Download de presentatie
De presentatie wordt gedownload. Even geduld aub

1
COPD: wat is er nieuw? V. Nowé

2
Topics Begin: = oud (GOLD 2011) Wat is er naast GOLD?
GOLD C – D: iedereen IHC? Effect op exacerbaties? Pneumonie? Dosis IHC? Afbouwen mogelijk en bij wie? Azithromycine: wie? Nieuwe inhalatoren Pneumococcenvaccin Acetylcysteïne

3
GOLD COPD aanpak/behandeling: Doel:
a five-year mortality rate of about 50% COPD aanpak/behandeling: Doel: Symptomen verminderen (Korte termijn) Verminderen van exacerbaties/hospitalisaties (Lange termijn) Exacerbaties/hospitalisatie GOLD 1. objectives that are directed towards immediately relieving and reducing the impact of symptoms, and objectives that reduce the risk of adverse health events that may affect the patient at some point in the future. + ECLIPSE 2. Pharmacologic therapy for COPD is used to reduce symptoms, reduce the frequency and severity of exacerbations, and improve health status and exercise tolerance. 3. A second strength of the original strategy was the simple, intuitive system for classifying COPD severity. This was based upon the FEV1 and was called a staging system because it was believed, at the time, that the majority of patients followed a path of disease progression in which the severity of the disease tracked the severity of the airflow limitation. Much is now known about the characteristics of patients in the different GOLD stages – for example, their level of risk of exacerbations, hospitalization, and death. However at an individual patient level, the FEV1 is an unreliable marker of the severity of breathlessness, exercise limitation, and health status impairment. 4. Long-term prognosis following hospitalization for COPD exacerbation is poor, with a five-year mortality rate of about 50% 604. Factors independently associated with poor outcome include older age, lower body mass index, comorbidities (e.g., cardiovascular disease or lung cancer), previous admissions for COPD exacerbations, clinical severity of the index exacerbation and need for long-term oxygen therapy at discharge605,606. Patients characterized by a higher prevalence and severity of respiratory symptoms, poorer quality of life, worse lung function, lower exercise capacity, lower lung density and thickened bronchial walls on CT-scan are also at increased risk of shorter long-term survival following an acute COPD exacerbation607. 4. An exacerbation of COPD is defined as an acute event characterized by a worsening of the patient’s respiratory symptoms that is beyond normal day-to-day variations and leads to a change in medication The rate at which exacerbations occur varies greatly between patients131,512. The best predictor of having frequent exacerbations (2 or more exacerbations per year) is a history of previous treated events132. In addition, worsening airflow limitation is associated with an increasing prevalence of exacerbations and risk of death. Hospitalization for a COPD exacerbation is associated with a poor prognosis with increased risk of death556 Sneller achteruitgang Lf Gedaalde fysische activiteit/inspanningstolerantie Gedaalde QOL Verhoogd risico op overlijden
 Verminderen van exacerbaties/hospitalisaties (Lange termijn) Exacerbaties/hospitalisatie. GOLD. 1. objectives that are directed towards immediately relieving and reducing the impact of symptoms, and objectives that reduce the risk of adverse health events that may affect the patient at some point in the future. + ECLIPSE. 2. Pharmacologic therapy for COPD is used to reduce symptoms, reduce the frequency and severity of exacerbations, and improve health status and exercise tolerance. 3. A second strength of the original strategy was the simple, intuitive system for classifying COPD severity. This was based upon the FEV1 and was called a staging system because it was believed, at the time, that the majority of patients followed a path of disease progression in which the severity of the disease tracked the severity of the airflow limitation. Much is now known about the characteristics of patients in the different GOLD stages – for example, their level of risk of exacerbations, hospitalization, and death. However at an individual patient level, the FEV1 is an unreliable marker of the severity of breathlessness, exercise limitation, and health status impairment. 4. Long-term prognosis following hospitalization for COPD exacerbation is poor, with a five-year mortality rate of about 50% 604. Factors independently associated with poor outcome include older age, lower body mass index, comorbidities (e.g., cardiovascular disease or lung cancer), previous admissions for COPD exacerbations, clinical severity of the index exacerbation and need for long-term oxygen therapy at discharge605,606. Patients characterized by a higher prevalence and severity of respiratory symptoms, poorer quality of life, worse lung function, lower exercise capacity, lower lung density and thickened bronchial walls on CT-scan are also at increased risk of shorter long-term survival following an acute COPD exacerbation An exacerbation of COPD is defined as an acute event characterized by a worsening of the patient’s respiratory symptoms that is beyond normal day-to-day variations and leads to a change in medication The rate at which exacerbations occur varies greatly between patients131,512. The best predictor of having frequent exacerbations (2. or more exacerbations per year) is a history of previous treated events132. In addition, worsening airflow limitation is associated with an increasing prevalence of exacerbations and risk of death. Hospitalization for a COPD exacerbation is associated with a poor prognosis with increased risk of death556. Sneller achteruitgang Lf. Gedaalde fysische activiteit/inspanningstolerantie. Gedaalde QOL. Verhoogd risico op overlijden.")
4
GOLD 2001 -2015 Aanpassing 2001: COPD obv ernst (FEV1): stadia I-IV 2.
A second strength of the original strategy was the simple, intuitive system for classifying COPD severity. This was based upon the FEV1 and was called a staging system because it was believed, at the time, that the majority of patients followed a path of disease progression in which the severity of the disease tracked the severity of the airflow limitation. Much is now known about the characteristics of patients in the different GOLD stages – for example, their level of risk of exacerbations, hospitalization, and death. However at an individual patient level, the FEV1 is an unreliable marker of the severity of breathlessness, exercise limitation, and health status impairment. 3. Long-term prognosis following hospitalization for COPD exacerbation is poor, with a five-year mortality rate of about 50%604. Factors independently associated with poor outcome include older age, lower body mass index, comorbidities (e.g., cardiovascular disease or lung cancer), previous admissions for COPD exacerbations, clinical severity of the index exacerbation and need for long-term oxygen therapy at discharge605,606. Patients characterized by a higher prevalence and severity of respiratory symptoms, poorer quality of life, worse lung function, lower exercise capacity, lower lung density and thickened bronchial walls on CT-scan are also at increased risk of shorter long-term survival following an acute COPD exacerbation607. 4. An exacerbation of COPD is defined as an acute event characterized by a worsening of the patient’s respiratory symptoms that is beyond normal day-to-day variations and leads to a change in medication The rate at which exacerbations occur varies greatly between patients131,512. The best predictor of having frequent exacerbations (2 or more exacerbations per year) is a history of previous treated events132. In addition, worsening airflow limitation is associated with an increasing prevalence of exacerbations and risk of death. Hospitalization for a COPD exacerbation is associated with a poor prognosis with increased risk of death556 5. GOLD concomitant COPD increases morbidity and mortality among patients with IHD610 --> COPD: meer mort bij Isch heart disease
, previous admissions for COPD exacerbations, clinical severity of the index exacerbation and need for long-term oxygen therapy at discharge605,606. Patients characterized by a higher prevalence and severity of respiratory symptoms, poorer quality of life, worse lung function, lower exercise capacity, lower lung density and thickened bronchial walls on CT-scan are also at increased risk of shorter long-term survival following an acute COPD exacerbation An exacerbation of COPD is defined as an acute event characterized by a worsening of the patient’s respiratory symptoms that is beyond normal day-to-day variations and leads to a change in medication The rate at which exacerbations occur varies greatly between patients131,512. The best predictor of having frequent exacerbations (2. or more exacerbations per year) is a history of previous treated events132. In addition, worsening airflow limitation is associated with an increasing prevalence of exacerbations and risk of death. Hospitalization for a COPD exacerbation is associated with a poor prognosis with increased risk of death GOLD. concomitant COPD increases morbidity and mortality among patients with IHD610 --> COPD: meer mort bij Isch heart disease.")
5
2. A second strength of the original strategy was the simple, intuitive system for classifying COPD severity. This was based upon the FEV1 and was called a staging system because it was believed, at the time, that the majority of patients followed a path of disease progression in which the severity of the disease tracked the severity of the airflow limitation. Much is now known about the characteristics of patients in the different GOLD stages – for example, their level of risk of exacerbations, hospitalization, and death. However at an individual patient level, the FEV1 is an unreliable marker of the severity of breathlessness, exercise limitation, and health status impairment. --> HETEROGENE groep!!! 3. Long-term prognosis following hospitalization for COPD exacerbation is poor, with a five-year mortality rate of about 50%604. Factors independently associated with poor outcome include older age, lower body mass index, comorbidities (e.g., cardiovascular disease or lung cancer), previous admissions for COPD exacerbations, clinical severity of the index exacerbation and need for long-term oxygen therapy at discharge605,606. Patients characterized by a higher prevalence and severity of respiratory symptoms, poorer quality of life, worse lung function, lower exercise capacity, lower lung density and thickened bronchial walls on CT-scan are also at increased risk of shorter long-term survival following an acute COPD exacerbation607. 4. An exacerbation of COPD is defined as an acute event characterized by a worsening of the patient’s respiratory symptoms that is beyond normal day-to-day variations and leads to a change in medication The rate at which exacerbations occur varies greatly between patients131,512. The best predictor of having frequent exacerbations (2 or more exacerbations per year) is a history of previous treated events132. In addition, worsening airflow limitation is associated with an increasing prevalence of exacerbations and risk of death. Hospitalization for a COPD exacerbation is associated with a poor prognosis with increased risk of death556 5. GOLD concomitant COPD increases morbidity and mortality among patients with IHD610 --> COPD: meer mort bij Isch heart disease
, previous admissions for COPD exacerbations, clinical severity of the index exacerbation and need for long-term oxygen therapy at discharge605,606. Patients characterized by a higher prevalence and severity of respiratory symptoms, poorer quality of life, worse lung function, lower exercise capacity, lower lung density and thickened bronchial walls on CT-scan are also at increased risk of shorter long-term survival following an acute COPD exacerbation An exacerbation of COPD is defined as an acute event characterized by a worsening of the patient’s respiratory symptoms that is beyond normal day-to-day variations and leads to a change in medication The rate at which exacerbations occur varies greatly between patients131,512. The best predictor of having frequent exacerbations (2. or more exacerbations per year) is a history of previous treated events132. In addition, worsening airflow limitation is associated with an increasing prevalence of exacerbations and risk of death. Hospitalization for a COPD exacerbation is associated with a poor prognosis with increased risk of death GOLD. concomitant COPD increases morbidity and mortality among patients with IHD610 --> COPD: meer mort bij Isch heart disease.")
6
GOLD 2001 - 2015 Aanpassing 2001: COPD obv ernst (FEV1): stadia I-IV
2011: FEV1 niet betrouwbare marker voor ernst van symptomen (dyspnoe, inspanningsbeperking, exacerbatierisico, hospitalisatierisico, overlijden) --> GOLD klassen A-B-C-D 2013,2014 en 2015 updates 2. A second strength of the original strategy was the simple, intuitive system for classifying COPD severity. This was based upon the FEV1 and was called a staging system because it was believed, at the time, that the majority of patients followed a path of disease progression in which the severity of the disease tracked the severity of the airflow limitation. Much is now known about the characteristics of patients in the different GOLD stages – for example, their level of risk of exacerbations, hospitalization, and death. However at an individual patient level, the FEV1 is an unreliable marker of the severity of breathlessness, exercise limitation, and health status impairment. 3. Long-term prognosis following hospitalization for COPD exacerbation is poor, with a five-year mortality rate of about 50%604. Factors independently associated with poor outcome include older age, lower body mass index, comorbidities (e.g., cardiovascular disease or lung cancer), previous admissions for COPD exacerbations, clinical severity of the index exacerbation and need for long-term oxygen therapy at discharge605,606. Patients characterized by a higher prevalence and severity of respiratory symptoms, poorer quality of life, worse lung function, lower exercise capacity, lower lung density and thickened bronchial walls on CT-scan are also at increased risk of shorter long-term survival following an acute COPD exacerbation607. 4. An exacerbation of COPD is defined as an acute event characterized by a worsening of the patient’s respiratory symptoms that is beyond normal day-to-day variations and leads to a change in medication The rate at which exacerbations occur varies greatly between patients131,512. The best predictor of having frequent exacerbations (2 or more exacerbations per year) is a history of previous treated events132. In addition, worsening airflow limitation is associated with an increasing prevalence of exacerbations and risk of death. Hospitalization for a COPD exacerbation is associated with a poor prognosis with increased risk of death556 5. GOLD concomitant COPD increases morbidity and mortality among patients with IHD610 --> COPD: meer mort bij Isch heart disease
 --> GOLD klassen A-B-C-D. 2013,2014 en 2015 updates. 2. A second strength of the original strategy was the simple, intuitive system for classifying COPD severity. This was based upon the FEV1 and was called a staging system because it was believed, at the time, that the majority of patients followed a path of disease progression in which the severity of the disease tracked the severity of the airflow limitation. Much is now known about the characteristics of patients in the different GOLD stages – for example, their level of risk of exacerbations, hospitalization, and death. However at an individual patient level, the FEV1 is an unreliable marker of the severity of breathlessness, exercise limitation, and health status impairment. 3. Long-term prognosis following hospitalization for COPD exacerbation is poor, with a five-year mortality rate of about 50%604. Factors independently associated with poor outcome include older age, lower body mass index, comorbidities (e.g., cardiovascular disease or lung cancer), previous admissions for COPD exacerbations, clinical severity of the index exacerbation and need for long-term oxygen therapy at discharge605,606. Patients characterized by a higher prevalence and severity of respiratory symptoms, poorer quality of life, worse lung function, lower exercise capacity, lower lung density and thickened bronchial walls on CT-scan are also at increased risk of shorter long-term survival following an acute COPD exacerbation An exacerbation of COPD is defined as an acute event characterized by a worsening of the patient’s respiratory symptoms that is beyond normal day-to-day variations and leads to a change in medication The rate at which exacerbations occur varies greatly between patients131,512. The best predictor of having frequent exacerbations (2. or more exacerbations per year) is a history of previous treated events132. In addition, worsening airflow limitation is associated with an increasing prevalence of exacerbations and risk of death. Hospitalization for a COPD exacerbation is associated with a poor prognosis with increased risk of death GOLD. concomitant COPD increases morbidity and mortality among patients with IHD610 --> COPD: meer mort bij Isch heart disease.")
7
GOLD 2015: klassen GOLD 2015: therapie Symptomen
Risico’s op exacerbaties Ernst longfunctie afwijkingen GOLD 2015: therapie Klasse Comorbiditeit GOLD 1. Assessment of COPD is based on the patient’s level of symptoms, future risk of exacerbations, the severity of the spirometric abnormality, and the identification of comorbidities. 2. Prevalentie most national data show that less than 6% of the adult population has been told that they have COPD8. This likely reflects the widespread under-recognition and under- diagnosis of COPD9. 5 latijns amerikaanse steden: In each country, the prevalence of COPD increased steeply with age, with the highest prevalence among those over age 60, ranging in the total population from a low of 7.8% in Mexico City, Mexico to a high of 19.7% in Montevideo, Uruguay. 3. Astma In the European Community Respiratory Health Survey, bronchial hyperresponsiveness was second only to cigarette smoking as the leading risk factor for COPD, responsible for 15% of the population attributable risk (smoking had a population attributable risk of 39%)73. 4. Comorbiditeit Comorbidities that occur frequently in COPD patients include cardiovascular disease, skeletal muscle dysfunction, metabolic syndrome, osteoporosis, depression and lung cancer. The existence of COPD may actually increase the risk for other diseases; this is particularly striking for COPD and lung cancer Whether this association is due to common risk factors (e.g., smoking), involvement of susceptibility genes, or impaired clearance of carcinogens is not clear. Comorbidities can occur in patients with mild, moderate or severe airflow limitation131, influence mortality and hospitalizations independently142, and deserve specific treatment. Therefore, comorbidities should be looked for routinely, and treated appropriately, in any patient with COPD.
 Comorbiditeit. Comorbidities that occur frequently in COPD patients include cardiovascular disease, skeletal muscle dysfunction, metabolic syndrome, osteoporosis, depression and lung cancer. The existence of COPD may actually increase the risk for other diseases; this is particularly striking for COPD and lung cancer Whether this association is due to common risk factors (e.g., smoking), involvement of susceptibility genes, or impaired clearance of carcinogens is not clear. Comorbidities can occur in patients with mild, moderate or severe airflow limitation131, influence mortality and hospitalizations independently142, and deserve specific treatment. Therefore, comorbidities should be looked for routinely, and treated appropriately, in any patient with COPD.")
8
ECLIPSE: Verhoogd risico op exacerbaties: heterogeniteit
GOLD 1. Studies --> These show an increase in risk of exacerbations, hospitalization and death with worsening of airflow limitation. 131 Agusti A, Calverley PM, Celli B, et al. Characterisation of COPD heterogeneity in the ECLIPSE cohort. Respir Res 2010;11:122. 2. --> prospectively collected data from large medium-term clinical trials They are not precise estimates that apply to each patient, but they illustrate clearly the increased risk of exacerbations and death between spirometric levels. Roughly, although up to 20% of GOLD 2 (Moderate aiflow limitation) patients may experience frequent exacerbations requiring treatment with antibiotics and/or systemic corticosteroids132 ECLIPSE, the risk of exacerbations significantly increases in GOLD 3 (Severe) and GOLD 4 (Very Severe). Since exacerbations increase the decline in lung function, deterioration in health status and risk of death, the assessment of exacerbation risk can also be seen as an assessment of the risk of poor outcomes in general. ECLIPSE: Verhoogd risico op exacerbaties: heterogeniteit
 patients may experience frequent exacerbations requiring treatment with antibiotics and/or systemic corticosteroids132 ECLIPSE, the risk of exacerbations significantly increases in GOLD 3 (Severe) and GOLD 4 (Very Severe). Since exacerbations increase the decline in lung function, deterioration in health status and risk of death, the assessment of exacerbation risk can also be seen as an assessment of the risk of poor outcomes in general. ECLIPSE: Verhoogd risico op exacerbaties: heterogeniteit.")
9
ECLIPSE = ECLIPSE Studie = 3 jaar 2138 pt
The best predictor of having frequent exacerbations (2 or more exacerbations per year) is a history of previous treated events132. In addition, worsening airflow limitation is associated with an increasing prevalence of exacerbations and risk of death. Hospitalization for a COPD exacerbation is associated with a poor prognosis with increased risk of death556. ECLIPSE
 is a history of previous treated events132. In addition, worsening airflow limitation is associated with an increasing prevalence of exacerbations and risk of death. Hospitalization for a COPD exacerbation is associated with a poor prognosis with increased risk of death556. ECLIPSE.")
10
In eerste jaar vd studie
Sterk geassocieerd met exa in voorafgaande jaar 29% Geen exa in 3 jaar Geen exa in voorgaande jaar Er is dus een stabiel fenotype dat frequent exacerbeert Dwz een groep van patienten die ongeacht de ernst van Lfverlies, meer gevoelig is voor het krijgen van exacerbaties Deze groep kan geidentificeerd w door navragen exacerbaties in voorafgaande jaar, en dit fenotype blijft stabiel over een 3jaar periode. De belangrijkste parameter voor frequente exacerbaties (>=2 per jaar) in alle GOLD stadia : een voorgeschiedenis van exacerbaties De incidentie v frequente exacerbaties stijgt wel met ernsiger stadium van Lf verlies
 in alle GOLD stadia : een voorgeschiedenis van exacerbaties. De incidentie v frequente exacerbaties stijgt wel met ernsiger stadium van Lf verlies.")
11
GOLD C D A B ICS + LABA or LAMA ICS + LABA and/or LAMA SAMA prn or
Global Strategy for Diagnosis, Management and Prevention of COPD Manage Stable COPD: Pharmacologic Therapy RECOMMENDED FIRST CHOICE GOLD C D 2 or more or > 1 leading to hospital admission 1 (not leading to hospital admission) GOLD 4 ICS + LABA or LAMA ICS + LABA and/or LAMA GOLD 3 Exacerbations per year A B GOLD 2 CAT, CCQ, MMRC SAMA prn or SABA prn LABA or LAMA GOLD 1 CAT < 10 mMRC 0-1 CAT > 10 mMRC > 2 © 2014 Global Initiative for Chronic Obstructive Lung Disease
 GOLD 4. ICS + LABA. or. LAMA. ICS + LABA. and/or. LAMA. GOLD 3. Exacerbations per year. A. B. GOLD 2. CAT, CCQ, MMRC. SAMA prn. or. SABA prn. LABA. or. LAMA. GOLD 1. CAT < 10. mMRC 0-1. CAT > 10. mMRC > 2. © 2014 Global Initiative for Chronic Obstructive Lung Disease.")
12
GOLD Symptomen

13
© 2014 Global Initiative for Chronic Obstructive Lung Disease
Global Strategy for Diagnosis, Management and Prevention of COPD Modified MRC (mMRC)Questionnaire GOLD simple measure of breathlessness such as the Modified British Medical Research Council (mMRC) Questionnaire (Table 2.4) was considered adequate for assessment of symptoms, as the mMRC relates well to other measures of health status91 and predicts future mortality risk92. However, it is now recognized that COPD has multiple symptomatic effects151. For this reason, a comprehensive symptom assessment is recommended rather than just a measure of breathlessness © 2014 Global Initiative for Chronic Obstructive Lung Disease
Questionnaire. GOLD. simple measure of breathlessness such as the Modified British Medical Research Council (mMRC) Questionnaire (Table 2.4) was considered adequate for assessment of symptoms, as the mMRC relates well to other measures of health status91 and predicts future mortality risk92. However, it is now recognized that COPD has multiple symptomatic effects151. For this reason, a comprehensive symptom assessment is recommended rather than just a measure of breathlessness. © 2014 Global Initiative for Chronic Obstructive Lung Disease.")
14
© 2014 Global Initiative for Chronic Obstructive Lung Disease
GOLD Global Strategy for Diagnosis, Management and Prevention of COPD Assess Risk of Exacerbations To assess risk of exacerbations use history of exacerbations and spirometry: Two or more exacerbations within the last year or an FEV1 < 50 % of predicted value are indicators of high risk. One or more hospitalizations for COPD exacerbation should be considered high risk. mssch © 2014 Global Initiative for Chronic Obstructive Lung Disease

15
GOLD Global Strategy for Diagnosis, Management and Prevention of COPD Therapeutic Options: Key Points Appropriate pharmacologic therapy can reduce COPD symptoms, reduce the frequency and severity of exacerbations, and improve health status and exercise tolerance. None of the existing medications for COPD has been shown conclusively to modify the long-term decline in lung function. Influenza and pneumococcal vaccination should be offered depending on local guidelines. Smoking cessation WEL

16
© 2014 Global Initiative for Chronic Obstructive Lung Disease
GOLD Global Strategy for Diagnosis, Management and Prevention of COPD Therapeutic Options: Bronchodilators Bronchodilator medications are central to the symptomatic management of COPD. Bronchodilators are prescribed on an as-needed or on a regular basis to prevent or reduce symptoms. The principal bronchodilator treatments are beta2- agonists, anticholinergics, theophylline or combination therapy. The choice of treatment depends on the availability of medications and each patient’s individual response in terms of symptom relief and side effects.. WEL © 2014 Global Initiative for Chronic Obstructive Lung Disease

17
Global Strategy for Diagnosis, Management and Prevention of COPD Therapeutic Options: Inhaled Corticosteroids GOLD Regular treatment with inhaled corticosteroids improves symptoms, lung function and quality of life and reduces frequency of exacerbations for COPD patients with an FEV1 < 60% predicted. Inhaled corticosteroid therapy is associated with an increased risk of pneumonia. Withdrawal from treatment with inhaled corticosteroids may lead to exacerbations in some patients. WEL

18
Depending on local guidelines
Global Strategy for Diagnosis, Management and Prevention of COPD Manage Stable COPD: Non-pharmacologic Patient Group Essential Recommended Depending on local guidelines A Smoking cessation (can include pharmacologic treatment) Physical activity Flu vaccination Pneumococcal vaccination B, C, D Pulmonary rehabilitation © 2014 Global Initiative for Chronic Obstructive Lung Disease
 Physical activity. Flu vaccination. Pneumococcal vaccination. B, C, D. Pulmonary rehabilitation. © 2014 Global Initiative for Chronic Obstructive Lung Disease.")
19
RecommendedFirst choice
Global Strategy for Diagnosis, Management and Prevention of COPD Manage Stable COPD: Pharmacologic Therapy (Medications in each box are mentioned in alphabetical order, and therefore not necessarily in order of preference.) Patient RecommendedFirst choice Alternative choice Other Possible Treatments A SAMA prn or SABA prn LAMA LABA SABA and SAMA Theophylline B LAMA and LABA SABA and/or SAMA C ICS + LABA LAMA and LABA or LAMA and PDE4-inh. or LABA and PDE4-inh. D and/or ICS + LABA and LAMA or ICS+LABA and PDE4-inh. or LAMA and PDE4-inh. Carbocysteine
 Patient. RecommendedFirst choice. Alternative choice. Other Possible. Treatments. A. SAMA prn. or. SABA prn. LAMA. LABA. SABA and SAMA. Theophylline. B. LAMA and LABA. SABA and/or SAMA. C. ICS + LABA. LAMA and LABA or. LAMA and PDE4-inh. or. LABA and PDE4-inh. D. and/or. ICS + LABA and LAMA or. ICS+LABA and PDE4-inh. or. LAMA and PDE4-inh. Carbocysteine.")
20
© 2014 Global Initiative for Chronic Obstructive Lung Disease
Global Strategy for Diagnosis, Management and Prevention of COPD Manage Exacerbations: Treatment Options Oxygen: titrate to improve the patient’s hypoxemia with a target saturation of 88-92%. Bronchodilators: Short-acting inhaled beta2-agonists with or without short-acting anticholinergics are preferred. Systemic Corticosteroids: Shorten recovery time, improve lung function (FEV1) and arterial hypoxemia (PaO2), and reduce the risk of early relapse, treatment failure, and length of hospital stay. A dose of 40 mg prednisone per day for 5 days is recommended. Nebulized magnesium as an adjuvent to salbutamol treatment in the setting of acute exacerbations of COPD has no effect on FEV1. NIET © 2014 Global Initiative for Chronic Obstructive Lung Disease
 and arterial hypoxemia (PaO2), and reduce the risk of early relapse, treatment failure, and length of hospital stay. A dose of 40 mg prednisone per day for 5 days is recommended. Nebulized magnesium as an adjuvent to salbutamol treatment in the setting of acute exacerbations of COPD has no effect on FEV1. NIET. © 2014 Global Initiative for Chronic Obstructive Lung Disease.")
21
Wat weten we naast GOLD?

22
Management of COPD according to Symptoms, Spirometric classification and Future Risk of Exacerbations ICS + LABA or LAMA ICS + LABA + LAMA 4 ≥ 2 3 (GOLD Classification of Airflow Limitation) Spirometry (Exacerbation history) Risk 2 1 SAMA or SAAB SOS LAMA or LABA Iedereen staat op IHC+LABA+LAMA vanaf GOLD 3-4 en >1 exacerbatie per jaar! Maar GOLD zegt ook bronchodill is hoeksteen van de behandeling --> zeker die pt op LAMA+LAMA zetten. En wat doen we met de IHC? 1 mMRC < 2 CAT < 10 mMRC ≥ 2 CAT ≥ 10 Symptoms (mMRC or CAT score)
 Spirometry. (Exacerbation history) Risk SAMA or SAAB SOS. LAMA or LABA. Iedereen staat op IHC+LABA+LAMA vanaf GOLD 3-4 en >1 exacerbatie per jaar! Maar GOLD zegt ook bronchodill is hoeksteen van de behandeling --> zeker die pt op LAMA+LAMA zetten. En wat doen we met de IHC 1. mMRC < 2. CAT < 10. mMRC ≥ 2. CAT ≥ 10. Symptoms. (mMRC or CAT score)")
23
© 2014 Global Initiative for Chronic Obstructive Lung Disease
GOLD Global Strategy for Diagnosis, Management and Prevention of COPD Therapeutic Options: Bronchodilators Bronchodilator medications are central to the symptomatic management of COPD. Bronchodilators are prescribed on an as-needed or on a regular basis to prevent or reduce symptoms. The principal bronchodilator treatments are beta2- agonists, anticholinergics, theophylline or combination therapy. The choice of treatment depends on the availability of medications and each patient’s individual response in terms of symptom relief and side effects.. HIER WEL © 2014 Global Initiative for Chronic Obstructive Lung Disease

24
TORCH

25
Effect of ICS on exacerbations (moderate and severe)
GSK STRICTLY CONFIDENTIAL Effect of ICS on exacerbations (moderate and severe) Mean number of exacerbations/year 17% reduction 1,2 1,13 0,97* 1 0,93* 0,85*†‡ 0,8 0,6 0,4 Matige exacerbaties worden gedefinieerd als exacerbaties waarvoor systemische corticosteroïden en/of antibiotica vereist zijn; ernstige exacerbaties worden gedefinieerd als exacerbaties waarvoor hospitalisatie vereist is. Het percentage exacerbaties werd berekend als het totaal aantal matige en/of ernstige exacerbaties die een patiënt kreeg gedurende de behandelingsperiode. Het aantal exacerbaties werd geanalyseerd door middel van een veralgemeend lineair model, uitgaande van een Negatieve binominale verdeling, met tijd op behandeling als een compensatievariabele. Het model omvatte aanpassingen voor de effecten van rookstatus, leeftijd, geslacht, ESW bij aanvang, aantal exacerbaties gemeld tijdens de 12 maanden vóór screening en van regio.1 SALM/FP verminderde op significante wijze het aantal matige/ernstige exacerbaties in vergelijking met placebo (25% reductie, p < 0,001), SALM (12% reductie, p = 0,002) en FP (9% reductie, p = 0,024). SALM en FP hadden ook significant minder exacerbaties dan placebo (respectievelijk 15%, p < 0,001 en 18%, p < 0,001). SALM/FP verminderde het aantal matige/ernstige exacerbaties in veel sterkere mate dan elk van de bestanddeelmonotherapieën. Exacerbaties en hospitalisaties voorspellen het sterfterisico door COPD over 5 jaren.2 Referentie Calverley PMA, Anderson JA, Celli B. for the TORCH investigators. Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. NEJM 2007; 356(8): & Online Supplement Soler-Cataluna JJ, Martinez-Garcia MA, Roman Sanchez P, et al. Severe acute exacerbations and mortality in patients with chronic obstructive pulmonary disease. Thorax 2005;60:925–31. 0,2 Placebo SALM FP SALM/FP Calverley P. et al. NEJM 2007.
 Mean number of exacerbations/year. 17% reduction. 1,2. 1,13. 0,97* 1. 0,93* 0,85*†‡ 0,8. 0,6. 0,4. Matige exacerbaties worden gedefinieerd als exacerbaties waarvoor systemische corticosteroïden en/of antibiotica vereist zijn; ernstige exacerbaties worden gedefinieerd als exacerbaties waarvoor hospitalisatie vereist is. Het percentage exacerbaties werd berekend als het totaal aantal matige en/of ernstige exacerbaties die een patiënt kreeg gedurende de behandelingsperiode. Het aantal exacerbaties werd geanalyseerd door middel van een veralgemeend lineair model, uitgaande van een Negatieve binominale verdeling, met tijd op behandeling als een compensatievariabele. Het model omvatte aanpassingen voor de effecten van rookstatus, leeftijd, geslacht, ESW bij aanvang, aantal exacerbaties gemeld tijdens de 12 maanden vóór screening en van regio.1. SALM/FP verminderde op significante wijze het aantal matige/ernstige exacerbaties in vergelijking met placebo (25% reductie, p < 0,001), SALM (12% reductie, p = 0,002) en FP (9% reductie, p = 0,024). SALM en FP hadden ook significant minder exacerbaties dan placebo (respectievelijk 15%, p < 0,001 en 18%, p < 0,001). SALM/FP verminderde het aantal matige/ernstige exacerbaties in veel sterkere mate dan elk van de bestanddeelmonotherapieën. Exacerbaties en hospitalisaties voorspellen het sterfterisico door COPD over 5 jaren.2. Referentie. Calverley PMA, Anderson JA, Celli B. for the TORCH investigators. Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. NEJM 2007; 356(8): & Online Supplement. Soler-Cataluna JJ, Martinez-Garcia MA, Roman Sanchez P, et al. Severe acute exacerbations and mortality in patients with chronic obstructive pulmonary disease. Thorax 2005;60:925–31. 0,2. Placebo. SALM. FP. SALM/FP. Calverley P. et al. NEJM")
26
Exacerbations requiring hospital admission
GSK STRICTLY CONFIDENTIAL Exacerbations requiring hospital admission Mean number of severe exacerbations/year 0,25 0,2 0,19 0,17 0,16* 0,16† 0,15 0,1 TORCH: Effect van IHC+LABA op ernstige exacerbaties Exacerbaties die hospitalisatie vereisen werden als ernstig geklasseerd. Het aantal exacerbaties werd geanalyseerd door middel van een veralgemeend lineair model, uitgaande van een negatieve binominale verdeling, met tijd op behandeling als een compensatievariabele. Het model omvatte aanpassingen voor de effecten van rookstatus, leeftijd, geslacht, ESW bij aanvang, aantal exacerbaties gemeld tijdens de 12 maanden vóór screening en van regio. Hospitalisatie kwam over 3 jaren minstens eenmaal voorbij 26% van de patiënten. Het jaarlijks opnamecijfer was 17% lager bij patiënten die met SALM/FP werden behandeld, vergeleken met placebo (p = 0,028). Exacerbaties en hospitalisaties voorspellen het sterfterisico door COPD over 5 jaren.1 Minder COPD-gebonden hospitalisaties is een belangrijk doel aangezien dit de levenskwaliteit van de patiënt zal verbeteren en bijgevolg de economische last van COPD zal verminderen. Referentie Soler-Cataluna JJ, Martinez-Garcia MA, Roman Sanchez P, et al. Severe acute exacerbations and mortality in patients with chronic obstructive pulmonary disease. Thorax 2005;60:925–31. Jones PW, Calverley PMA, Celli B et al. The Towards a Revolution in COPD Health (TORCH) study: fluticasone propionate/salmeterol improves and sustains health status in COPD over 3 years. Chest 2006; 130(4 suppl): 177S-178S 0,05 Placebo SALM FP SALM/FP Calverley P. et al. NEJM 2007.
. Exacerbaties en hospitalisaties voorspellen het sterfterisico door COPD over 5 jaren.1. Minder COPD-gebonden hospitalisaties is een belangrijk doel aangezien dit de levenskwaliteit van de patiënt zal verbeteren en bijgevolg de economische last van COPD zal verminderen. Referentie. Soler-Cataluna JJ, Martinez-Garcia MA, Roman Sanchez P, et al. Severe acute exacerbations and mortality in patients with chronic obstructive pulmonary disease. Thorax 2005;60:925–31. Jones PW, Calverley PMA, Celli B et al. The Towards a Revolution in COPD Health (TORCH) study: fluticasone propionate/salmeterol improves and sustains health status in COPD over 3 years. Chest 2006; 130(4 suppl): 177S-178S. 0,05. Placebo. SALM. FP. SALM/FP. Calverley P. et al. NEJM")
27
In COPD, hoe verhoudt zich het risico van ICS tov het voordeel van ICS?
NNH << NNT NNH < NNT NNH = NNT NNH > NNT NNH >> NNT NNH: Number Needed to Harm NNT: Number Needed to Treat

28
In COPD, hoe verhoudt zich het risico van ICS tov het voordeel van ICS?
NNH << NNT NNH < NNT NNH = NNT NNH > NNT NNH >> NNT NNH: Number Needed to Harm NNT: Number Needed to Treat

29
______________

30
ICS in COPD: risk of pneumonias
= NNH Suissa S., Thorax 2012.

31
ICS in COPD: risk of pneumonia
Risico op pneumonie is blijkbaar ook dosis afhankelijk!!! Price D. et al, PCRJ 2013.

32
Wat is de optimale dosis ICS bij COPD?
Budesonide 2x 400 = 800 µg Fluticason dipropionaat 2x 100 = 200 µg Fluticason dipropionaat 2x 250 = 500 µg Fluticason dipropionaat 2x 500 = µg Fluticason furoaat 1x 50 = 50 µg Fluticason furoaat 1x 92 = 92 µg Fluticason furoaat 1x 184 = 184 µg

33
Opmerking: Patiënten in de studie hadden een gedocumenteerde voorgeschiedenis van COPD met een post-bronchodilatorische FEV1 van 70% of minder i.vgl.m. voorspelde waarde en een FEV1/FVC van 0.70 of minder; minstens 10 tabak pakjaren en een gedocumenteerde voorgeschiedenis van 1 of meerdere COPD exacerbaties in het afgelopen jaar waarbij systemische of orale coricosteroïde behandeling of antibiotica werd toegediend of waarbij de patiënt gehospitaliseerd werd. In de run-in fase kregen alle patiënten fluticasone proprionaat/salmeterol 250/50 mcg 2x/d.

34
Opmerking: Dit zijn de pooled gegevens van 2 replica-studies. Relvar Ellipta 92/22 gaf de grootste reductie risico in exacerbaties, nl. 27% t.o.v. vilanterol alleen. Anders uitgedrukt: NNT (number needed to treat) versus vilanterol voor Relvar Ellipta is 3,3. (Als men 3,3 patiënten behandelt met Relvar Ellipta 92/22 in plaats van met vilanterol alleen, voorkomt men 1 exacerbatie) Inclusiecriterium was o.a. minimum 1 exacerbatie in het afgelopen jaar. Ongeveer 60% van de geïncludeerde patiënten hadden 1 exacerbatie gehad in het afgelopen jaar. Ongeveer 40% van de geïncludeerde patiënten hadden 2 of meer exacerbaties gehad in het afgelopen jaar.
 versus vilanterol voor Relvar Ellipta is 3,3. (Als men 3,3 patiënten behandelt met Relvar Ellipta 92/22 in plaats van met vilanterol alleen, voorkomt men 1 exacerbatie) Inclusiecriterium was o.a. minimum 1 exacerbatie in het afgelopen jaar. Ongeveer 60% van de geïncludeerde patiënten hadden 1 exacerbatie gehad in het afgelopen jaar. Ongeveer 40% van de geïncludeerde patiënten hadden 2 of meer exacerbaties gehad in het afgelopen jaar.")
35
Wat is de optimale dosis ICS bij COPD?
Budesonide 2x 400 = 800 µg ? Fluticason dipropionaat 2x 100 = 200 µg Fluticason dipropionaat 2x 250 = 500 µg ? Fluticason dipropionaat 2x 500 = µg Fluticason furoaat 1x 50 = 50 µg Fluticason furoaat 1x 92 = 92 µg Fluticason furoaat 1x 184 = 184 µg

36
In patiënten met COPD * leidt stoppen van ICS tot:
Exacerbaties Frequente exacerbaties Mortaliteit Depressie Geen van bovenstaande antwoorden * behandeld met tripple therapie (LAMA + LABA + ICS)
")
37
In patiënten met COPD * leidt stoppen van ICS tot:
Exacerbaties Frequente exacerbaties Mortaliteit Depressie Geen van bovenstaande antwoorden * behandeld met triple therapie (LAMA + LABA + ICS)
")
38
WISDOM trial _____ -->

39
WISDOM trial: exacerbations
Stelselmatig verlagen van IHC, bij groep LABA, LAMA en IHC, telkens dalen per 6 weken Magnussen H. et al, NEJM 2014.

40
Volgens GOLD Withdrawal from treatment with inhaled corticosteroids may lead to exacerbations in some patient, although in another study with severe and very severe COPD patients, inhaled corticosteroids could be gradually withdrawn over a three-month period without increasing the medium term risk of exacerbations, although lung function deteriorated significantly.

41
The ‘frequent exacerbator phenotype’: ECLIPSE Frequency/Severity of Exacerbations by GOLD stage
Er is een fenotype van exacerbatie Exacerbation rates increased with GOLD stage, irrespective of severity of exacerbation. Hurst JR, et al. N Engl J Med. 2010;363: 41

42
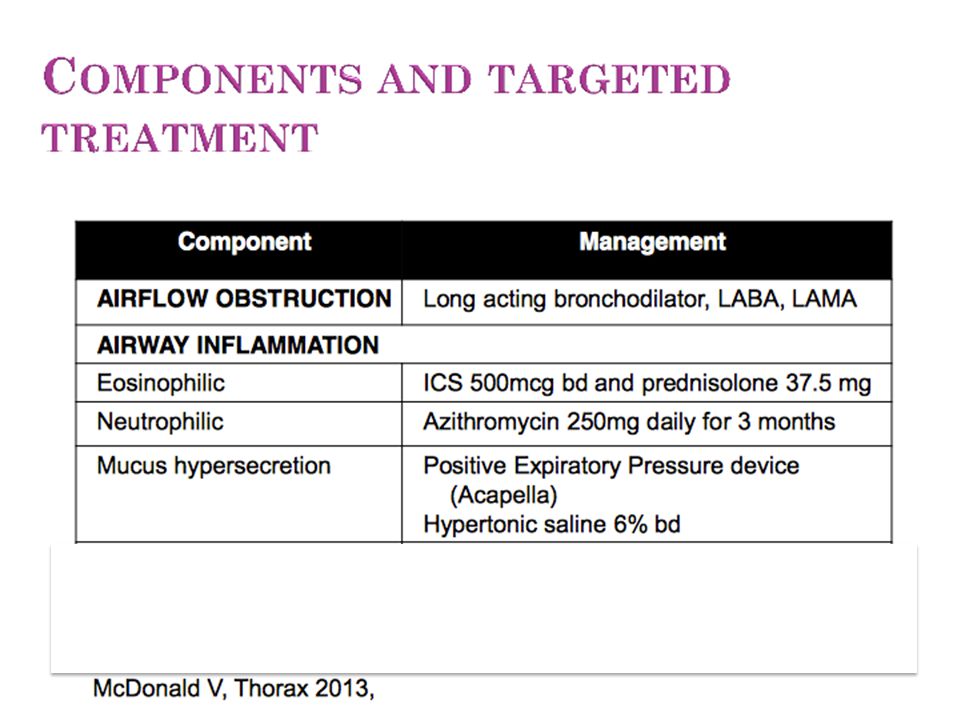
Acute exacerbations of COPD: heterogeneity
Phenotype van COPD exacerbaties Studies tonen aan dat 20-30% van de COPD pt een eosinofiele inflammatie bezitten --> eosinofiele bronchitis --> die doen het dus beter met Predni/IHC Bafadhel M. et al, AJRCCM 2011; 184:

44
COPD exacerbation type predicts response to azithromycin
Predictors of Chronic Obstructive Pulmonary Disease Exacerbation Reduction in Response to Daily Azithromycin Therapy", American Journal of Respiratory and Critical Care Medicine, Vol. 189, No. 12 (2014), pp Dagelijks azithromycine 250mg/dag aan pt die in voorgaande jaar een AECOPD hebben gedaan die minimaal cortico’s/hospitalisatie/spoedbezoek/O2 nodig hadden. Azithromycin was most effective in reducing AECOPD requiring both antibiotic and steroid treatment (n = 1,113; cumulative incidence analysis, P = ; recurrent events analysis, P = 0.002). M. Han et al, AJRCCM 2014.
, pp Dagelijks azithromycine 250mg/dag aan pt die in voorgaande jaar een AECOPD hebben gedaan die minimaal cortico’s/hospitalisatie/spoedbezoek/O2 nodig hadden. Azithromycin was most effective in reducing AECOPD requiring both antibiotic and steroid treatment (n = 1,113; cumulative incidence analysis, P = ; recurrent events analysis, P = 0.002). M. Han et al, AJRCCM")
46
Azithromycin prevents exacerbations of COPD
Dagelijks Azi 250mg: aan COPD pt, FU 1 jaar. A total of 1577 subjects were screened. --> Among selected subjects with COPD, azithromycin taken daily for 1 year, when added to usual treatment, decreased the frequency of exacerbations and improved quality of life but caused hearing decrements in a small percentage of subjects. Although this intervention could change microbial resistance patterns, the effect of this change is not known. Albert R. et al, NEJM 2011.

47
Significante reductie in exacerbaties in pt onder azithromycine vs placebo: HR 0,58 p 0,001
Number needed to treat om 1 pt te vrijwaren van een exacerbatie = 5! DE kracht van de studie= dat het allemaal pt waren die frequent exacerbeerden >3= per jaar, slechts 7% in de controle groep had geen exacerbatie tijdens verloop van de studie (1 jaar). HOE? Azi: macrolide met immunomodulaire eigenschappen/anti-inflammatoire eigenschappen Azi accumuleert in de neutrofielen en phagocyten in een 200x hogere concentratie dan extracell. --> als die cellen gerecruteerd worden naar een site van infectie/injury: dus wordt ook azi snel en in hoge conc afgeleverd aan de luchtwegen bi COPD pt Macroliden resistance ontwikkelt zich wel in populaties frequent blootgesteld aan macroliden. Echter betekenis van macroliden resistente kiemen voor een persoon is niet duidelijk. + er werden geen aan deze macroliden-resistentie gekoppelde adverse events gevonden bij pt met CF/non-CF bronchiectasieen/COPD. Goede tolernatie op GI vlak in COLUMBUS. Echter geen aandacht voor Cardiovasculair toxische neveneffecten/gehoorsverlies (verlengd Qtc). Hoe lang dat je het moet geven voor verdere protectie blijft onduidelijk.
. HOE Azi: macrolide met immunomodulaire eigenschappen/anti-inflammatoire eigenschappen. Azi accumuleert in de neutrofielen en phagocyten in een 200x hogere concentratie dan extracell. --> als die cellen gerecruteerd worden naar een site van infectie/injury: dus wordt ook azi snel en in hoge conc afgeleverd aan de luchtwegen bi COPD pt. Macroliden resistance ontwikkelt zich wel in populaties frequent blootgesteld aan macroliden. Echter betekenis van macroliden resistente kiemen voor een persoon is niet duidelijk. + er werden geen aan deze macroliden-resistentie gekoppelde adverse events gevonden bij pt met CF/non-CF bronchiectasieen/COPD. Goede tolernatie op GI vlak in COLUMBUS. Echter geen aandacht voor Cardiovasculair toxische neveneffecten/gehoorsverlies (verlengd Qtc). Hoe lang dat je het moet geven voor verdere protectie blijft onduidelijk.")
48
Stepwise treatment of COPD according to Severity: spirometry, symptoms, exacerbations
Maintenance: LAMA and LABA Plus: ICS and/or 2) AZI Smoking cessation Vaccination (influenza) Patient education Self-management Pulmonary rehabilatation: if mMRC ≥ 2 Oxygen therapy: if PaO2 < 60 mmHg Maintenance: LAMA and LABA Maintenance: LAMA or LABA Reliever: SAMA or SABA STEP 3 Spiro 3 or 4 ≤ 1 exac STEP 4 Spiro 2, 3 or 4 mMRC ≥ 2 ≥ 2 exac STEP 1 Spiro 1 or 2 mMRC < 2 No exac STEP 2 Spiro 1 or 2 mMRC ≥ 2 ≤ 1 exac SABA ± SAAC SOS
 AZI. Smoking cessation. Vaccination (influenza) Patient education. Self-management. Pulmonary rehabilatation: if mMRC ≥ 2. Oxygen therapy: if PaO2 < 60 mmHg. Maintenance: LAMA. and. LABA. Maintenance: LAMA. or. LABA. Reliever: SAMA. or. SABA. STEP 3. Spiro 3 or 4. ≤ 1 exac. STEP 4. Spiro 2, 3 or 4. mMRC ≥ 2. ≥ 2 exac. STEP 1. Spiro 1 or 2. mMRC < 2. No exac. STEP 2. Spiro 1 or 2. mMRC ≥ 2. ≤ 1 exac. SABA ± SAAC SOS.")
49
Nieuwe inhalatoren Zie hand-outs

50
LAMA

51
ICS+LABA

52
LAMA+LABA

53
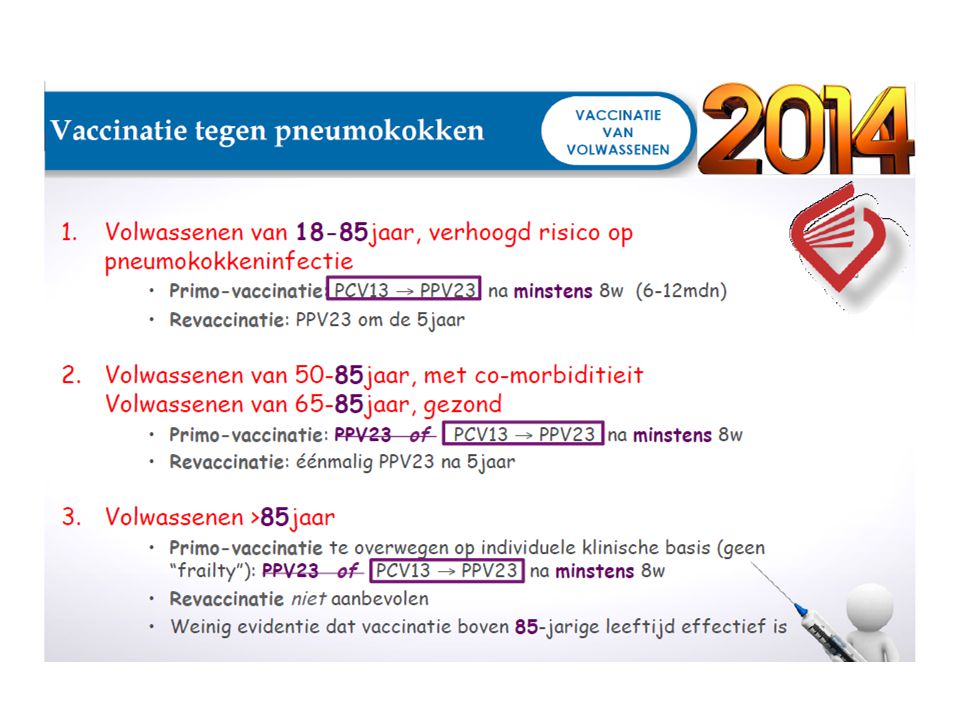
Pneumococcen vaccin? GOLD Hoge raad
Influenza vaccines can reduce serious illness. Pneumococcal polysaccharide vaccine is recommended for COPD patients 65 years and older and for COPD patients younger than age 65 with an FEV1 < 40% predicted Hoge raad Nieuwe publicatie 10/2/2015 Aanpassingen obv Capita studie

54
OUDE RICHTLIJN Oude richtlijn

57
niet

58
niet

59
Acetylcysteïne GOLD 2015 Pantheon Lancet 2014
Hoge dosis NAC: significant minder exa in GOLD II Pantheon Lancet 2014 GOLD In patients treated with and without inhaled corticosteroids, high doses of N-acetylcysteine significantly reduced exacerbation rates, but only in GOLD stage 2 patients594. Reference 594: Zheng JP, Wen FQ, Bai CX, Wan HY, Kang J, Chen P, et al; PANTHEON study group. Twice daily N-acetylcysteine 600 mg for exacerbations of chronic obstructive pulmonary disease (PANTHEON): a randomised, double-blind placebo-controlled trial. Lancet Respir Med 2014 Mar;2(3): Bij GOLD II en III = -22% exacerbaties
* Bij GOLD II (matig) = -39% exacerbaties antioxidativeandanti-inflammatoryproperties, and mucolytic activity, might be effective for treatment of COPD. N-acetylcysteine is a well-known, effective mucolytic drug that reduces sputum viscosity and elasticity, improves mucociliary clearance and modulates the inflammatory response.5,6 Furthermore, N-acetylcysteine has both direct and indirect antioxidant properties
: a randomised, double-blind placebo-controlled trial. Lancet Respir Med 2014 Mar;2(3): Bij GOLD II en III = -22% exacerbaties * Bij GOLD II (matig) = -39% exacerbaties. antioxidativeandanti-inflammatoryproperties, and mucolytic activity, might be effective for treatment of COPD. N-acetylcysteine is a well-known, effective mucolytic drug that reduces sputum viscosity and elasticity, improves mucociliary clearance and modulates the inflammatory response.5,6 Furthermore, N-acetylcysteine has both direct and indirect antioxidant properties.")
60
Resultaten6 PANTHEON-studie: The Lancet, 2014 -22%
Aantal exacerbaties per behandelingsperiode COPD-patiënten in GOLD-stadia II en III -22% 6. Zhen J-P, et al. Twice daily N-acetylcysteine 600 mg for exacerbations of chronic obstructive pulmonary disease (PANTHEON): a randomised, double-blind placebo-controlled trial. Lancet Respir Med Mar;2(3): Zambon Gamme 10 tabs Mode d’action Objectifs Méthode Résultats Conclusion Résumé Objectifs Méthode Résultats Conclusions Notices
: a randomised, double-blind placebo-controlled trial. Lancet Respir Med Mar;2(3): Zambon. Gamme. 10 tabs. Mode d’action. Objectifs. Méthode. Résultats. Conclusion. Résumé. Objectifs. Méthode. Résultats. Conclusions. Notices.")
61
Jaarlijks aantal exacerbaties per GOLD-stadium
PANTHEON-studie: The Lancet, 2014 Resultaten6 Jaarlijks aantal exacerbaties per GOLD-stadium NAC vermindert het jaarlijks aantal exacerbaties van COPD-patiënten in GOLD-stadium II (matig) met 39 % -39% NAC 1200 mg vs Placebo - Gold Mod. < (0.48,0.77) VERBETERING VAN DE KLINISCHE TOESTAND VAN DE PATIËNT IN DE GOLD-STADIA II EN III 6. Zhen J-P, et al. Twice daily N-acetylcysteine 600 mg for exacerbations of chronic obstructive pulmonary disease (PANTHEON): a randomised, double-blind placebo-controlled trial. Lancet Respir Med Mar;2(3): Zambon Gamme 10 tabs Mode d’action Objectifs Méthode Résultats Conclusion Résumé Objectifs Méthode Résultats Conclusions Notices
 met 39 % -39% NAC 1200 mg vs Placebo - Gold Mod. < (0.48,0.77) VERBETERING VAN DE KLINISCHE TOESTAND VAN DE PATIËNT IN DE GOLD-STADIA II EN III. 6. Zhen J-P, et al. Twice daily N-acetylcysteine 600 mg for exacerbations of chronic obstructive pulmonary disease (PANTHEON): a randomised, double-blind placebo-controlled trial. Lancet Respir Med Mar;2(3): Zambon. Gamme. 10 tabs. Mode d’action. Objectifs. Méthode. Résultats. Conclusion. Résumé. Objectifs. Méthode. Résultats. Conclusions. Notices.")
62
Take home messages Nieuwe GOLD: leiddraad Maar in GOLD C en D
LAMA+LABA staan op de eerste plaats bij GOLD C-D IHC pro’s en con’s Dosis te hoog? WISDOM: 1 jaar geen exacerbatie --> afbouwen = veilig COLUMBUS: Azithromycine: >= 2-3 exa per jaar NAC in GOLD 2: significante daling van exacerbaties Pneumococcen vaccinatie: nieuwe aanbeveling van de Hoge Raad

63
Take home messages Verdere studies nodig
predictoren voor IHC/azithromycine behandeling? Eosinofielen (referentie Brusselle) > > IHC: 30% minder exacerbaties < > IHC geen daling van exacerbaties, eerder meer pneumonieen Eerdere behandeling (cortico’s+AB) --> azi gevoelig
 > > IHC: 30% minder exacerbaties. < > IHC geen daling van exacerbaties, eerder meer pneumonieen. Eerdere behandeling (cortico’s+AB) --> azi gevoelig.")
Verwante presentaties
>")















 bij MS>")


