Download de presentatie
De presentatie wordt gedownload. Even geduld aub

1
HIV en Hart en vaatziekten
Marc van der Valk

2
Bijwerkingen HIV therapie
Korte termijn Lange termijn Hart en vaatziekten Lipodystrofie syndroom polyneuropathie (aantasting van zenuwuiteinden) Osteoporose (Botontkalking) (nierziekten) (leverziekten) (maligniteiten)
 Osteoporose (Botontkalking) (nierziekten) (leverziekten) (maligniteiten)")
3
Korte termijn bijwerkingen
Zeer veel combinaties maag darm bezwaren Efavirenz (stocrin) / nevirapine (viramune) huidafwijkingen Gestoorde leverwaarden Etc etc etc Dromen/ derealisatie/ depersonalisatie efavirenz (stocrin/ atripla)
 / nevirapine (viramune) huidafwijkingen. Gestoorde leverwaarden. Etc etc etc. Dromen/ derealisatie/ depersonalisatie efavirenz (stocrin/ atripla)")
5
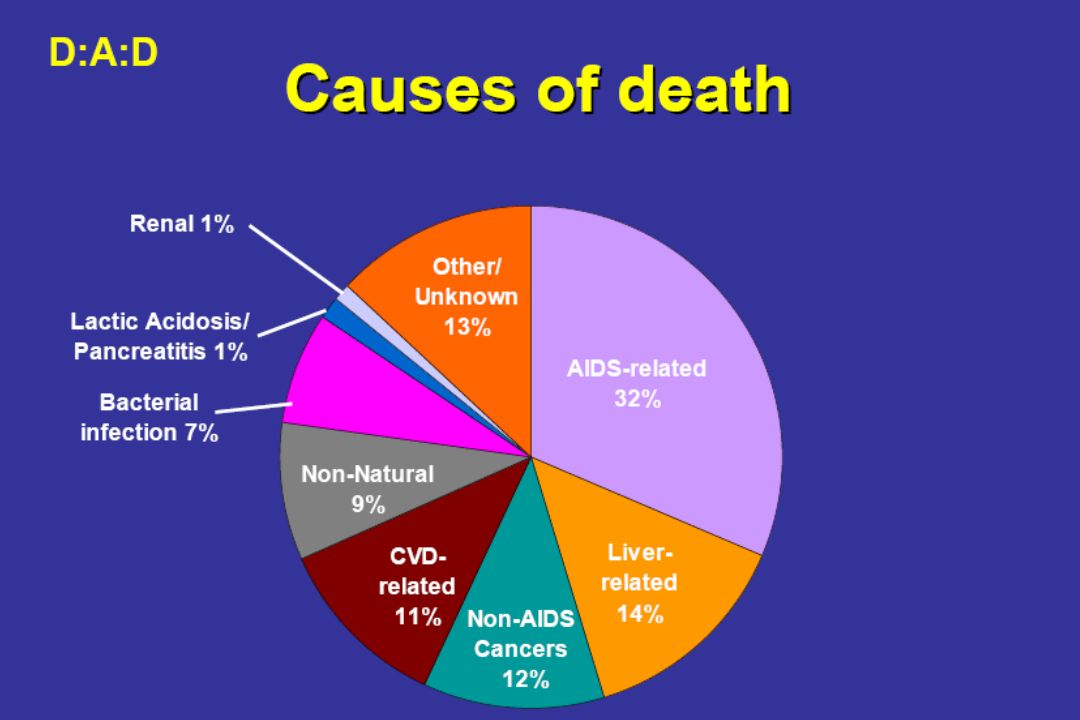
Hart en vaatziekten (CVD) (coronary vascular disease)
 (coronary vascular disease)")
6
Risico op hartinfarct per jaar antiretrovirale therapie
RR per year of cART: Univariable: [ ] Adjusted: [ ] Total 345 94469 Events PYFU

7
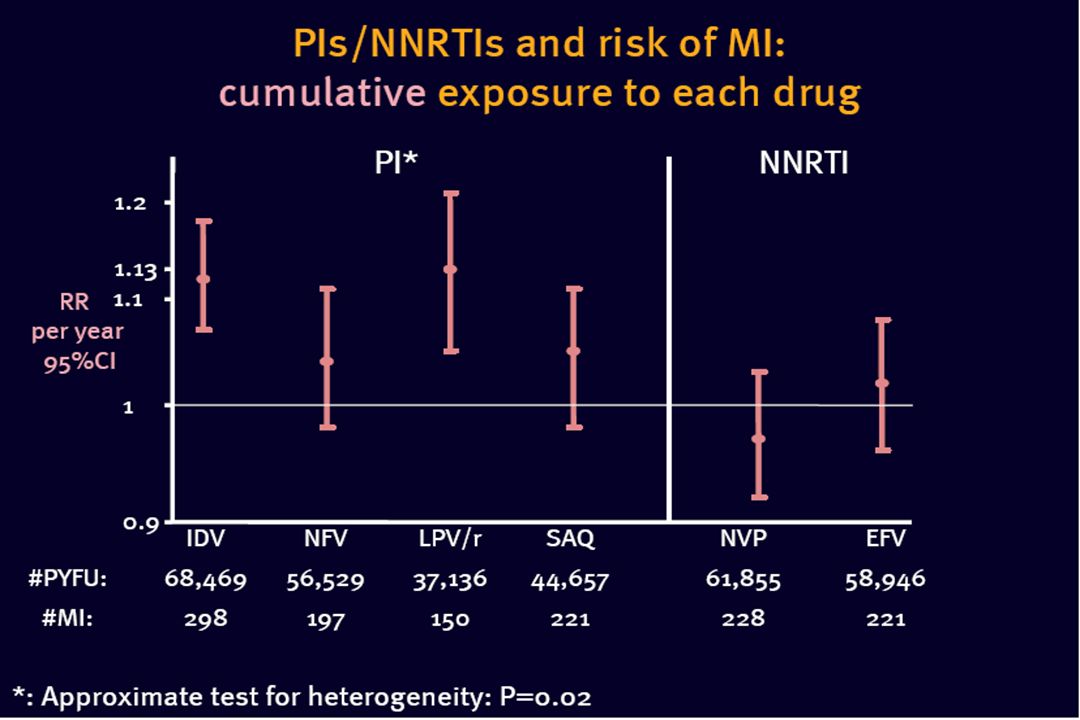
Adjusted RR* per year of PI: 1.16 [1.10-1.23]
Relatief risico op het krijgen van een hartinfarct per jaar blootstelling aan protease remmers Adjusted RR* per year of PI: 1.16 [ ] : Adjusted for sex, age, cohort, calendar year, prior CVD, family history of CVD, smoking, body-mass index, NNRTI exposure
![Adjusted RR* per year of PI: 1.16 [ ]](http://slideplayer.nl/slide/7251154/24/images/7/Adjusted+RR%2A+per+year+of+PI%3A+1.16+%5B+%5D.jpg "Relatief risico op het krijgen van een hartinfarct per jaar blootstelling aan protease remmers. Adjusted RR* per year of PI: 1.16 [ ] : Adjusted for sex, age, cohort, calendar year, prior CVD, family history of CVD, smoking, body-mass index, NNRTI exposure.")
9
Update Relatief risico op het krijgen van een hartinfarct per jaar blootstelling aan protease remmers Wel voor lopinavir (kaletra) en indinavir Niet voor nelfinavir en saquinavir (invirase/fortofase) Nieuwe protease remmers (atazanavir/ darunavir/ amprenavir) vooralsnog onbekend
 en indinavir. Niet voor nelfinavir en saquinavir (invirase/fortofase) Nieuwe protease remmers (atazanavir/ darunavir/ amprenavir) vooralsnog onbekend.")
10
Adjusted RR* per year of NNRTI: 1.05 [0.98-1.13]
Relatief risico op het krijgen van een hartinfarct per jaar blootstelling aan NNRTI (efavirenz/ nevirapine) Adjusted RR* per year of NNRTI: 1.05 [ ] : Adjusted for sex, age, cohort, calendar year, prior CVD, family history of CVD, smoking, body-mass index, PI exposure
![Adjusted RR* per year of NNRTI: 1.05 [ ]](http://slideplayer.nl/slide/7251154/24/images/10/Adjusted+RR%2A+per+year+of+NNRTI%3A+1.05+%5B+%5D.jpg "Relatief risico op het krijgen van een hartinfarct per jaar blootstelling aan NNRTI (efavirenz/ nevirapine) Adjusted RR* per year of NNRTI: 1.05 [ ] : Adjusted for sex, age, cohort, calendar year, prior CVD, family history of CVD, smoking, body-mass index, PI exposure.")
12
Predicting Myocardial Infarction With the Framingham Risk Equation
MI per 1000 years 1 2 3 4 5 6 7 8 Duration of HAART (yrs) < 1 1-2 2-3 3-4 4+ Observed Predicted Law MG, et al. HIV Medicine 2006
 < Observed. Predicted. Law MG, et al. HIV Medicine")
13
D:A:D study Voorspellers hartinfarct bij HIV Adjusted RR 1.17
Haart per jaar Leeftijd per 5 jaar ouder Mannelijk geslacht Eerder hart-vaatziekten roken Familie hart en vaatziekten Adjusted RR (95% CI: ) 0.1 1 10 100 Relatieve risico op hart infarct (95% CI) Aangepast voor familie geschiedenis, BMI, HIV risk, cohort, kalendar jaar and ras El Sadr W, et al. 12th CROI Abstract 745.
 Relatieve risico op hart infarct (95% CI) Aangepast voor familie geschiedenis, BMI, HIV risk, cohort, kalendar jaar and ras. El Sadr W, et al. 12th CROI Abstract 745.")
14
Conclusies Door niet aan HIV gerelateerde factoren ( klassieke risicofactoren) veel groter risico op hart en vaatziekten ivt effect van medicatie/HIV zelf
 veel groter risico op hart en vaatziekten ivt effect van medicatie/HIV zelf.")
15
Impact van Roken op hart en vaatziekten
DAD Study Group. NEJM 2007, 356: RR (95% CI) Eerder HVZ ( ) Roken ( ) Hoge bloeddruk ( ) Totaal cholesterol 1.26 ( )
 Eerder HVZ 4.64 ( ) Roken 2.92 ( ) Hoge bloeddruk 1.30 ( ) Totaal cholesterol 1.26 ( )")
16
Interheart study Lancet vol 368 Aug 19 2007

17
HIV geinfecteerden individuen roken meer
70 p<0.0001 APROCO Cohort (HIV+) 60 MONICA sample (HIV–) p<0.0001 50 p=NS 40 Percent patients 30 p<0.01 20 10 p=NS 17 Smoking Hypertension Blood glucose 126 mg/dL HDL-C <40 mg/dL LDL-C >160 mg/dL HIV+ men and women (N=223) on PI-based regimens vs 527 HIV– male subjects: Savès M et al. Clin Infect Dis 2003;37:292–298
 60. MONICA sample (HIV–) p< p=NS. 40. Percent patients. 30. p< p=NS. 17. Smoking. Hypertension. Blood. glucose. 126 mg/dL. HDL-C. <40 mg/dL. LDL-C. >160 mg/dL. HIV+ men and women (N=223) on PI-based regimens vs 527 HIV– male subjects: Savès M et al. Clin Infect Dis 2003;37:292–298.")
18
Hoge bloedvetten

19
Anitchkov (1913)
")
20
Gezonde vrijwilligers

21
Worteltjes en groene sla

22
Ei geel

23
Goede en slechte bloedvetten
From the liver Back to the liver “Reverse cholesterol transport” TG TG C C C C C apoB apoB apoB apoB apo A-I VLDL IDL large buoyant LDL small dense LDL HDL slecht goed

24
HIV heeft een effect op bloedvetten
HDL cholesterol = goede cholesterol LDL cholesterol = slechte cholesterol Meer kleine dense LDL deeltjes (LDL-B phenotype) Triglyceriden Grunfeld C, et al. J Clin Endocrinol Metab. 1992;74:
 Triglyceriden. Grunfeld C, et al. J Clin Endocrinol Metab. 1992;74:")
25
Risico op afwijkende bloedvetten
7,483 patienten The risk estimates are adjusted for age, sex, parameters related to HIV-disease and parameters related to cardiovascular risk factors. Therapy naïve patients are used as a reference group and have therefore an odds ratio of 1. Using a multivariate logistic regression model, we assessed the risk of dislipideamia by first line regimen for each lipid parameter. Within the PI group, the risks are higher for those on a double PI-regimen. Similar analyses are undertaken to investigate the lipid profiles for different PI’s and combinations thereof. These are however beyond the scope of this analysis. Patients using a PI based regimen have a statistically significant increased risk of dislipidaemia for each of the lipid parameters compared to the naïve patients. But the risk of an increased concentration of triglycerides or LDL-cholesterol is not statistically significant higher compared to therapy naïve patients. For these patients, the risk of an increased total cholesterol is also significant higher compared to naïve patients. Again, the picture is different for patients using an nNRTI. The risk estimates for nevirapine and efavirenz are very similar. Nor is the risk of a decreased HDL-cholestrol concentration. Triglyceriden Totaal chol LDL-chol HDL-chol *aangepast voor geslacht, lftd, BMI, roken, eerder hart en vaatziekten, familie hart en vaatziekten, lipodystrophy, CD4, HIV-RNA, eerdere AIDS diagnose Van Leth et al. CROI 2002

26
Suikerziekte

27
Hoe erg is suikerziekte eigenlijk?
Hartinfarct bij mensen met en zonder suikerziekte No DM DM 100 200 300 400 500 MI events per 1,000 person-yrs 35 188 202 NS* 450 p<0.001 p <0.001 No prior MI (N=2,194) Prior MI (N=238) MI: myocardial infarction; NS: non-significant difference (from Cox proportional hazards model analysis) Adapted from: Haffner SM et al. N Engl J Med 1998;339:229–234
 Prior MI (N=238) MI: myocardial infarction; NS: non-significant difference (from Cox proportional hazards model analysis) Adapted from: Haffner SM et al. N Engl J Med 1998;339:229–234.")
28
Risico op suikerziekte groter bij HIV ivt niet HIV geinfecteerden
Juli 1994–Juni 2000 7,219 HIV patienten (61% man) and 2 ,792,971 niet-HIV (30% man) geinfecteerden 14 - HIV 12 - geen-HIV 10 - 8 - (per 100 person-years) Diabetes incidentie 6 - 4 - 2 - 0 - 18–24 25–34 35–44 45–54 55–64 65+ Age group Currier JS et al. 9th CROI 2002, abstract 677
 and 2 ,792,971 niet-HIV (30% man) geinfecteerden HIV geen-HIV (per 100 person-years) Diabetes incidentie –24. 25–34. 35–44. 45–54. 55– Age group. Currier JS et al. 9th CROI 2002, abstract 677.")
29
Welke pillen kunnen effect hebben op suikerstofwisseling
Alle protease remmers (muv atazanavir / reyataz) Ook oudere NRTI (d4T (zerit) >ZDV) Behandeling DM bij HIV net zoals bij patienten zonder HIV.
 Ook oudere NRTI (d4T (zerit) >ZDV) Behandeling DM bij HIV net zoals bij patienten zonder HIV.")
30
Als die pillen zo slecht zijn waarom dan niet tijdelijk stoppen???
Meer hart en vaatziekten bij patiënten die tijdelijk stopten! (SMART studie 2008) Oorzaak mogelijk gelegen in meer chronische ontstekingsreactie in het lichaam tgv HIV virus
 Oorzaak mogelijk gelegen in meer chronische ontstekingsreactie in het lichaam tgv HIV virus.")
31
Acuut Coronair Syndroom & Acuut Myocard Infarct
Ivo van der Bilt, Cardiologie AMC, Amsterdam Cardionetworks

32
Begripsbepaling Begripsbepaling/Definities Pathofysiologie
Klachten & symptomen Diagnostiek Therapie

33
Definities Hypoxie (Grieks) verminderde zuurstof in de weefsels
Anoxie (Grieks) zeer laag/afwezig zuurstof in de weefsels Perfusie (Latijn) weefseldoorstroming Ischemie (Grieks) inadequate bloedtoevoer van weefsel of orgaan soorten: - supply - demand dysbalans = ischemie in principe reversibel Angina (Latijn) pijn Pectoris (Latijn) van de borst
 zeer laag/afwezig zuurstof in de weefsels. Perfusie (Latijn) weefseldoorstroming. Ischemie (Grieks) inadequate bloedtoevoer van weefsel of orgaan. soorten: - supply. - demand dysbalans = ischemie. in principe reversibel. Angina (Latijn) pijn. Pectoris (Latijn) van de borst.")
34
Definities Necrose (Grieks) accidentele, door externe factoren veroorzaakte, celdood Infarct (Latijn) irreversibele (orgaan)schade DUS: Angina pectoris “Pijn op de borst (letterlijk) veroorzaakt door reversibele, maar inadequate bloedtoevoer van (een deel van) de hartspier ( dysbalans tussen supply + demand).”
 veroorzaakt door reversibele, maar inadequate bloedtoevoer van (een deel van) de hartspier ( dysbalans tussen supply + demand).")
35
Angina Pectoris = Hartkramp

36
Pijn op de Borst ≠ Hartkramp

37
Pijn op de borst cardiaal (hart) vaten (aneurysma/ dissectie)
pulmonaal (longen) abdominaal (buik/ maag) Myalgeen (spieren) anders
 abdominaal (buik/ maag) Myalgeen (spieren) anders.")
38
Begripsbepaling Stabiele angina pectoris
Chronische verminderde supply als gevolg van coronair stenosen. In rust is er voldoende perfusie. Indien demand hoger wordt, treedt pijn op de borst op. Zodra de demand minder wordt, verdwijnen de klachten. Instabiele angina pectoris Acute maar reversibele inadequate bloedvoorziening (supply) van (een deel van) de hartspier ten gevolge van het tekort schieten van de bloedtoevoer (kan irreversibel worden = myocard infarct) CCU indicatie. CAVE: dreigend infarct.
 van (een deel van) de hartspier ten gevolge van het tekort schieten van de bloedtoevoer (kan irreversibel worden = myocard infarct) CCU indicatie. CAVE: dreigend infarct.")
39
Begripsbepaling Instabiele angina pectoris
Acute maar reversibele inadequate bloedvoorziening van (een deel van) de hartspier ten gevolge van het tekort schieten van de bloedtoevoer (kan irreversibel worden = myocard infarct). Acuut myocard infarct Acute en irreversibele beschadiging van (een deel van) de hartspier ten gevolge van het tekort schieten van de bloedtoevoer, leidend tot necrose en verlittekening van het desbetreffende deel van het myocard.
 de hartspier ten gevolge van het tekort schieten van de bloedtoevoer (kan irreversibel worden = myocard infarct). Acuut myocard infarct. Acute en irreversibele beschadiging van (een deel van) de hartspier ten gevolge van het tekort schieten van de bloedtoevoer, leidend tot necrose en verlittekening van het desbetreffende deel van het myocard.")
40
NYHA-klasse New York Heart Association Bij stabiele AP of hartfalen
Functionele klasse I-IV I Geen of sporadisch klachten II Klachten bij zware inspanning III Klachten bij lichte inspanning IV Klachten in rust

41
Pathofysiologie

42
Schematic of the Life History of a Human Coronary Atheroma
Figure 4 Schematic of the life history of an atheroma. The normal human coronary artery has a typical trilaminar structure. The endothelial cells in contact with the blood in the arterial lumen rest upon a basement membrane. The intimal layer in adult humans generally contains a smattering of smooth muscle cells scattered within the intimal extracellular matrix. The internal elastic lamina forms the barrier between the tunica intima and the underlying tunica media. The media consists of multiple layers of smooth muscle cells, much more tightly packed than in the diffusely thickened intima, and embedded in a matrix rich in elastin as well as collagen. In early atherogenesis, recruitment of inflammatory cells (Figs 1–3) and the accumulation of lipids leads to formation of a lipid-rich core, as the artery enlarges in an outward, ablumenal direction to accommodate the expansion of the intima. If inflammatory conditions prevail and risk factors such as dyslipidaemia persist, the lipid core can grow, and proteinases secreted by the activated leukocytes can degrade the extracellular matrix, while pro-inflammatory cytokines such as interferon- (IFN-) can limit the synthesis of new collagen. These changes can thin the fibrous cap and render it friable and susceptible to rupture. When the plaque ruptures, blood coming in contact with the tissue factor in the plaque coagulates. Platelets activated by thrombin generated from the coagulation cascade and by contact with the intimal compartment instigate thrombus formation. If the thrombus occludes the vessel persistently, an acute myocardial infarction can result (the dusky blue area in the anterior wall of the left ventricle, lower right). The thrombus may eventually resorb as a result of endogenous or therapeutic thrombolysis. However, a wound healing response triggered by thrombin generated during blood coagulation can stimulate smooth muscle proliferation. Platelet-derived growth factor (PDGF) released from activated platelets stimulates smooth muscle cell migration. Transforming growth factor- (TFG-), also released from activated platelets, stimulates interstitial collagen production. This increased migration, proliferation and extracellular matrix synthesis by smooth muscle cells thickens the fibrous cap and causes further expansion of the intima, often now in an inward direction, yielding constriction of the lumen. Stenotic lesions produced by the lumenal encroachment of the fibrosed plaque may restrict flow, particularly under situations of increased cardiac demand, leading to ischaemia, commonly provoking symptoms such as angina pectoris. Advanced stenotic plaques, being more fibrous, may prove less susceptible to rupture and renewed thrombosis. Lipid lowering can reduce lipid content and calm the intimal inflammatory response, yielding a more 'stable' plaque with a thick fibrous cap and a preserved lumen (centre). Nature 420, (19 December 2002); doi: /nature01323 <> Inflammation in atherosclerosis PETER LIBBY Pos. Family History Hypertension DM Smoking Obesity Inactivity HIV ? HIV remmers? Statins Hygienic measures Adapted from P. Libby, Nature 2002, 420,
 and the accumulation of lipids leads to formation of a lipid-rich core, as the artery enlarges in an outward, ablumenal direction to accommodate the expansion of the intima. If inflammatory conditions prevail and risk factors such as dyslipidaemia persist, the lipid core can grow, and proteinases secreted by the activated leukocytes can degrade the extracellular matrix, while pro-inflammatory cytokines such as interferon- (IFN-) can limit the synthesis of new collagen. These changes can thin the fibrous cap and render it friable and susceptible to rupture. When the plaque ruptures, blood coming in contact with the tissue factor in the plaque coagulates. Platelets activated by thrombin generated from the coagulation cascade and by contact with the intimal compartment instigate thrombus formation. If the thrombus occludes the vessel persistently, an acute myocardial infarction can result (the dusky blue area in the anterior wall of the left ventricle, lower right). The thrombus may eventually resorb as a result of endogenous or therapeutic thrombolysis. However, a wound healing response triggered by thrombin generated during blood coagulation can stimulate smooth muscle proliferation. Platelet-derived growth factor (PDGF) released from activated platelets stimulates smooth muscle cell migration. Transforming growth factor- (TFG-), also released from activated platelets, stimulates interstitial collagen production. This increased migration, proliferation and extracellular matrix synthesis by smooth muscle cells thickens the fibrous cap and causes further expansion of the intima, often now in an inward direction, yielding constriction of the lumen. Stenotic lesions produced by the lumenal encroachment of the fibrosed plaque may restrict flow, particularly under situations of increased cardiac demand, leading to ischaemia, commonly provoking symptoms such as angina pectoris. Advanced stenotic plaques, being more fibrous, may prove less susceptible to rupture and renewed thrombosis. Lipid lowering can reduce lipid content and calm the intimal inflammatory response, yielding a more stable plaque with a thick fibrous cap and a preserved lumen (centre). Nature 420, (19 December 2002); doi: /nature <> Inflammation in atherosclerosis. PETER LIBBY. Pos. Family History. Hypertension. DM. Smoking. Obesity. Inactivity. HIV HIV remmers Statins. Hygienic. measures. Adapted from P. Libby, Nature 2002, 420,")
43
Atherosclerotic Lesion in a Human Artery
Panel A shows a cross-sectioned coronary artery from a patient who died of a massive myocardial infarction. It contains an occlusive thrombus superimposed on a lipid-rich atherosclerotic plaque. The fibrous cap covering the lipid-rich core has ruptured (area between the arrows), exposing the thrombogenic core to the blood. Trichrome stain was used, rendering luminal thrombus and intraplaque hemorrhage red and collagen blue. Panel B is a high-power micrograph of the area in Panel A indicated by the asterisk and shows that the contents of the atheromatous plaque have seeped through the gap in the cap into the lumen, suggesting that plaque rupture preceded thrombosis (the asterisk indicates cholesterol crystals). (Panels A and B courtesy of Dr. Erling Falk, University of Aarhus, Aarhus, Denmark.) Panel C illustrates the consequences of the activation of immune cells in a coronary plaque. Microbes, autoantigens, and various inflammatory molecules can activate T cells, macrophages, and mast cells, leading to the secretion of inflammatory cytokines (e.g., interferon- and tumor necrosis factor) that reduce the stability of plaque. The activation of macrophages and mast cells also causes the release of metalloproteinases and cysteine proteases, which directly attack collagen and other components of the tissue matrix. These cells may also produce prothrombotic and procoagulant factors that directly precipitate the formation of thrombus at the site of plaque rupture. Figure 1. Atherosclerotic Lesion in a Human Artery. N Engl J Med 2005; 352:
, exposing the thrombogenic core to the blood. Trichrome stain was used, rendering luminal thrombus and intraplaque hemorrhage red and collagen blue. Panel B is a high-power micrograph of the area in Panel A indicated by the asterisk and shows that the contents of the atheromatous plaque have seeped through the gap in the cap into the lumen, suggesting that plaque rupture preceded thrombosis (the asterisk indicates cholesterol crystals). (Panels A and B courtesy of Dr. Erling Falk, University of Aarhus, Aarhus, Denmark.) Panel C illustrates the consequences of the activation of immune cells in a coronary plaque. Microbes, autoantigens, and various inflammatory molecules can activate T cells, macrophages, and mast cells, leading to the secretion of inflammatory cytokines (e.g., interferon- and tumor necrosis factor) that reduce the stability of plaque. The activation of macrophages and mast cells also causes the release of metalloproteinases and cysteine proteases, which directly attack collagen and other components of the tissue matrix. These cells may also produce prothrombotic and procoagulant factors that directly precipitate the formation of thrombus at the site of plaque rupture. Figure 1. Atherosclerotic Lesion in a Human Artery. N Engl J Med 2005; 352:")
44
Pathofysiologie Voornaamste oorzaken AP:
Atherosclerotische stenose (fixed / stable plaque) Coronair spasme (atherosclerotische plaque)
 Coronair spasme (atherosclerotische plaque)")
45
Pathofysiologie Overige oorzaken AP:
Refractair coronair spasme (cocaïne, allergische reactie) CO-intoxicatie (koolstofmono-oxide) Anemie (!) Hypoxaemie door welke oorzaak dan ook
 CO-intoxicatie (koolstofmono-oxide) Anemie (!) Hypoxaemie door welke oorzaak dan ook.")
46
Risicofactoren

47
Klachten en symptomen Pijn op de borst: - drukkend/snoerend/bandvormig
- uitstraling (li>re) arm of kaak - inspanningsgebonden - goede reactie op NTG Dyspnoe - als POB equivalent - Als gevolg van pompfalen Vegetatieve verschijnselen?: - Vrijwel nooit
 arm of kaak. - inspanningsgebonden. - goede reactie op NTG. Dyspnoe - als POB equivalent. - Als gevolg van pompfalen. Vegetatieve verschijnselen : - Vrijwel nooit.")
48
Klachten en symptomen Complicaties bij AP: Ritme/geleidingstoornissen
Verminderde LV functie door ischemie. Decompensatio cordis CAVE Asthma cardiale (m.n. bij patiënten met een reeds pre-existent gecompromitteerde LV functie.)
")
49
Diagnostiek De Anamnese is de hoeksteen van de diagnostiek bij AP!! (inspanningsgebonden POB?) ECG (ST elevaties/depressies/T-top inversie) Lab: uitsluiten ACS/AMI (Troponine T/I, CK-MB etc.)
")
50
Diagnostiek Polikliniek Anamnese (inspanningsgebonden POB) ECG
Inspanningstesten (uitlokken klachten) X-ECG MIBI scan dobutamine echo
 X-ECG. MIBI scan. dobutamine echo.")
51
Diagnostiek - Klacht - ECG

52
Diagnostiek Dobutamine/inspannings MIBI

53
Diagnostiek Dobutamine/inspannings MIBI

54
Therapie Doel therapie - optimaliseren balans tussen demand en supply
Verbeteren supply - voorkomen thrombusvorming op stenose - ASA(Ascal)/Clopidogrel(Plavix) remt plaatjesaggregatie - ‘remmen’ progressie stenose(s) - Statine (cholesterol , verbeteren endotheeldysfunctie) - voorkomen vaatspasmen met Ca-antagonisten
/Clopidogrel(Plavix) remt plaatjesaggregatie. - ‘remmen’ progressie stenose(s) - Statine (cholesterol , verbeteren endotheeldysfunctie) - voorkomen vaatspasmen met Ca-antagonisten.")
55
Therapie Verminderen demand - vertragen hartfrequentie: beta-blokkade
- bestrijden hypertensie: nitraten, beta-blokkade, ACE - verminderen contractiliteit: beta-blockade, nitraten (preload )
")
56
Therapie Refractaire AP (medicatie schiet tekort)
Revascularisatie procedures: - PTCA - CABG Revascularisatie onmogelijk - anatomie coronairen accepteren en evt. pijn behandelen - Angiogenese - Transmyocardiale laser revascularisatie (TMLR) - TENS (transcutane electrische neurostimulatie) - Medicatie toevoegen : bv. Vastarel, Nicorandil, etc.
 - TENS (transcutane electrische neurostimulatie) - Medicatie toevoegen : bv. Vastarel, Nicorandil, etc.")
57
Dus.... Myocardinfarct Non-Q-wave infarct Instabiele Angina pectoris
3 uitingen van in principe dezelfde ziekte Coronarialijden Syndroom geen medische diagnose, maar Aangezien zelfde ziekte, gevat onder 1 noemer: Acuut coronair syndroom Alleen door de voortschrijdende techniek 3 verschillende namen,

58
Risicofactoren voor atherosclerose
Leeftijd Mannelijk geslacht Positieve familie anamnese Verhoogd cholesterol Diabetes Mellitus Overgewicht Roken! HIV?

59
Klachten Drukkende pijn op de borst
Uitstralend naar de kaak of linker arm Bij IAP toename bij inspanning Niet houdingsafhankelijk Neemt niet toe bij druk op thorax Misselijkheid, braken, transpireren Bij IAP reactie op NTG Benauwdheid (bij decompensatie) Collaps (bij ritmestoornissen) Misselijkheid, braken en transpireren met name bij Infarct
 Collaps (bij ritmestoornissen) Misselijkheid, braken en transpireren met name bij Infarct.")
60
Lichamelijk onderzoek
Bleek, zweterig (met name bij infarct) Doodsangst (met name bij infarct) Bloeddruk vaak afwijkend Pols kan afwijkend zijn (ritmestoornis) Koorts na infarct (38º) Gewichts toename (bij decompensatie)
 Doodsangst (met name bij infarct) Bloeddruk vaak afwijkend. Pols kan afwijkend zijn (ritmestoornis) Koorts na infarct (38º) Gewichts toename (bij decompensatie)")
61
Beleid: NTG (iv) Ascal Heparine Telemetrie / CCU
Bij infarct: eventueel trombolyse eventueel Primaire PTCA Ischaemie detectie

62
Beleid: Preventie!!!! Stoppen met roken Minder vet eten
Bij DM suiker goed reguleren Afvallen Medicatie: Simvastatine Ascal Β-blokker

63
Myocardinfarct

64
Definitie Acuut myocard infarct
Acute en irreversibele beschadiging van (een deel van) de hartspier ten gevolge van het tekort schieten van de bloedtoevoer, leidend tot necrose en verlittekening van het desbetreffende deel van het myocard.
 de hartspier ten gevolge van het tekort schieten van de bloedtoevoer, leidend tot necrose en verlittekening van het desbetreffende deel van het myocard.")
65
Pathofysiologie Oorzaken AMI
- meestal thrombotische occlusie t.g.v. plaque ruptuur plaatjesaggregatie vasoactiva spasmen thrombine stollingsactivatie bevordering aggregatie

66
Pathofysiologie Oorzaken AMI - zelden: embolus (endocarditis!)
coronair spasme (cocaine, allergische reactie) CO-intoxicatie anemie hypoxaemie
 CO-intoxicatie. anemie. hypoxaemie.")
67
Pathofysiologie Plaque ruptuur

68
Pathofysiologie Grootte AMI
afhankelijk mate verstoring evenwicht demand-supply en hoe lang deze verstoring aanhoudt. supply: - plaats afsluiting - duur afsluiting - irreversibel na min ischemie - collaterale doorbloeding - (Hb, PO2) demand - zuurstof behoefte myocard - frequentie, RR, contractiliteit
 demand. - zuurstof behoefte myocard. - frequentie, RR, contractiliteit.")
69
Pathofysiologie Plaats afsluiting Groot Klein

70
Pathofysiologie Tijdsbeloop AMI begin infarcering: 20-30 min
volledig na ongeveer 6 uur NB: stuttering infarction: - afwisselend occlusie/reperfusie - geprotraheerd beloop ischemie meest uitgesproken endocardiaal infarcering endo epicard (uren)
")
71
Pathofysiologie Oud non-transmuraal infarct Oud transmuraal infarct
Hypertrofie Vers infarct

72
Klachten en symptomen Klachten door AMI zelf
Pijn op de borst: - drukkend/snoerend/bandvormig - uitstraling (li>re) arm of kaak - in rust onstaan (!0400 AM) - weinig of geen reactie NTG Vegetatieve verschijnselen: - misselijk, braken, transpiratie, gapen
 arm of kaak. - in rust onstaan (!0400 AM) - weinig of geen reactie NTG. Vegetatieve verschijnselen: - misselijk, braken, transpiratie, gapen.")
73
Klachten en symptomen Mogelijke gevolgen van AMI
Dyspneu: backward failure Shock: forward failure duizelig/collaps: ritme-/geleidingsstoornissen (VF!) CVA: LV thrombus/AF NB: frequent geen (duidelijke) klachten ouderen, diabetici!!
 CVA: LV thrombus/AF. NB: frequent geen (duidelijke) klachten ouderen, diabetici!!")
74
Diagnostiek ECG en AMI (evolutie)
")
75
Diagnostiek laboratorium
Enzymbepalingen Infarct = necrose Integriteit celmembraan verloren intracellulaire stoffen ontsnappen naar extracellulair biochemische markers van infarcering

76
Diagnostiek biochemische markers CK/creatine kinase: aspecifiek
CK-MB: myocardiale fractie (10% van CK = infarct) ASAT/aspartaat aminotransferase: aspecifiek LDH/lactaat dehydrogenase: aspecifiek Troponines: onderdeel contractie mechanisme spiercel (zeer gevoelig en specifiek)
 ASAT/aspartaat aminotransferase: aspecifiek. LDH/lactaat dehydrogenase: aspecifiek. Troponines: onderdeel contractie mechanisme spiercel (zeer gevoelig en specifiek)")
77
Diagnostiek

78
Diagnostiek Differentiaal diagnostiek Cardiaal
- Instabiele AP geen irreversibele schade klacht als bij AMI, vaak niet vegetatief vaak subendocardiaal:ST-depressie, neg T, wel reactie NTG - Pericarditis houdings- en ademhalingsafhankelijk ST-elevatie ‘all-over’; geen reciproke depressie

79
Diagnostiek Differentiaal diagnostiek Vasculair
- Aneurysma Dissecans ‘scheurende’ pijn tussen schouderbladen RR verschillen li/re arm; arm/been neurologische uitval!! - Longembolie sterke ademhalingsafhankelijkheid pijn, dyspneu meer uitgesproken, na bevalling, fractuur, immobilisatie, veneuze thrombose,CVD verhoogd, pleurawrijven, tachycardie rechter as, RBTB, SIQIIInegTIII

80
Diagnostiek Differentiaal diagnostiek Oesophagusspasme
reageert ook op NTG!!! Bovenbuikspathologie ouderen! (Inter)costaal Pathologie (Tietze)
costaal Pathologie (Tietze)")
81
Diagnostiek Diagnose hartinfarct vermoed als: - typische klachten
- typische ECG afwijkingen Diagnose hartinfarct bewezen als: - typisch beloop ECG afwijkingen - enzymen positief (CK 2x bovengrens normaal, CK-MB 10% hiervan, positieve Troponines)
")
82
Therapie “TIME IS MUSCLE”: snelheid is geboden
Doel therapie - herstelen balans tussen vraag en aanbod beperken infarctgrootte! “TIME IS MUSCLE”: snelheid is geboden “TIME TO REPERFUSION” bepaalt een groot deel van de prognose mogelijkheden thrombolyse en PCI

83
Therapie ‘time is muscle!’

84
Therapie Verbeteren supply: - zuurstof per neusssonde
- doorgankelijkheid coronair herstellen (reperfusie) - Ascal remt plaatjesaggregatie - chemische recanalisatie: i.v. Thrombolyse - mechanische recanalisatie: PTCA - inotropie, I.A.B.P. bij cardiogene shock
 - Ascal remt plaatjesaggregatie. - chemische recanalisatie: i.v. Thrombolyse. - mechanische recanalisatie: PTCA. - inotropie, I.A.B.P. bij cardiogene shock.")
85
Therapie Verminderen demand: - vertragen hartfrequentie: beta-blokkade
- bestrijden hypertensie: nitraten, beta-blokkade - pijnbestrijding/sedatie: Fentanyl - bedrust

86
Therapie Recanalisatie Algemeen < 3 h: 50 % risk area gered
“TIME IS MUSCLE!” Pre-thrombolyse tijdperk: Hartcatheterisatie: (De Wood et al.1980, De Feyter et al. 1982) 4 uur na infarct: 87% occlusie 1 dag - 8 wkn: 65% occlusie
 4 uur na infarct: 87% occlusie. 1 dag - 8 wkn: 65% occlusie.")
87
Therapie Keuze Thrombolyse versus P.C.I. PTCA ‘waarschijnlijk’ superieur Uiteindelijke keuze afhankelijk : winst vs. risico logistiek financiën Situatie regio Amsterdam: Indien klachten <6 uur P.C.I. LIFENET

88
Therapie PTCA vs Thrombolysis Korte termijn Keeley, The Lancet 2003

89
Therapie PTCA vs Thrombolysis lange termijn Keeley, The Lancet 2003

90
PCI

91
Nejm site

92
Reperfusie ECG en ST resolutie > 70% resolutie 30 - 70% resolutie

93
Therapie Basistherapie Aspirine, betablockers + statines Eventueel ACE remmers: (verwacht) hartfalen Diuretica: idem Antiarrhytmica: bij (ventriculaire) aritmie Antistolling: bij bewezen LV thrombus of profylactisch bij slechte LV restfunctie Nitraten: (post AMI) angina pectoris
 aritmie. Antistolling: bij bewezen LV thrombus of profylactisch bij slechte LV restfunctie. Nitraten: (post AMI) angina pectoris.")
94
Therapie

95
Therapie

96
Onderhoudstherapie

97
Therapie Controversieel Tevens Antistolling: iedereen post AMI
Ca blockers: Oversterfte? Digoxine: falen - alleen effect aantal heropnamen Tevens Stoppen met roken Hypertensie behandelen Diabetes goed regelen Overgewicht bestrijden

98
Vragen????

Verwante presentaties




 bij ROW>")








 overgewicht.>")




>")

