Download de presentatie
De presentatie wordt gedownload. Even geduld aub

1
wervelkolom immobilisatie
Refereren chi-seh Mark van Zanten Aios seh

2
LPA 8 (Landelijk protocol ambulancezorg)
")
3
Achtergrond Uit het oogpunt LPA8
Wat te verwachten na 1 januari Hoe te handelen hospitaal Discussie

4
Casus Traumachirurg, +/- 45 jaar, feestje oud&nieuw
Bij invoegen A9 auto vs auto Beklemd BZV onduidelijk Enkele glazen champagne Bij ambulance goed aanspreekbaar, echter zeer opstandig, wil niet op een plank ‘help mij uit de auto, ik heb verder niks’

5
1) Indicatie wervelkolom immobilisatie 2) Geen indicatie wervelkolom immobilisatie
?
6
NB: Hoog energetisch trauma op zich is geen indicatie om te immobiliseren

7
Manueel / kraag / auto knippen en uit laten stappen?

8
?

10
NEXUS (National Emergency X-radiography utilization study)
Geen drukpijn CWK, en Geen tekenen intoxicatie, en Geen verlaagd bewustzijn, en Geen focale neurologische verschijnselen, en Geen pijnlijk afleidend letsel Test Sensitivity: 99.6% Test Specificity: 12.9% Negative Predictive Value: 99.9% Hoffman JR, Wolfson AB, Todd K, Mower WR. Selective cervical spine radiography in blunt trauma: methodology of the National Emergency X-Radiography Utilization Study (NEXUS). Ann Emerg Med Oct;32(4):461-9.
. Ann Emerg Med Oct;32(4):")
11
Canadian c-spine Test Sensitivity: 99.4-100%
Test Specificity: % Negative Predictive Value: 100% Canadian CT Head and C-Spine (CCC) Study Group. Canadian C-Spine Rule study for alert and stable trauma patients: I. Background and rationale. CJEM Mar;4(2):84-90.
 Study Group. Canadian C-Spine Rule study for alert and stable trauma patients: I. Background and rationale. CJEM Mar;4(2):")
12
N Engl J Med Dec 25;349(26): The Canadian C-spine rule versus the NEXUS low-risk criteria in patients with trauma. Stiell IG1, Clement CM, McKnight RD, Brison R, Schull MJ, Rowe BH, Worthington JR, Eisenhauer MA, Cass D, Greenberg G, MacPhail I, Dreyer J, Lee JS, Bandiera G, Reardon M, Holroyd B, Lesiuk H, Wells GA. For alert patients with trauma who are in stable condition, the CCR is superior to the NLC with respect to sensitivity and specificity for cervical-spine injury, and its use would result in reduced rates of radiography.

13
Enkele ‘hoogtepunten’
‘Alerte patiënten die drukpijn aangeven cervicaal, kunnen mogelijk het beste zelf uitstappen’ ‘vervoer bij voorkeur op vacuummatras’ ‘Behoud bij alerte patiënt voorkeurshouding; dus ook halfzittend vervoer’ ‘wetenschappelijke meerwaarde volledige wervelkolommobilisatie is niet aangetoond’ ‘neurologische outcome niet verbeterd’ ‘Nadelen; angst/onrust, decubitus, aspiratie, resp insuff’ ‘ICP stijging door compressie vv jugularis interna’ ‘bij gebruik nekspalk reductie mondopening 20-25%’ ‘geen evidence dat cervicale WK extra geimmobiliseerd wordt door headblocks en kraag tegelijk’ ‘aanleggen spalk bij kinderen dient achterwege te worden gelaten, onvoldoende rekening met wisselende anatomie’

14
Evidence?

16
Emerg Med J. 2013;30(1067-9) Pre-hospital spinal immobilisation: an initial consensus statement. Connor et al. Beschreven consensus

17
Emerg Med J Feb;29(2):104-7 Value of a rigid collar in addition to head blocks: a proof of principle study. Holla M. 10 vrijwilligers Digitale meting nekkraag vs headblocks Maximale mondopening Geen extra immobillisatie Mondopening significant verminderd bij nekkraag

18
Emerg Med J Dec; 30(12): Minimal patient handling: a faculty of prehospital care consensus statement Moss R, Porter K (UK) Beschreven consensus

19
Journal of neurotrauma. March 2014;31:531-540
Journal of neurotrauma. March 2014;31: Prehospital Use of cervical collars in trauma patients: a critical review. Terje Sundstrom et al.

20
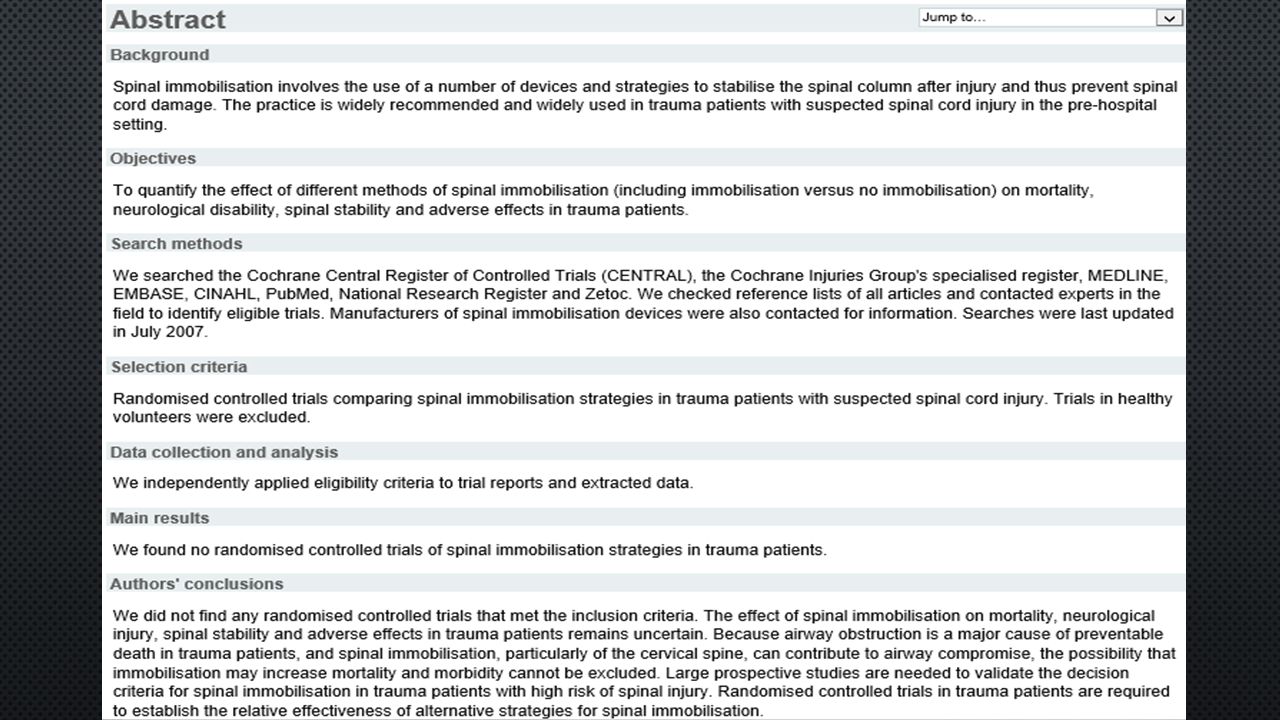
Introductie Al 30 jr ongewijzigd beleid, 50-60 landen
Kragen ter preventie secundair letsel Cochrane 2007: RCT missen, onbekende effecten op mortaliteit/neurologische schade Literature search; 50 artikelen + expert opinion

22
Doel evidence voor immobilisatie is mogelijk zwak, is er evidence voor adverse effects?

23
Enkele cijfers… 2-4% traumapatienten met CWK letsel, waarvan 20% SCI
Delayed of missed diagnose 1.3% Incidentie wervelfracturen 12:100000 Fall of motor vehicle accident

24
En verder… Medicolegaal Voelt verstandig Symbool hoge kwaliteit zorg
Relatief makkelijk eenduidig protocol

25
Effectief? 3-25% SCI is secundair
-moeilijk testen neurologische uitval in prehospitale setting -extrapolatie bevindingen zkh naar prehospitaal -gedateerd Theodore et al neurosurgery Bell et al Spine J. Sundheim et al Ann. Emerg. Med.

26
BETERE IMMOBILISATIE KRAAG + PLANK EN HEADBLOCKS JUIST/ONJUIST
BETERE IMMOBILISATIE BIJ KRAAG VS GEEN KRAAG JUIST/ONJUIST KRAAG/VACUUM VS KRAAG/PLANK ?

27
Emerg Med J Feb;29(2):104-7 Value of a rigid collar in addition to head blocks: a proof of principle study. Holla M. 10 vrijwilligers Digitale meting nekkraag vs headblocks Maximale mondopening Geen extra immobillisatie Mondopening significant verminderd bij nekkraag

28
Conrad et al. Motion in the unstable cervical spine during hopsital bed transfers. J. Trauma 2010: 69; METHODS: Cervical spine instability was created at C5-C6 in cadavers. manual transfer performed by six trained individuals and a transfer made by two people using the On3 lateral transfer device. Both techniques were tested under four collar conditions. Cervical spine motion was measured using an electromagnetic motion analysis device with sensors fixed to the anterior bodies of C5 and C6. RESULTS: No significant differences were observed (flexion, [p = 0.325]; axial rotation [p = 0.590]; lateral bending [p = 0.112]). Nor were there significant differences among the three collars used (flexion [p = 0.462]; axial rotation [p = 0.434]; lateral bending [p = 0.250]). For all transfers, using no collar resulted in more motion than using a collar; but was not statistically significant.
. Nor were there significant differences among the three collars used (flexion [p = 0.462]; axial rotation [p = 0.434]; lateral bending [p = 0.250]). For all transfers, using no collar resulted in more motion than using a collar; but was not statistically significant.")
29
Luscombe et al. Comparison of a long spinal board and vacuum splints for cervical spine immobilization. Ann. Emerg. Med. 1992:21( ) METHODS: Nine volunteers wearing standardised clothing and rigid neck collars were secured on to a backboard and vacuum mattress An operating department table was used to tilt the volunteers from 45 degrees head up to 45 degrees head down, and additionally 45 degrees laterally. Movements of the head, sternum, and pubic symphysis (pelvis) from a fixed position were then recorded. The comfort level during the procedure was assessed using a 10 point numerical rating scale (NRS) where 1=no pain and 10=worst pain imaginable. RESULTS: The mean body movements in the head up position (23.3 v 6.66 mm), head down (40.89 v 8.33mm), and lateral tilt (18.33 v 4.26mm) were significantly greater on the backboard than on the vacuum mattress (p<0.01 for all planes of movement). Using the NRS the vacuum mattress (mean score=1.88) was significantly more comfortable than the backboard (mean score=5.22) (p<0.01). CONCLUSIONS: In the measured planes the vacuum mattress provides significantly superior stability and comfort than a backboard.
 from a fixed position were then recorded. The comfort level during the procedure was assessed using a 10 point numerical rating scale (NRS) where 1=no pain and 10=worst pain imaginable. RESULTS: The mean body movements in the head up position (23.3 v 6.66 mm), head down (40.89 v 8.33mm), and lateral tilt (18.33 v 4.26mm) were significantly greater on the backboard than on the vacuum mattress (p<0.01 for all planes of movement). Using the NRS the vacuum mattress (mean score=1.88) was significantly more comfortable than the backboard (mean score=5.22) (p<0.01). CONCLUSIONS: In the measured planes the vacuum mattress provides significantly superior stability and comfort than a backboard.")
30
Toegenomen frequentie neurologische schade.
Adverse effects Toegenomen frequentie neurologische schade. Ptn met ankylosing spondylitis. 5% ptn met wervelfractuur had as 4.5 mmHG ICP stijging door compressie vv jugularis Gecompromiseerde mondopening Aspiratie Decubitus Discomfort, pijn, stress Toename beeldvorming Bij penetrerend letsel; verhoogde mortaliteit en morbiditeit

31
Neurologische schade

32
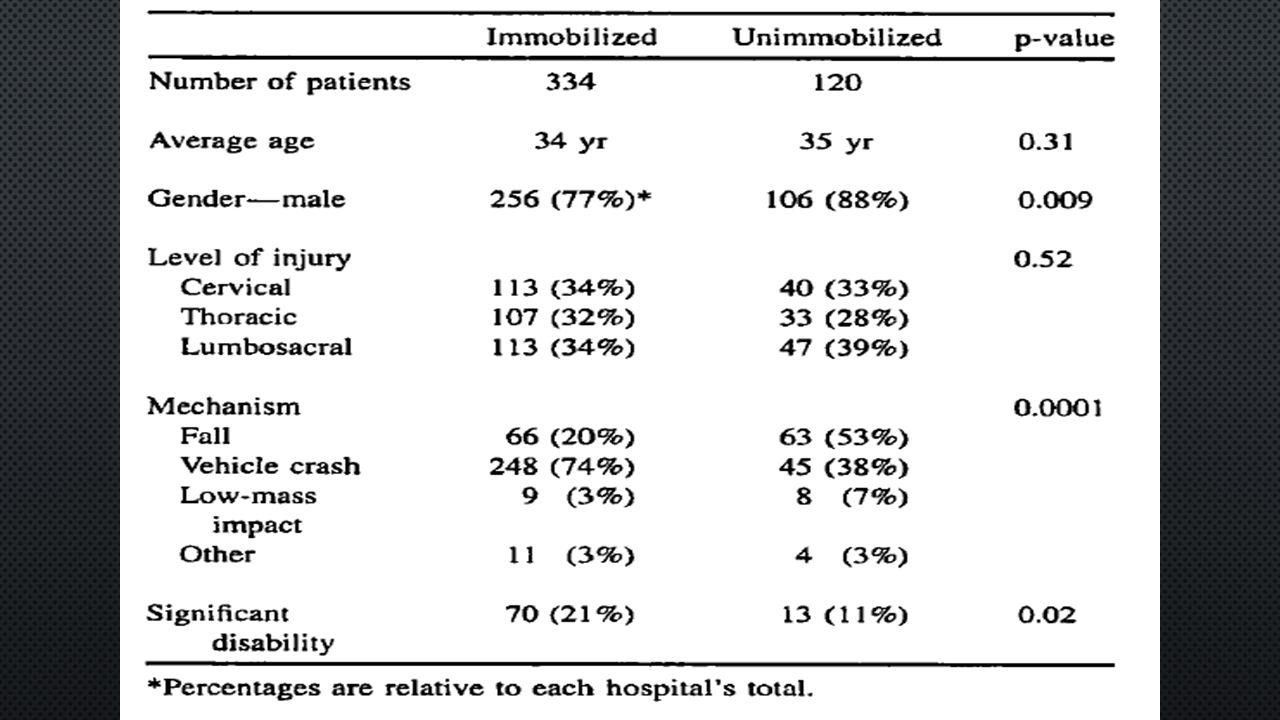
Hauswald et al. Out of hospital spinal immobilization: its effect on neurologic injury. Acad Emerg Med 1998:5( ) METHODS: A 5-year retrospective chart review at 2 university hospitals. None of the 120 patients seen at the University of Malaya had spinal immobilization during transport all 334 patients seen at the University of New Mexico did. Neurologic injuries were assigned to 2 categories, disabling or not disabling, RESULTS: There was less neurologic disability in the unimmobilized Malaysian patients (OR 2.03; 95% CI ; p = 0.04). Results were similar when the analysis was limited to patients with cervical injuries (OR 1.52; 95% CI ; p = 0.34). CONCLUSION: Out-of-hospital immobilization has little or no effect on neurologic outcome in patients with blunt spinal injuries.
. Results were similar when the analysis was limited to patients with cervical injuries (OR 1.52; 95% CI ; p = 0.34). CONCLUSION: Out-of-hospital immobilization has little or no effect on neurologic outcome in patients with blunt spinal injuries.")
34
Maar… EXCLUSIE OVERLEDEN PTN (ONGEVAL OF TIJDENS TRANSPORT)
GEEN TRAUMA SEVERITY SCORES HETEROGENITEIT SPINAL INJURY NIVEAU ZORG? ALLEEN INCLUSIE BIJ BEWEZEN LETSEL

35
ICP

36
Graig et al. 1991 Intensive care med Davies et al
Graig et al Intensive care med Davies et al Injury Hunt et al Anesthesia kolb et al Am J Emerg Mobbs et al anz j Surg Stone et al Acad Emerg Med GRAIG: 2X CASE REPORT IC, BIJ KRAAG ICP STIJGING DAVIES: N=19, IC, GEMIDDELDE STIJGING 4.5 MMHG, LANGDURIG KRAAG HUNT: N=30, IC, GEMIDDELDE STIJGING 4.6 MMHG, >15 MMHG STERKER KOLB: N=20, CEREBROSPINAL FLUID PRESSURE (CSFP) 24.8MM H2O STIJGING MOBBS: N=10, GEMIDDELDE STIJGING 4.4 MMHG, KRAAG BIJ TRAUMA STONE: N=42 VRIJWILLIGERS, DOORSNEDE VV JUG MET ECHO, SIGN TOENAME
 24.8MM H2O STIJGING. MOBBS: N=10, GEMIDDELDE STIJGING 4.4 MMHG, KRAAG BIJ TRAUMA. STONE: N=42 VRIJWILLIGERS, DOORSNEDE VV JUG MET ECHO, SIGN TOENAME.")
37
Pressure ulcurs

38
Powers et al. The incidence of skin breakdown associated with use of cervical collars. J Trauma nurs 2006:13( ) 484 patients Patients had the cervical collar in place for an average of 10.3 days, with an SD of 11.4 days. Skin breakdown was noted in 33 (6.8%) patients
 patients.")
39
Walker et al. Pressure ulcurs in cervical spine immobilisation: a retrospective analysis. J wound care 2012;21( ) N=90, retrospectief Gaat om langdurig geïmmobiliseerde ptn (permanente kraag, halo)
")
40
Pijn, stress, onrust

41
March et al. Changes in physical examination caused by use of spinal immobilization. Prehosp emerg med 2002;6( ) METHODS: This was a single-blinded, prospective study at a tertiary care university teaching hospital. Twenty healthy volunteers without previous back pain or injuries, were fully immobilized for one hour, with a cervical collar and strapped to a long wooden backboard. Midline palpation of vertebrae to illicit pain was performed at 10-minute intervals. participants were asked to rate neck and back pain on a scale from 1 to 10 (1 for no pain, and 10 for unbearable pain), to see whether subjective pain from immobilization correlated with tenderness to palpation. RESULTS: Three patients had point tenderness of cervical vertebrae within 40 minutes. Five patients developed point tenderness of vertebrae by 60 minutes. Eighteen of 20 participants complained of increasing discomfort over time. The median initial pain scale was 1 (range 1-1), in contrast to 4 (range 1-9) at 60 minutes, p < CONCLUSION: standard immobilization causes a false-positive exam for midline vertebral tenderness.
, to see whether subjective pain from immobilization correlated with tenderness to palpation. RESULTS: Three patients had point tenderness of cervical vertebrae within 40 minutes. Five patients developed point tenderness of vertebrae by 60 minutes. Eighteen of 20 participants complained of increasing discomfort over time. The median initial pain scale was 1 (range 1-1), in contrast to 4 (range 1-9) at 60 minutes, p < CONCLUSION: standard immobilization causes a false-positive exam for midline vertebral tenderness.")
42
Toename beeldvorming

43
Leonard et al. Potential adverse effects of spinal immobilization in children. Prehosp emerg care 2012;16(4): METHODS: a prospective cohort study of children presenting to the emergency department (ED) for evaluation following trauma over a 13-month period. spinal immobilization prior to physician evaluation or if they met the American College of Surgeons (ACS) guidelines for spinal immobilization but were not immobilized. self-reported pain, use of radiography to evaluate the cervical spine, ED length of stay, and ED disposition. RESULTS: 137 spine-immobilized children and 112 not immobilized There were differences between the two study groups, which included age, mechanism of injury comparable Pediatric Trauma Scores (PTSs) and Glasgow Coma Scale scores (GCSs). Immobilized children had a higher median pain score (3 versus 2) cervical radiography (56.6% versus 13.4%) admitted to the hospital (41.6% versus 14.3%) The comparison groups had similar lengths of stay in the ED.
 for evaluation following trauma over a 13-month period. spinal immobilization prior to physician evaluation or if they met the American College of Surgeons (ACS) guidelines for spinal immobilization but were not immobilized. self-reported pain, use of radiography to evaluate the cervical spine, ED length of stay, and ED disposition. RESULTS: 137 spine-immobilized children and 112 not immobilized. There were differences between the two study groups, which included age, mechanism of injury. comparable Pediatric Trauma Scores (PTSs) and Glasgow Coma Scale scores (GCSs). Immobilized children had a higher median pain score (3 versus 2) cervical radiography (56.6% versus 13.4%) admitted to the hospital (41.6% versus 14.3%) The comparison groups had similar lengths of stay in the ED.")
44
Conclusie Evidence = zwak, met name gebaseerd op de historische beïnvloeding Steeds meer onderzoek wijst op negatieve effecten Stop routinematig aanbrengen kraag Wervelplank, blocks en straps Extractie met behulp kraag Pogen tot vervoer minder rigide vacuummatras

45
Spinal immobilisatie naar spinal voorzorgsmaatregelen
Prehospital Emergency Care Apr/June: 18(2); EMS spinal precautions and the use of the long backboard resource document to the position statement of the national association of EMS physicians and the american college of surgeons committee on trauma Chelsea C White et al. Overeenkomstig Cultuuromslag Spinal immobilisatie naar spinal voorzorgsmaatregelen
; EMS spinal precautions and the use of the long backboard resource document to the position statement of the national association of EMS physicians and the american college of surgeons committee on trauma Chelsea C White et al. Overeenkomstig. Cultuuromslag. Spinal immobilisatie naar spinal voorzorgsmaatregelen.")
46
Adverse effects TOEGENOMEN FREQUENTIE NEUROLOGISCHE SCHADE.
PTN MET ANKYLOSING SPONDYLITIS. 5% PTN MET WERVELFRACTUUR HAD AS 4.5 MMHG ICP STIJGING DOOR COMPRESSIE VV JUGULARIS > KLINISCH RELEVANT?, IC SETTTING GECOMPROMISEERDE MONDOPENING ASPIRATIE DECUBITUS > KLINISCHE RELEVANT?, PROBLEEM BEHANDELING DISCOMFORT, PIJN, STRESS > FOUTPOSITIEF ONDERZOEK TOENAME BEELDVORMING > BIJ KINDEREN, JA BIJ PENETREREND LETSEL; VERHOOGDE MORTALITEIT EN MORBIDITEIT

47
Terug naar LPA8…Eigen mening
Evidence voor zwak Evidence tegen zwak Niet alle ‘hoogtepunten’ terug te vinden in literatuur Streven na kortdurende immobilisatie Vacuummatras verdedigbaar Toename discutabele situaties aangeboden traumapatienten (denk aan de traumachirurg casus) Logistieke problemen te verwachten?
 Logistieke problemen te verwachten")
48
Discussie

Verwante presentaties




 Quiz Night !>")















