Download de presentatie
De presentatie wordt gedownload. Even geduld aub

1
Verslaving Nieuwe Inzichten vanuit Wetenschappelijk Onderzoek: Richting voor de Praktijk
Wim van den Brink Amsterdam Institute for Addiction Research Academisch Medisch Centrum Universiteit van Amsterdam Verslaving en Zorg 3, Ede, 15 januari 2008

2
Inhoudsopgave Wat zijn verslavende stoffen? Wat is verslaving?
Hoe kijken we naar verslaafden? Verslaving een hersenziekte? Verslaving een behandelbare hersenziekte! Conclusies

3
Wat zijn Verslavende Stoffen?

4
Geneesmiddel, Drug of Doping

5
Geneesmiddel, Drug of Doping

6
Geneesmiddel, Drug of Doping
Viagara

7
Drug of Voeding

8
Wat zijn verslavende stoffen?
Stoffen met een belonend karakter, dwz stoffen die je een goed/aangenaam gevoel geven (EUFORIE) Stoffen waar mensen als ze ze eenmaal hebben gehad bij voortduring aan moeten denken (CRAVING) Stoffen waar sommige mensen als ze het eenmaal kennen niet meer vanaf kunnen blijven (CONTROLEVERLIES) “Het water loopt in je mond”
 Stoffen waar mensen als ze ze eenmaal hebben gehad bij voortduring aan moeten denken (CRAVING) Stoffen waar sommige mensen als ze het eenmaal kennen niet meer vanaf kunnen blijven (CONTROLEVERLIES) Het water loopt in je mond")
9
Wat is Verslaving?

10
Wat is essentieel voor Verslaving?
Tolerantie Zie je eigenlijk bij de meeste stoffen en geneesmiddelen Onthoudingsverschijnselen Craving Specifiek voor verslavende stoffen en voor verslaving “Het water loopt in je mond” CONTROLEVERLIES AFHANKELIJKHEID

11
Misbruik, Afhankelijkheid, Verslaving
Gebruik dat kan leiden of heeft geleid tot psychologische of maatschappelijke problemen Afhankelijkheid Ongecontroleerd gebruik van middelen ten gevolge van hunkering en/of onthoudingsverschijnselen dat heeft geleid tot lichamelijke, psychische en/of sociale problemen Verslaving Afhankelijkheid met geautomatiseerd gebruik van middelen dat niet gemakkelijk gestopt kan worden en waarvoor professionele hulp moet worden ingeroepen of al is ingeroepen.

12
Hoe zit het met Gokken? Afhankelijkheid Pathologisch Gokken
Voortdurend verlangen Meer en langer gebruik Duidelijke tolerantie Onthoudingsverschijnselen Mislukte stoppogingen Interferentie met verplichtingen Verwaarlozing activiteiten Doorgaan met gebruik ondanks aantoonbare schade Pathologisch Gokken Preoccupatie met gokken Verspeelt meer geld Meer inzetten om zelfde effect Rusteloos/Geïrriteerd bij niet spelen Mislukte stoppogingen Interferentie met verplichtingen Opoffering activiteiten Doorgaan met gebruik ondanks duidelijke problemen Volgende dag terug om verlies goed te maken

13
Gokverslaving? (Potenza, 2006; Petry, 2006, Goudriaan et al., 2005)
Klinische kenmerken heel vergelijkbaar (Marks, 1990) (craving/compulsion; loss of control; continue despite adverse effects) Cognitieve stoornissen vergelijkbaar (Goudriaan et al., 2005) (deficient cortical judgement/planning (EF); deficient inhibition) Neurochemische afwijkingen vergelijkbaar (Roy et al, 1989) (NE abnormalities in CSF [related to extraversion]) Neuroimaging beelden vergelijkbaar (Potenza, 2003, 2004) (fMRI reactions to pictures; PET reactions to pictures) Vergelijkbaar efect van anti-craving medicijnen (Kim, 2006) (reduced urge to gamble following naltrexone treatment)
 (craving/compulsion; loss of control; continue despite adverse effects) Cognitieve stoornissen vergelijkbaar (Goudriaan et al., 2005) (deficient cortical judgement/planning (EF); deficient inhibition) Neurochemische afwijkingen vergelijkbaar (Roy et al, 1989) (NE abnormalities in CSF [related to extraversion]) Neuroimaging beelden vergelijkbaar (Potenza, 2003, 2004) (fMRI reactions to pictures; PET reactions to pictures) Vergelijkbaar efect van anti-craving medicijnen (Kim, 2006) (reduced urge to gamble following naltrexone treatment)")
14
Verslaving, Gewoonte of Hobby
middel, beloning gedrag, geheugen?

15
Hoe kijken we naar verslaafden?

16
Geschiedenis van Verslaving
Marlatt Jellinek Hoog Hullen Ideologie Empirie

17
Verslaving 1990-heden Hersenziekte model: 1990-nu (CGT and medicatie)
Charles O’Brien Hersenziekte model: 1990-nu (CGT and medicatie)
")
18
Verslaving een Hersenziekte

19
Aanwijzingen Hersenziekte
Genetische kwetsbaarheid Biologische risicofactoren Betrokkenheid van het brein: * initiatie opiaten (VTA) en dopamine (NcA), VStriatum * craving dopamine (NcA, Amygdala, AGC) (LIKING) * gewoontedrag dopamine, glutamaat (Putamen, NcCaudatus) DStriatum * stress noradrenaline (LC-HPA) (WANTING) * salience (importantie) dopamine (OFC) OFC * terugval glutamaat (AGC,PFC) DLPFC Effect van medicatie
 en dopamine (NcA), VStriatum. * craving dopamine (NcA, Amygdala, AGC) (LIKING) * gewoontedrag dopamine, glutamaat (Putamen, NcCaudatus) DStriatum. * stress noradrenaline (LC-HPA) (WANTING) * salience (importantie) dopamine (OFC) OFC. * terugval glutamaat (AGC,PFC) DLPFC. Effect van medicatie.")
20
Aanwijzingen Hersenziekte
Genetische kwetsbaarheid Biologische risicofactoren Betrokkenheid van het brein: * initiatie opiaten (VTA) en dopamine (NcA), VStriatum * craving dopamine (NcA, Amygdala, AGC) (LIKING) * gewoontedrag dopamine, glutamaat (Putamen, NcCaudatus) DStriatum * stress noradrenaline (LC-HPA) (WANTING) * salience (importantie) dopamine (OFC) OFC * terugval glutamaat (AGC,PFC) DLPFC Effect van medicatie
 en dopamine (NcA), VStriatum. * craving dopamine (NcA, Amygdala, AGC) (LIKING) * gewoontedrag dopamine, glutamaat (Putamen, NcCaudatus) DStriatum. * stress noradrenaline (LC-HPA) (WANTING) * salience (importantie) dopamine (OFC) OFC. * terugval glutamaat (AGC,PFC) DLPFC. Effect van medicatie.")
21
Erfelijkheid van Roken (Nederlandse Tweelingstudie: Vink en Boomsma, 2004)
Genetisch Gedeelde omgeving (SES) Unieke omgeving (vrienden) Experimenteren met roken 40% (chromosoom 6, 10, 14) 55% 5% Aantal sigaretten 50% (chromosoom 3, 10) 30% 20% Nicotine afhankelijkheid 75% 0% 25%
 Unieke omgeving. (vrienden) Experimenteren. met roken. 40% (chromosoom 6, 10, 14) 55% 5% Aantal sigaretten. 50% (chromosoom 3, 10) 30% 20% Nicotine afhankelijkheid. 75% 0% 25%")
22
Aanwijzingen Hersenziekte
Genetische kwetsbaarheid Biologische risicofactoren Betrokkenheid van het brein: * initiatie opiaten (VTA) en dopamine (NcA), VStriatum * craving dopamine (NcA, Amygdala, AGC) (LIKING) * gewoontedrag dopamine, glutamaat (Putamen, NcCaudatus) DStriatum * stress noradrenaline (LC-HPA) (WANTING) * salience (importantie) dopamine (OFC) OFC * terugval glutamaat (AGC,PFC) DLPFC Effect van medicatie
 en dopamine (NcA), VStriatum. * craving dopamine (NcA, Amygdala, AGC) (LIKING) * gewoontedrag dopamine, glutamaat (Putamen, NcCaudatus) DStriatum. * stress noradrenaline (LC-HPA) (WANTING) * salience (importantie) dopamine (OFC) OFC. * terugval glutamaat (AGC,PFC) DLPFC. Effect van medicatie.")
23
Bewust Fenotype Bewust/ Onbewust Endofenotype Onbewust/ Genotype
Alcoholism Bewust Bewust/ Onbewust Onbewust/ Fenotype Endofenotype Genotype Liability Alcoholism Alcoholism Spectrum Conditioning Attentional bias Low alcohol response Conflict Monitoring Disinhibition Reward Deficiency etc. candidate genes OPRM1 DRD1 COMT GRIN2B GABRA6 DRD2 SERT MAOA Ooteman et al (2006) adapted from Gottesman & Gould (2003) CNR1 HTR1B GABRB2 GABRG2
 adapted from Gottesman & Gould (2003) CNR1. HTR1B. GABRB2. GABRG2.")
24
Aanwijzingen Hersenziekte
Genetische kwetsbaarheid Biologische risicofactoren Betrokkenheid van het brein: * initiatie opiaten (VTA) en dopamine (NcA), VStriatum * craving dopamine (NcA, Amygdala, AGC) (LIKING) * gewoontedrag dopamine, glutamaat (Putamen, NcCaudatus) DStriatum * stress noradrenaline (LC-HPA) (WANTING) * salience (importantie) dopamine (OFC) OFC * terugval glutamaat (AGC,PFC) DLPFC Effect van medicatie
 en dopamine (NcA), VStriatum. * craving dopamine (NcA, Amygdala, AGC) (LIKING) * gewoontedrag dopamine, glutamaat (Putamen, NcCaudatus) DStriatum. * stress noradrenaline (LC-HPA) (WANTING) * salience (importantie) dopamine (OFC) OFC. * terugval glutamaat (AGC,PFC) DLPFC. Effect van medicatie.")
25
Fasen in het Verslavingsproces
Structuren Neurotransmitters Initiatie Anhedonie Ventral Tegmental Area (VTA) Nucleus Accumbens (NcA) Endorphines (-receptors) Dopamine Conditionering Craving Nucleus Accumbens (Ventrale Striatum) Amygdala Thalamus Prefrontal Cortex (OFC, ACC) Dynorphines (-receptors) CRH Glutamate Importantie Attentional Bias OFC Gewoontevorming Putamen, NcCaudatus (Dorsale Striatum) Disinhibitie Conflictregistratie Relapse DLPFC ACC Norepinephrine, 5HT GABA, Glutamate OnthoudingsSx Locus Ceruleus Norepinephrine Van den Brink, 2005, 2006; Van Ree, 2002; de Vries and Schippenberg, 2002; Kreek et al, 2002; Kosten and George, 2002; Koob, 2003
 Nucleus Accumbens (NcA) Endorphines (-receptors) Dopamine. Conditionering. Craving. Nucleus Accumbens (Ventrale Striatum) Amygdala. Thalamus. Prefrontal Cortex (OFC, ACC) Dynorphines (-receptors) CRH. Glutamate. Importantie. Attentional Bias. OFC. Gewoontevorming. Putamen, NcCaudatus (Dorsale Striatum) Disinhibitie. Conflictregistratie. Relapse. DLPFC. ACC. Norepinephrine, 5HT. GABA, Glutamate. OnthoudingsSx. Locus Ceruleus. Norepinephrine. Van den Brink, 2005, 2006; Van Ree, 2002; de Vries and Schippenberg, 2002; Kreek et al, 2002; Kosten and George, 2002; Koob,")
26
Decreased DA Binding in Corpus Striatum in Alcohol and Drug Addicts after Prolonged Abstinence Reward Deficiency?

27
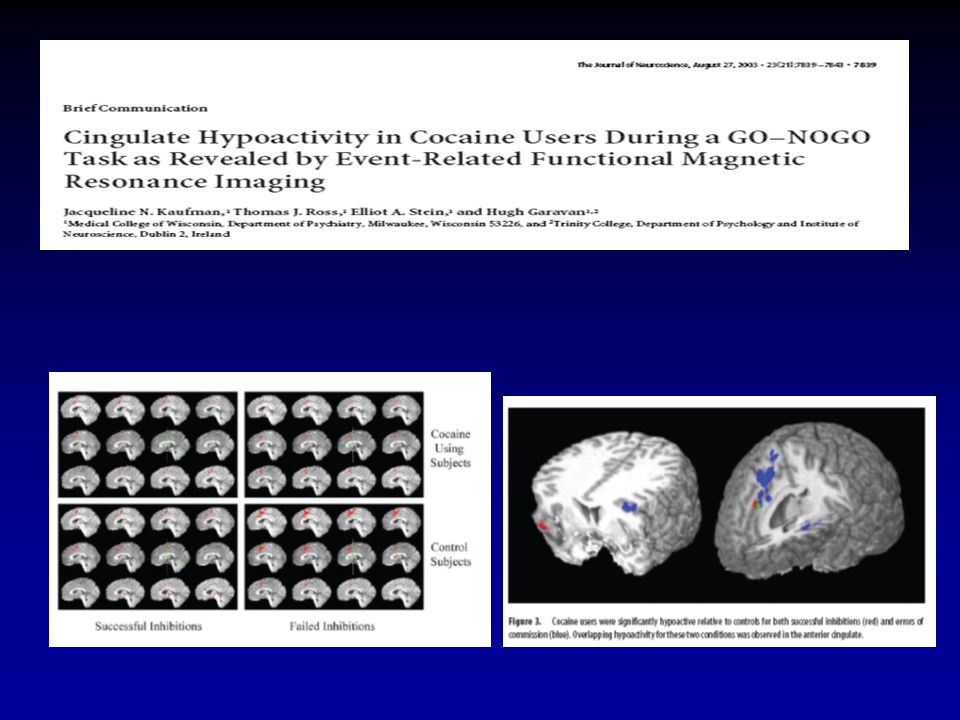
Prefrontal Cortex and ACC Under-Activity after Sustained Abstinence

28
Relation Striatal and Orbitofrontal Activity

29
I-RISA Model Impaired Response Inhibition and Salience Attribution
Goldstein and Volkow, 2002

30
I-RISA Model of Addiction Volkow (2004)
Control Control Salience Drive STOP Salience Drive GO Memory Memory Non-Addicted Brain Addicted Brain

31
Functioneel Model en Hersenstructuren
Volkow, 2006

32
Attentional Bias – Craving - Relapse

33
Attentional Bias – Craving - Relapse

35
Attentional Bias – Craving - Relapse

36
Attentional Bias-Cue-Reactivity-Craving-Relapse
Repeated Reward Detection Threshold Disinhibition Attentional Bias Cue-Reactivity Craving Relapse Conflict Registration

37
Verslaving een Behandelbare Hersenziekte Medicamenteuze Interventies

38
Medicamenteuze Interventies
Antagonist Anti-Craving Drug Cognitive Enhancer Agonist Naltrexone Acamprosate Modafinil Methadone Opioid dependence Alcohol dependence Cocaine dependence Repeated Reward Antagonists Agonists Detection Threshold Disinhibition Attentional Bias Cue-Reactivity Craving Relapse Conflict Registration Cognitive Enhancers Anti-Craving Drugs

39
Medicatie Nicotineafhankelijkheid
buproprion rimonabant nortryptyline varenicline

40
Alcohol Dependence Acamprosate Disulfiram Topiramate Naltrexone
Ondansetron

41
Alcoholdependence Repeated Reward Detection Threshold Disinhibition
Antagonist Agonist Detection Threshold Disinhibition Attentional Bias Cue-Reactivity Craving Relapse Conflict Registration Cognitive Enhancer Anti-Craving Drug

42
Naltrexon Pharmacogenetica Oslin et al, Neuropsychopharmacology, 2003
Δ = 30% Δ = 15% A/G, G/G =32% AA = 68%

43
Medicatie Cannabisafhankelijkheid
No effective medications available Hart (2005) Drug and Alcohol Dependence
 Drug and Alcohol Dependence.")
44
Medicatie Opiaatverslaving
Registration CBG-MEB buprenorphine methadone diacethylmorfine naltrexone buprenorphine + naloxone

45
Medicatie Cocaineverslaving
Nog geen bewezen-effective medicamenteuze behandeling beschikbaar Veelbelovend Disulfiram Modafinil Topiramate/Baclofen/Tiagabine Naltrexone Rimonabant Deep Brain Stimulation

46
Verslaving een Behandelbare Hersenziekte Neurofysiologische Interventies

47
Attentional Bias-Cue-Reactivity-Craving-Relapse
Repeated Reward Detection Threshold Disinhibition Attentional Bias Cue-Reactivity Craving Relapse Conflict Registration BioFeedback

48
Onderactiviteit ACC bij
volwassen ADHD patienten Hoe zit het bij verslaafden? Wat doet motiverende gespreksvoering op de activiteit van de ACC?

49
Go/No-Go Task

51
Effect EEG Biofeedback kinderen ADHD (Beauregard , Levesque, 2006) (Review: Holtmann en Stadler, 2006) ACC Thalamus Nc Caudatus Li Sup Parietaal ACC Nc Caudatus VLPFC EEG Biofeedback activatie ACC en Nc Caudatus bij sel. aandacht en mot. inhibitie taak EEG-Biofeedback activatie VLPFC bij motorische inhibitie taak EEG Biofeedback leidt ook tot betere gedragsprestaties op deze gebieden.

52
EEG Feedback and Addiction
Am J Drug Alcohol Abuse. 2005;31(3): Scott WC, Kaiser D, Othmer S, Sideroff SI Effects of an EEG biofeedback protocol on a mixed substance abusing population. This study examined whether an EEG biofeedback protocol could improve outcome measures for a mixed substance abusing inpatient population. METHOD: One hundred twenty-one volunteers undergoing an inpatient substance abuse program were randomly assigned to the EEG biofeedback or control group. EEG biofeedback included training in Beta and SMR to address attentional variables, followed by an alpha-theta protocol. Subjects received a total of 40 to 50 biofeedback sessions. The control group received additional time in treatment equivalent to experimental procedure time. The Test of Variables of Attention (TOVA), and MMPI, were administered with both tester and subject blind as to group placement to obtain unbiased baseline data. Treatment retention and abstinence rates as well as psychometric and cognitive measures were compared. RESULTS: Experimental subjects remained in treatment significantly longer than the control group (p <0.005). Of the experimental subjects completing the protocol, 77% were abstinent at 12 months, compared to 44% for the controls. Experimental subjects demonstrated significant improvement on the TOVA (p<.005) after an average of 13 beta-SMR sessions. Following alpha-theta training, significant differences were noted on 5 of the 10 MMPI-2 scales at the p<.005 level. CONCLUSIONS: This protocol enhanced treatment retention, variables of attention, and abstinence rates one year following treatment.
: Scott WC, Kaiser D, Othmer S, Sideroff SI. Effects of an EEG biofeedback protocol on a mixed substance. abusing population. This study examined whether an EEG biofeedback protocol could improve outcome measures for a mixed substance abusing inpatient population. METHOD: One hundred twenty-one volunteers undergoing an inpatient substance abuse program were randomly assigned to the EEG biofeedback or control group. EEG biofeedback included training in Beta and SMR to address attentional variables, followed by an alpha-theta protocol. Subjects received a total of 40 to 50 biofeedback sessions. The control group received additional time in treatment equivalent to experimental procedure time. The Test of Variables of Attention (TOVA), and MMPI, were administered with both tester and subject blind as to group placement to obtain unbiased baseline data. Treatment retention and abstinence rates as well as psychometric and cognitive measures were compared. RESULTS: Experimental subjects remained in treatment significantly longer than the control group (p <0.005). Of the experimental subjects completing the protocol, 77% were abstinent at 12 months, compared to 44% for the controls. Experimental subjects demonstrated significant improvement on the TOVA (p<.005) after an average of 13 beta-SMR sessions. Following alpha-theta training, significant differences were noted on 5 of the 10 MMPI-2 scales at the p<.005 level. CONCLUSIONS: This protocol enhanced treatment retention, variables of attention, and abstinence rates one year following treatment.")
53
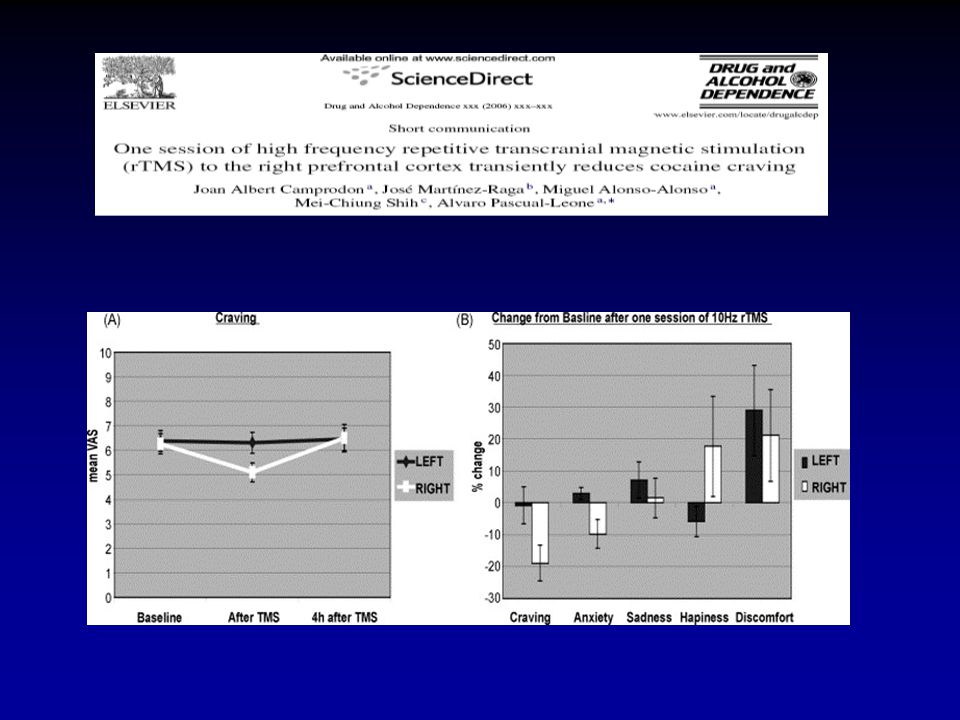
Attentional Bias - Cue-Reactivity - Craving –Relapse
Repeated Reward DBS rTMS Detection Threshold Disinhibition Attentional Bias Cue-Reactivity Craving Relapse Conflict Registration

55
Stimulation sites: [11C]raclopride PET measures of
Occipitaal en DLPFC dopamine release in Nc Caudatus
![Stimulation sites: [11C]raclopride PET measures of](http://slideplayer.nl/slide/4832982/15/images/55/Stimulation+sites%3A+%5B11C%5Draclopride+PET+measures+of.jpg "Occipitaal en DLPFC dopamine release in Nc Caudatus.")
56
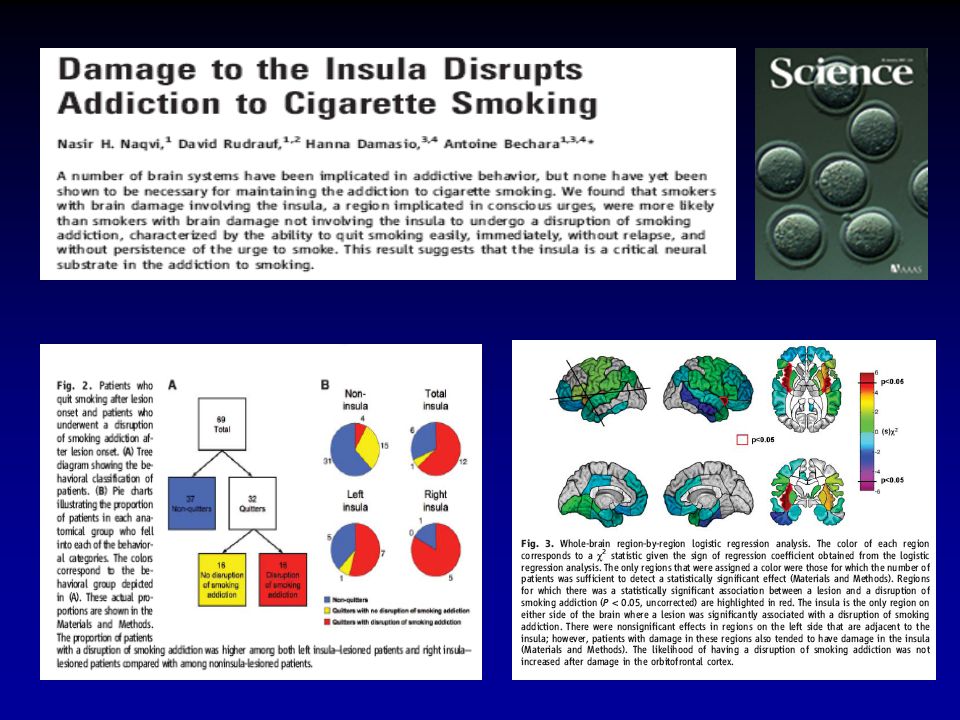
Clinical study for alleviating opiate drug psychological dependence by a method of ablating the nucleus accumbens with stereotactic surgery. Gao et al., 2003 Department of Neurosurgery, Tangdu Hospital, Fourth Military Medical University, Xian, China. Wayne Hall, 2006

58
Verslaving een Behandelbare Hersenziekte Psychosociale Interventies

59
Mesa Grande- Alcohol (Miller & Wilbourne, 2003)
systematische review 361 gecontroleerde studies; 538 contrasten; patiënten elke studie gescoord op kwaliteit (MQS: 0 tot 17: >13 = excellent) Elke studie gescoord op effectiviteit (OLS: -2 tot +2) Elk type interventie gescoord op bewezen effectiviteit (CES) Type interventies gerangschikt naar CES in “mesa grande” MQS= Methodological Quality Score; OLS = Outcome Logic Score; CES = Cumulative Evidence Score
 Elke studie gescoord op effectiviteit (OLS: -2 tot +2) Elk type interventie gescoord op bewezen effectiviteit (CES) Type interventies gerangschikt naar CES in mesa grande MQS= Methodological Quality Score; OLS = Outcome Logic Score; CES = Cumulative Evidence Score.")
60
Effectieve Interventies (>3 studies)
INTERVENTIE/RANGORDE CES % pos N studies Gem. MQS % Klinisch 01 Korte interventie 280 68 31 12.7 48 02 Motiverende interventie 173 71 17 13.1 53 03 Acamprosaat 116 100 5 11.6 04 Naltrexon 83 6 11.3 05 Sociale vaardigheidstraining 85 25 10.5 84 06 CRA 80 4 13.0 07 Gedragscontracten (CM) 64 10.4 08 Gedragstherap relatietherapie 60 62 8 12.9 09 Case management 33 67 10.2 10 Selfcontrole 50 12.0 11 Cognitieve therapie 21 40 10 10.0 88 12 Rogeriaanse counseling 20 57 7 10.6 86 13 Disulfiram 24 10.8 14 Aversietherapie (apnoe) 18 3 9.7 15 Covert sensitisation 38 10.9 16 Acupunctuur 14 17 Aversietherapie (misselijkheid) 18 Bibliotherapie 11 19 Zelfcontrole training 9 49 35 12.8 63
 Gedragstherap relatietherapie Case management Selfcontrole Cognitieve therapie Rogeriaanse counseling Disulfiram Aversietherapie (apnoe) Covert sensitisation Acupunctuur Aversietherapie (misselijkheid) 18 Bibliotherapie Zelfcontrole training")
61
Niet-Effectieve Interventies (>3 studies)
INTERVENTIE/RANGORDE CES % pos N studies Gem. MQS % Klinisch 46 Educatieve films en groepen -343 27 23 8.7 38 45 Algemene alcoholcounseling -239 10 20 11.2 85 44 Inzichtgevende psychotherapie -225 11 18 10.9 88 43 Confronterende counseling -190 10.7 73 42 Ontspanningsoefeningen -144 17 10.6 66 39 AA -108 14 7 86 38 Milieutherapie -107 12 100 37 TCA -104 6 35 Terugvalpreventie -87 30 11.9 34 Anxiolytica -80 29 8.4 33 5-HT antagonist -68 3 11.3 30 Hypnose -41 4 10.3 29 Functionele analyse -36 12.0 28 Relatietherapie (anders) -33 8 12.3 27 Lithium -32 43 11.4 26 SSRI -16 53 15 8.6 25 12 step facilitatie -13 33 23 Gezinstherapie -4 20 Minnesota model -3
 Lithium SSRI step facilitatie Gezinstherapie Minnesota model. -3.")
62
Verslaving een Hersenziekte Gevolgen voor Psychotherapie
Anhedonie Kunnen alternatieve activiteiten wel bevredigend worden? Wat is effectieve component van CRA? (Roozen et al, 2005). * Mogelijkheden CM met vouchers? Hoogte en aard van de beloning? Craving Werkt cue-exposure therapie wel bij stimuli die niet aversief zijn en waar geen bijstelling van cognities plaatsvindt. (Marissen, 2005)? * CET plus CBT en/of plus medicatie? (Ressler et al., 2004) * Anticraving medicatie plus psychotherapie? (Roozen et al., 2006) Attentional Bias Impliciete processen die aleen via unbewuste technieken kunnen worden aangepakt * Vermindering attentional bias (Field en Eastwood, 2005; Wiers et al 2006) Gewoontegedrag Niet bewust, moeilijk te controleren. * Biofeedback, DBS? Disinhibitie Vaardigheidstraining ter vermindering van impulsiviteit, maar zelfrapportage niet erg betekenisvol (Goudriaan et al., 2005). * Medicatie: modafinil, SSRI, dexamfetamine? * Biofeedback?
. * Mogelijkheden CM met vouchers Hoogte en aard van de beloning Craving. Werkt cue-exposure therapie wel bij stimuli die niet aversief zijn en waar geen. bijstelling van cognities plaatsvindt. (Marissen, 2005) * CET plus CBT en/of plus medicatie (Ressler et al., 2004) * Anticraving medicatie plus psychotherapie (Roozen et al., 2006) Attentional Bias. Impliciete processen die aleen via unbewuste technieken kunnen worden. aangepakt. * Vermindering attentional bias (Field en Eastwood, 2005; Wiers et al 2006) Gewoontegedrag. Niet bewust, moeilijk te controleren. * Biofeedback, DBS Disinhibitie. Vaardigheidstraining ter vermindering van impulsiviteit, maar zelfrapportage. niet erg betekenisvol (Goudriaan et al., 2005). * Medicatie: modafinil, SSRI, dexamfetamine * Biofeedback")
63
Verslaving een Behandelbare Hersenziekte Psychiatrische Comorbiditeit

64
Psychiatrische Comorbiditeit
Addiction and Schizophrenia: Classical, Atypical or just Clozapine Addiction and ADHD: No Medication, Methylphenidate or Atomoxetine Alcohol and Depression: SSRIs, but not in ealy onset alcoholics Alcohol and Anxiety: Buspirone is not recommended Alcohol and PTSD: Topiramate(?) Opioids and Depression: no SSRIs but imipramine Depression and Nicotine: Bupropion? Bipolar and Alcohol: Valproate?
 Opioids and Depression: no SSRIs but imipramine. Depression and Nicotine: Bupropion Bipolar and Alcohol: Valproate")
65
Conclusies

66
Conclusies Verslaving is een behandelbare hersenziekte
Kernsymptoom van verslaving is craving met controlverlies Medicatie en farmacogenetica zullen steeds belangrijker worden Neurofysiologische interventies voor jongeren en resistenten? Psychotherapie minder nadruk op inzicht en meer op training Therapietrouw en rehabilitatie blijven van groot belang

Verwante presentaties


 Topics:>")













>")



