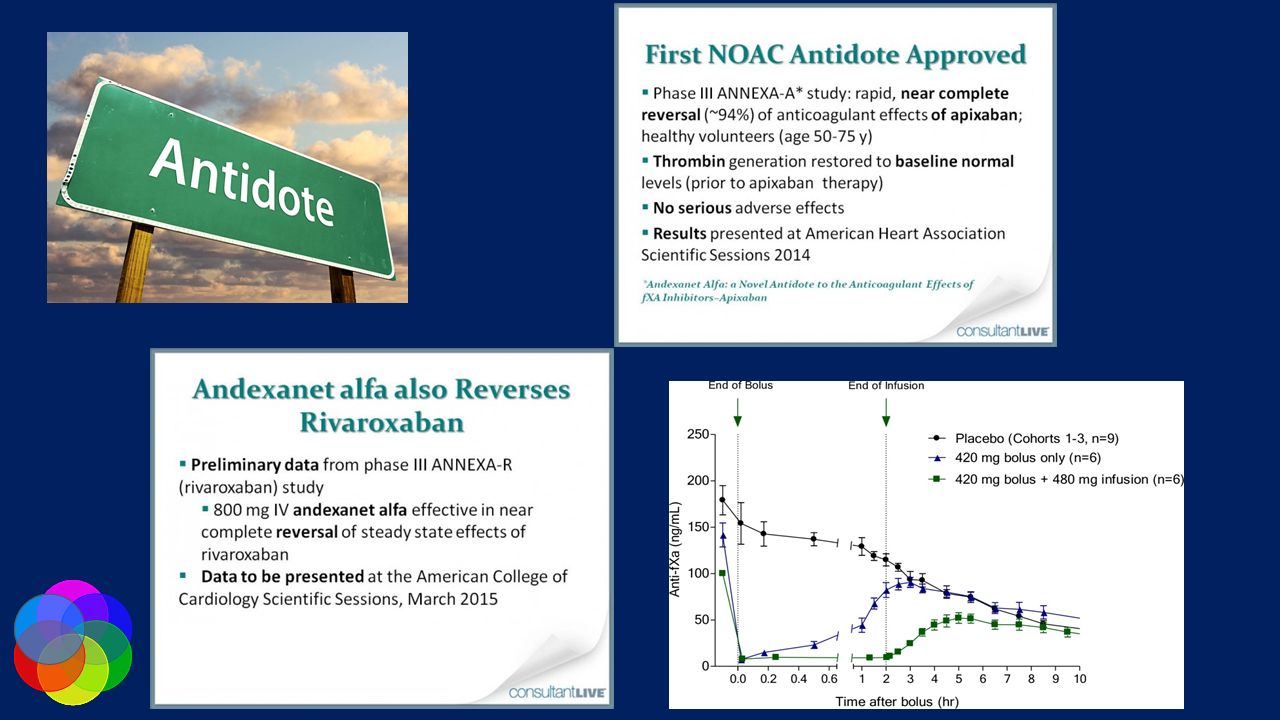
Antidotum voor rivaroxaban
Uit onderzoek bij gezonde vrijwilligers blijkt, dat het mogelijk is met hoge doseringen vierstollingsfactoren- concentraat (PCC) het effect van rivaroxaban te couperen Eerenberg ES, et al. Circulation 2011;124:
 het effect van rivaroxaban te couperen. Eerenberg ES, et al. Circulation 2011;124:")
19
Antidotum voor dabigatran
Met idarucicumab is het mogelijk het anticoagulerend effect van dabigatran te couperen Pollack CV, et al. N Eng J Med 2015

20
NOAC’s vs. warfarin: significante afname in beroerte en systemische embolie

21
NOAC’s zijn op zijn minst even veilig als warfarine wat betreft ernstige bloedingen

22
NOAC’s verminderen significant haemorrhagische beroerte en all-cause dood in vergelijking met warfarin

23
Zorgen rondom NOACs Bij introductie NOAC weinig ervaring met NOAC in de dagelijkse klinische praktijk in Nederland Hierdoor veel zorgen over effectiviteit en veiligheid van NOAC in dagelijkse praktijk Effectiviteit in dagelijkse praktijk (ouderen, polyfarmacie, nierfunctiestoornissen, etc). Management van bloedingen bij gebrek antidotum. Therapietrouw bij NOAC en gevolgen voor patiënten? Door wegvallen trombosedienst ook de ‘regiefunctie’ van de trombosedienst over de antistollingsbehandeling weggevallen. Voor NOAC was nog niet duidelijk vastgelegd wie deze regiefunctie zal overnemen.
. Management van bloedingen bij gebrek antidotum. Therapietrouw bij NOAC en gevolgen voor patiënten Door wegvallen trombosedienst ook de ‘regiefunctie’ van de. trombosedienst over de antistollingsbehandeling weggevallen. Voor. NOAC was nog niet duidelijk vastgelegd wie deze regiefunctie zal. overnemen.")
24
NOACs in de dagelijkse praktijk
- Real-world data -

25
FDA Medicare database (dabigatran)
Observationele studie patiënten, patiënten > 65jr De novo OAC bij AF 84% van de d patiënten kreeg dabigatran 150mg 2dd David J. Graham et al. Circulation. 2015;131:

26
FDA Medicare database (dabigatran)
David J. Graham et al. Circulation. 2015;131:

27
FDA Medicare database (dabigatran)
No. of Events Incidence Rate per 1000 Person-Years Adjusted Hazard Ratio (95% CI) P Value Dabigatran Warfarin Primary outcomes Ischemic stroke 205 270 11.3 13.9 0.80 (0.67–0.96) 0.02 Major bleeding 777 851 42.7 43.9 0.97 (0.88–1.07) 0.50 Gastrointestinal 623 513 34.2 26.5 1.28 (1.14–1.44) <0.001 Intracranial 60 186 3.3 9.6 0.34 (0.26–0.46) Acute myocardial infarction 285 327 15.7 16.9 0.92 (0.78–1.08) 0.29 Secondary outcomes All hospitalized bleeds 1079 1139 59.3 58.8 1.00 (0.92–1.09) 0.97 Mortality 603 744 32.6 37.8 0.86 (0.77–0.96) 0.006 David J. Graham et al. Circulation. 2015;131:
 P Value. Dabigatran. Warfarin. Primary outcomes. Ischemic stroke (0.67–0.96) Major bleeding (0.88–1.07) Gastrointestinal (1.14–1.44) < Intracranial (0.26–0.46) Acute myocardial. infarction (0.78–1.08) Secondary outcomes. All hospitalized bleeds (0.92–1.09) Mortality (0.77–0.96) David J. Graham et al. Circulation. 2015;131:")
28
Beyer-Westendorf et al. Blood, 2014.
Dresden NOAC Registry Beyer-Westendorf et al. Blood, 2014.

29
Effectiviteit en veiligheid in de orthopedie
J Thromb Thrombolysis DOI /s

30
Conclusies NOAC’s verminderen het risico op ernstige bloedingen
De uitkomst na een ernstige bloeding is beter met de NOAC’s De werkzaamheid en veiligheid van NOAC’s in de dagelijkse praktijk is op zijn minst hetzelfde als in de trials.

31
Het ideale antitromboticum ?
dabigatran etexilaat rivaroxaban apixaban endoxaban Vaste orale dosering + / - + Voorspelbaar effect Interacties minder dan VKA Monitoring monitoring niet noodzakelijk, maar ook niet mogelijk Antidotum idarucizumab vierstollingsfactoren-concentraat - Minstens even effectief en veilig + + ++

Verwante presentaties