Download de presentatie
De presentatie wordt gedownload. Even geduld aub

1
Dr. A. Breugelmans Diensthoofd Urologie RZ Heilig Hart Leuven
OVERACTIEVE BLAAS O.A.B. 14 april 2010 Dr. A. Breugelmans Diensthoofd Urologie RZ Heilig Hart Leuven

2
Urineverlies – Talrijke mythes
MYTH: PREVENTION IS IMPOSSIBLE MYTH: INDWELLING CATHETERS ARE THE BEST INTERVENTION FOR INTRACTABLE URINARY INCONTINENCE MYTH: THERE ARE NO EFFECTIVE TREATMENTS FOR URINARY INCONTINENCE-IT'S UNAVOIDABLE IN NURSING HOME RESIDENTS MYTH: THERE IS ONLY ONE TYPE OF URINARY INCONTINENCE MYTH: URINARY INCONTINENCE IS UNMANAGEABLE IN PEOPLE WITH DEMENTIA MYTH: COMPLETE CONTINENCE IS THE ONLY INDICATION OF SUCCESSFUL TREATMENT MYTH: URINARY INCONTINENCE FALLS UNDER THE PURVIEW OF PHYSICIANS; NURSES CAN'T DO MUCH TO HELP MYTH: URINARY INCONTINENCE IS INEVITABLE WITH AGE MYTH: OLDER ADULTS DON'T MIND BEING INCONTINENT AND WEARING PADS

3
Urineverlies – Evenveel oorzaken

4
Urineverlies – Evenveel oorzaken
D elirium, dementia, deconditionering I nfection, inflammation A trophy of the vagina /urethra P harmaceuticals, psychologic (depression) E xcessive urine output (Cong.Heart Failure, diabetes) R estricted mobility S tool impaction, sacral nerve root pathology
 E xcessive urine output (Cong.Heart Failure, diabetes) R estricted mobility. S tool impaction, sacral nerve root pathology.")
5
Urineverlies - Vormen Inspanning Urge Mixed Overloop Continue
Centraal/Emotioneel (decorumverlies)
")
6
Incontinentie / Residu
+ residu : - BOOS - neurogene hypotonie (VSD, medicatie, L, hysterie) - residu : - UWI sensorisch - atrofische vaginitis - fecale impactie - O.A.B.
 - residu : - UWI sensorisch. - atrofische vaginitis. - fecale impactie. - O.A.B.")
7
Inspanningsurineverlies
Zwakke sluiting (anatomisch / functioneel) Bekkenbodemspieroefeningen Alfa-adrenergica (+/- anticholinergica) TVT ea
 Bekkenbodemspieroefeningen. Alfa-adrenergica. (+/- anticholinergica) TVT ea.")
8
Theorie van Enhorning (druktransmissie)
")
9
Integrale Theorie van Ulmsten

10
Principe van de BH-suspensie
Continente patiënt Incontinente patiënt

11
Principe van de BH-suspensie

12
Situering van de overactieve blaas

13
Urgentie Incontinentie
Overactieve blaas Incontinentie Urgentie Frequency 8 or more visits to the toilet per 24 hours Nocturia 2 or more visits to toilet during sleeping hours Stress Incontinentie Frequentie “symptom syndrome suggestive of lower urinary tract dysfunction” Nycturie Gemengde symptomen (Abrams et al. Neurourol Urodyn 21: , 2002); Milsom I, et al. BJU Int. 2001;87:
; Milsom I, et al. BJU Int. 2001;87:")
14
2 TYPES O.A.B. “DROOG” “NAT”
Patienten met urgentie, frequentie of nycturie: Patienten met urgentie incontinentie: Normale patiënt “DROOG” “NAT”

15
Elderly: “STERK EN LUI ???”
detrusor hyperactivity with impaired bladder contractility is common (DHIC) involuntary detrusor contractions, yet must strain to empty their bladders either incompletely or completely.
 involuntary detrusor contractions, yet must strain to empty their bladders either incompletely or completely.")
16
ETIOLOGIE

17
O.A.B. - Neurogene Theorie
Blaasvulling : sensorisch motorisch Mictiefaze Blaasdruk Normale plasdrang Blaas vulling Eerste plasgevoel Blaas vulling The normal micturition cycle consists of a storage phase and an emptying phase. The storage phase encompasses bladder filling, the first sensation to void, and the desire to void. During bladder filling, urethral resistance is increased as a result of activation of the urethral sphincters by spinal reflexes. The emptying phase is characterized by a volitional contraction of the detrusor muscle (immediately preceded by urethral sphincter relaxation), leading to a rise in bladder pressure and emptying of the bladder. As the bladder begins to refill, the cycle is repeated. Wein AJ, Rovner ES. Int J Fertil. 1999;44:56-66. Wein AJ, Rovner ES. The overactive bladder: an overview for primary care health providers. Int J Fertil. 1999;44:56-66.
, leading to a rise in bladder pressure and emptying of the bladder. As the bladder begins to refill, the cycle is repeated. Wein AJ, Rovner ES. Int J Fertil. 1999;44: Wein AJ, Rovner ES. The overactive bladder: an overview for primary care health providers. Int J Fertil. 1999;44:")
18
Normale Mictie Controle
Para (Voiding) Ortho (Filling) Adapted from Opsomer RJ., Lorge F., 1999
 Ortho (Filling) Adapted from Opsomer RJ., Lorge F.,")
19
Bezenuwing van de lagere urinewegen
Abrams P, Wein AJ. The Overactive Bladder—A Widespread and Treatable Condition Detrusorspier Sympathisch Parasympathisch Somatisch Externe sfincter Bekkenbodemspier Centraal zenuwstelsel

20
During bladder filling distension results in afferent pelvic discharge; after synapse in pudendal nucleus efferent pudendal impulses produce contraction of external sphincter helping to maintain continence. Other efferent sympathetic fibres synapse in post ganglionic parasympathetic neuron, resulting in inhibition of detrusor contraction. Afferent pelvic nerve discharges ascend in spinal cord, synapse in pontine micturition centre Descending efferent pathways cause Inhibition of pudendal firing - relaxation of sphincter Inhibition of sypathetic firing - opens bladder neck pelvic parasypathetic firing - detrusor contraction

21
Neurotransmitters + receptoren
Cholinerge receptoren Adrenerge receptoren Nicotine receptoren (N) Muscarine receptoren a- adrenerge receptoren b-adrenerge receptoren a1,a2,a3,...,an b1,b2,b3,..,bn M1, M2, M4, M5 M3
 Muscarine receptoren. a- adrenerge receptoren. b-adrenerge receptoren. a1,a2,a3,...,an. b1,b2,b3,..,bn. M1, M2, M4, M5. M3.")
22
Myogene Theorie Autonome Theorie

23
UROTHEEL

24
TRP-kanalen (Elaut, 2009) Transient receptor potential channels
Ionenkanalen Activatie: fysisch (T), mechanische stress, Chemisch (pH, osmol.) ZINTUIGEN VAN DE CEL
, mechanische stress, Chemisch (pH, osmol.) ZINTUIGEN VAN DE CEL.")
25
PREVALENTIE en BELANG

26
US NOBLE Study Stewart WF et al. 2003
Prevalentie van O.A.B. EU Study Milsom I et al. 2001 US NOBLE Study Stewart WF et al. 2003 45 40 40 35 Men 35 Men 30 Women Women 30 25 25 20 Prevalence, % 20 Prevalence, % 15 15 10 10 References: Milsom I, Abrams L, Cardozo L, Roberts RG, Thuroff J, Wein J. How widespread are the symptoms of an overactive bladder and how are they managed? A population-based prevalence study. BJU Int. 2001;87: Stewart WF, Van Rooyen JB, Cundiff GW, et al. Prevalence and burden of overactive bladder in the US. World J Urol. 2003;20: 5 5 40–44 45–49 50–54 55–59 60–64 65–69 70–74 75+ 18-24 25-34 35-44 45-54 55-64 65-74 75+ Age, years Age, years 1 op twaalf volwassenen lijdt aan de symptomen van overactieve blaas: dit is meer dan bij osteoporose of de ziekte van Alzheimer Epidemiological research done in 6 EU countries (France, Germany, Italy, Sweden, UK, Spain) Milsom I et al. BJU Int. 2001;87: Stewart WF et al. World J Urol. 2003;20:
 Milsom I et al. BJU Int. 2001;87: Stewart WF et al. World J Urol. 2003;20:")
27
EUROPEAN UROLOGY Volume 57, issue 4, pages , April Voiding Dysfunction A Comparison of the Frequencies of Medical Therapies for Overactive Bladder in Men and Women: Analysis of More Than 7.2 Million Aging Patients Brian T. Helfand a, R. Mark Evans b, Kevin T. McVary a .

28
Klachten ??? (Sickness or aging – Cicero 44AD)
10 20 30 40 50 60 70 80 90 Not Worth Bothering a Doctor About Not Really a Medical Condition Can’t Be Cured or Helped Natural Part of Aging A Sign of a More Serious Medical Condition Hereditary, So It Can’t Be Helped A Result of the Way I Live Ignored by the Medical Community Something Few People My Age Have Something You Have to Learn to Live With Total Women Men * Urinary Problems Like Mine Are… Reference: Irwin DE, Milsom I, Kopp Z, Abrams P, Cardozo L. Impact of overactive bladder symptoms on employment, social interactions and emotional well-being in 6 European countries. BJU Int. 2006;97: Percentage of Subjects *P≤.05 vs men. Irwin DE et al. BJU Int. 2006;97:

29
? ? Kostprijs (verbandmateriaal, medicatie) Geen totale genezing
Onwetend over mogelijke behandeling (“mythes”) Beschaamd om erover te spreken Aanpassing levensstijl France Germany Italy Spain UK Japan US Total Prevalence (000s) 7852.7 8751.2 9127.4 57,125.6 Percent Diagnosed 5% Total Diagnosed Population (000s) 409.9 642.9 704.2 456.8 476.5 757.7 2,982.0 Percent Drug Treated 36% Total Drug-Treated Population (000s) 147.6 231.4 253.5 164.5 171.5 272.8 1,073.5 Percent Compliant 25% 20% Total Compliant Population (000s) 36.9 57.9 63.4 41.1 42.9 54.6 268.4 ? Kostprijs (verbandmateriaal, medicatie) Geen totale genezing Neveneffecten medicatie
 Beschaamd om erover te spreken. Aanpassing levensstijl. France. Germany. Italy. Spain. UK. Japan. US. Total Prevalence (000s) , Percent Diagnosed. 5% Total Diagnosed Population (000s) , Percent Drug Treated. 36% Total Drug-Treated Population (000s) , Percent Compliant. 25% 20% Total Compliant Population (000s) Kostprijs (verbandmateriaal, medicatie) Geen totale genezing. Neveneffecten medicatie.")
30
OAB en levenskwaliteit
Beroepsmatig Sociaal Sexueel Impact van de OAB op levenskwaliteit Fysisch Huiselijk Emotioneel

31
Co-morbidities Associated With OAB Results From the EPIC Study
Men 35 * 30 OAB cases (n = 502) 25 Controls (n = 502) * 20 15 * * 10 * * 5 Obesity Hypertension Depression Asthma Diabetes Chronic constipation Neurologic conditions Subjects, % Dyslipidemie 30 * Women 25 * The EPIC study was a cross-sectional, population-based survey of adults (N=19,165) in 5 countries including Canada, Germany, Italy, Sweden, and the United Kingdom. Computer assisted telephone interviews were conducted using a geographically stratified random sample of the population. ICS definitions of OAB and lower urinary tract symptoms were used to classify participants. A nested case-control analysis was performed on data collected from participants with OAB (cases; n=1434) and without OAB (controls; n=1434). Cases and controls were matched for sex, country, and 5-year age groups. Participants were asked to report a history of chronic constipation or physician diagnoses of asthma, diabetes, hypertension, neurologic conditions (multiple sclerosis, stroke, parkinsonism), or depression. Respondents also noted their height, weight, and diuretic use. Body mass index (BMI) was calculated according to the World Health Organization criteria, and participants were classified as underweight, normal weight, overweight, obese, or very obese. Prevalence odds ratios and 95% confidence intervals were calculated using logistic regression models. Several factors were significantly associated with reported OAB in bivariate analyses. In multivariate analyses, neurologic conditions, chronic constipation, depression, and obesity were significantly associated with OAB after controlling for age, sex, and country. Several common chronic health conditions were significantly more prevalent in cases than in controls, including chronic constipation, neurologic conditions, depression, and obesity, even after adjusting for covariates such as age, sex and country. Reference: Irwin DE, Milsom I, Kopp Z, Herschorn S, Artibani W. Comorbidities associated with overactive bladder: results from the EPIC study. Neurourol Urodyn Poster 141. Presented at the 37th Annual Meeting of the International Continence Society; August 20-14, 2007; Rotterdam, Netherlands. OAB cases (n = 932) 20 * Controls (n = 932) 15 * * 10 * 5 * Obesity Hypertension Depression Asthma Diabetes Chronic constipation Neurologic conditions *P ≤ 0.05 vs. controls (within gender). Irwin DE et al. Presented at ICS 2007
 25. Controls (n = 502) * * * 10. * * 5. Obesity. Hypertension. Depression. Asthma. Diabetes. Chronic constipation. Neurologic conditions. Subjects, % Dyslipidemie. 30. * Women. 25. * The EPIC study was a cross-sectional, population-based survey of adults (N=19,165) in 5 countries including Canada, Germany, Italy, Sweden, and the United Kingdom. Computer assisted telephone interviews were conducted using a geographically stratified random sample of the population. ICS definitions of OAB and lower urinary tract symptoms were used to classify participants. A nested case-control analysis was performed on data collected from participants with OAB (cases; n=1434) and without OAB (controls; n=1434). Cases and controls were matched for sex, country, and 5-year age groups. Participants were asked to report a history of chronic constipation or physician diagnoses of asthma, diabetes, hypertension, neurologic conditions (multiple sclerosis, stroke, parkinsonism), or depression. Respondents also noted their height, weight, and diuretic use. Body mass index (BMI) was calculated according to the World Health Organization criteria, and participants were classified as underweight, normal weight, overweight, obese, or very obese. Prevalence odds ratios and 95% confidence intervals were calculated using logistic regression models. Several factors were significantly associated with reported OAB in bivariate analyses. In multivariate analyses, neurologic conditions, chronic constipation, depression, and obesity were significantly associated with OAB after controlling for age, sex, and country. Several common chronic health conditions were significantly more prevalent in cases than in controls, including chronic constipation, neurologic conditions, depression, and obesity, even after adjusting for covariates such as age, sex and country. Reference: Irwin DE, Milsom I, Kopp Z, Herschorn S, Artibani W. Comorbidities associated with overactive bladder: results from the EPIC study. Neurourol Urodyn Poster 141. Presented at the 37th Annual Meeting of the International Continence Society; August 20-14, 2007; Rotterdam, Netherlands. OAB cases (n = 932) 20. * Controls (n = 932) 15. * * 10. * 5. * Obesity. Hypertension. Depression. Asthma. Diabetes. Chronic constipation. Neurologic conditions. *P ≤ 0.05 vs. controls (within gender). Irwin DE et al. Presented at ICS")
32
DIAGNOSE

33
Diagnose Anamnese KO Urine Mictiedagboek Beeldvorming Urodynamica

34
Anamnese Ziekten? Medicatie? Operatief? Bevallingen?
Drinkgewoonte, plasgedrag MOBILITEIT? CONSTIPATIE?

35
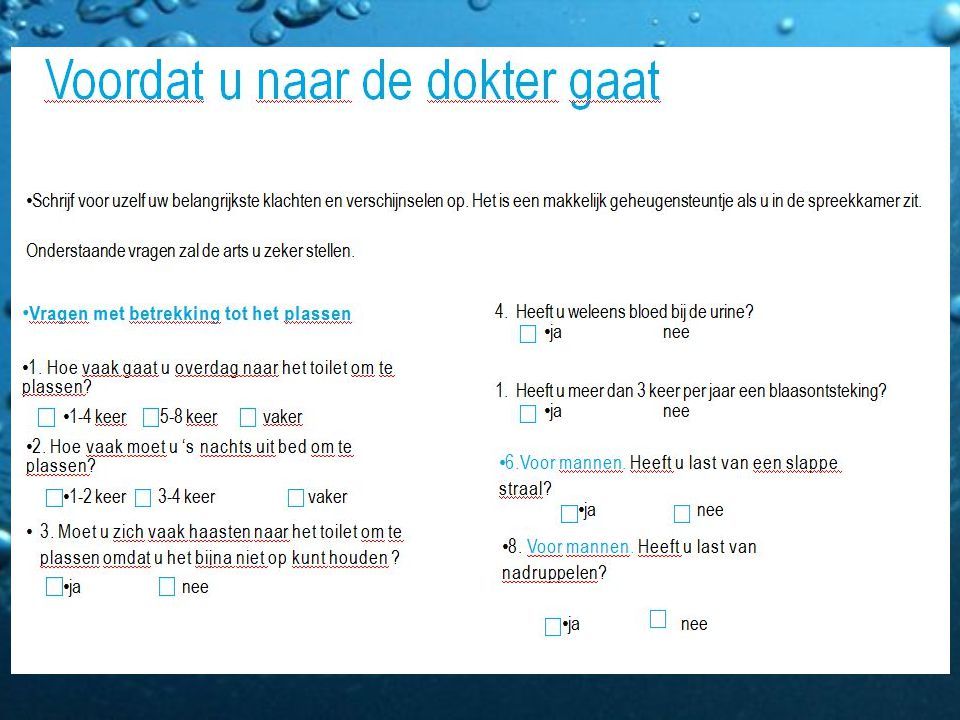
Sleutelvragen voor de patiënt
Hoe vaak gaat u in totaal naar het toilet gedurende een periode van 24 uur? – PLAST U VAAK ? Hoe vaak staat u ‘s nachts op om naar het toilet te gaan? Hoe vaak overdag voelt u een plotse en sterke drang om te plassen? Komt u vaak te laat op het toilet? Verliest u urine (HNP??) ? Gebruikt u inlegverbanden? Hebt u regelmatig “blaasontstekingen” ? Abrams P, et al. Am J Manag Care. 2000;6(suppl):S580-S590. Chapple C., Pocket Reference to Overactive Bladder, 2007, Current Medicine Group
 Gebruikt u inlegverbanden Hebt u regelmatig blaasontstekingen Abrams P, et al. Am J Manag Care. 2000;6(suppl):S580-S590. Chapple C., Pocket Reference to Overactive Bladder, 2007, Current Medicine Group.")
38
OAB-V8 questionnaire

39
Heeft u onge- lukjes gehad?
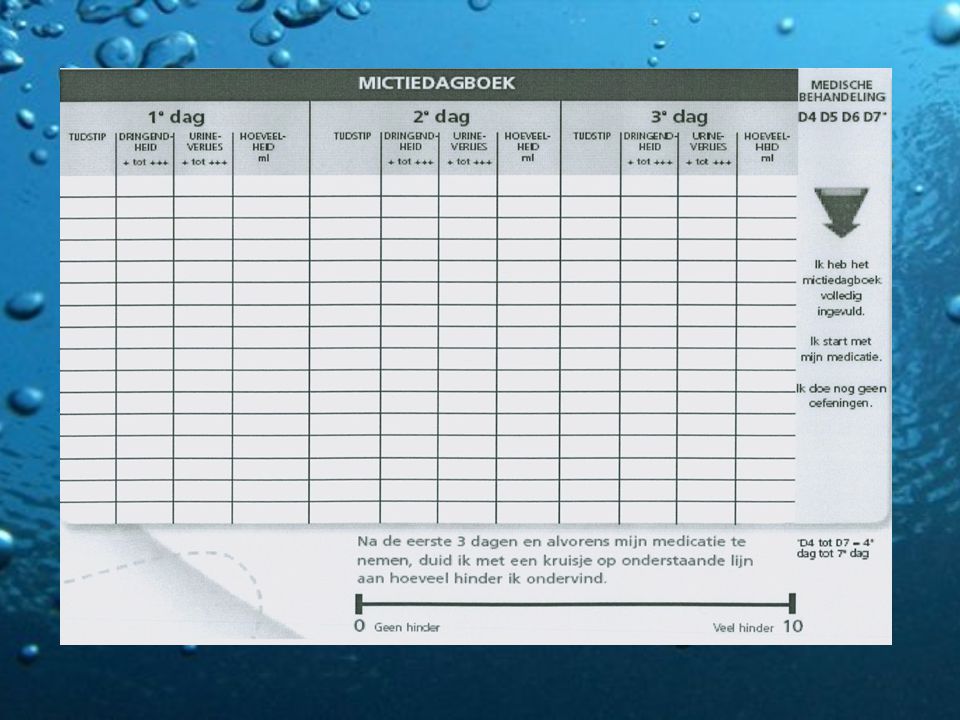
Plasdagboek – Volumedagboek – Mictiedagboek (3-7d) Dag 1 Tijdstip Gedronken Moest u plassen? Ongewenst urineverlies Wat heeft u gedronken en hoeveel? Hoeveel keer? Hoeveelheid urine (minimaal, gemiddeld, veel) Voelde u een plotselinge aandrang? Waar was u op dit moment mee bezig? Heeft u onge- lukjes gehad? Hoeveelheid urine heeft u verloren? (minimaal, gemiddeld, veel) Wat was u op dat moment aan het doen? uur Koffie, 1 kopje 2 gemiddeld ja nee Op visite bij mijn dochter minimaal aan het eten uur uur uur uur uur uur uur uur uur uur uur
 Dag 1. Tijdstip Gedronken Moest u plassen Ongewenst urineverlies. Wat heeft u gedronken en hoeveel Hoeveel keer Hoeveelheid urine (minimaal, gemiddeld, veel) Voelde u een plotselinge aandrang Waar was u. op dit moment mee bezig Heeft u onge- lukjes gehad Hoeveelheid urine heeft u verloren (minimaal, gemiddeld, veel) Wat was u op dat moment. aan het doen uur. Koffie, 1 kopje. 2. gemiddeld. ja. nee. Op visite bij mijn dochter. minimaal. aan het eten uur uur uur uur uur uur uur uur uur uur uur.")
41
Klinisch Onderzoek Abdominaal Neurologisch Pelvisch (vrouw)
Genitaal/prostaat (man)
")
42
Zijn anticholinergica veilig bij BPH???
… Nota: Bij de man … BPH BOO ischemie cholinerge denervatie detrusor-overactiviteit Zijn anticholinergica veilig bij BPH???

43
Urine-analyse Pyurie Bacteriurie Hematurie Proteinurie Glucosurie

44
Beeldvorming Echografie: blaaswanddikte, residu, RIP; ∆HUW??
IVU, cystogram CT-scan

45
Specifiek urologisch onderzoek
Indien discordantie tussen anamnese, KO en eventuele proefbehandeling Residubepaling Uroflowmetrie Cystometrie Cystoscopie

46
Urodynamisch onderzoek

47
Urodynamisch onderzoek

48
Urodynamisch onderzoek

49
BEHANDELING

50
Behandeling Gedrag Anticholinergica Topica vaginaal
Pelvische reëducatie

51
Resistente vormen van O.A.B.
Neuromodulatie S3 (eerst test onder LA) TENS / SANS: transcutaneous electric nerve stimulator BotulineToxine remt het vrijkomen van acetylcholine uit de synaps —> tijdelijke chemodenervatie met spierrelaxatie. Duur / herhaling / retentie Hydrodistentie Blaasvergrotingsplastie
 TENS / SANS: transcutaneous electric nerve stimulator. BotulineToxine. remt het vrijkomen van acetylcholine uit. de synaps —> tijdelijke chemodenervatie. met spierrelaxatie. Duur / herhaling / retentie. Hydrodistentie. Blaasvergrotingsplastie.")
52
Gedragstherapie Regulatie van de vochtinname Blaastraining
Naar het toilet gaan op voorafbepaalde tijdstippen Onderbreken tijdens het plassen “Voiding by time and not by desire” (blaasinhoud) Spiertraining van de bekkenbodem
 Spiertraining van de bekkenbodem.")
53
Gedragstherapie “Lifestyle changes” Let op met caffeine en alcohol
Drink “voldoende” Mobiliteit Andere gezondheids- problemen (D-I-A-P-E-R-S) Behavior modification is the foundation of OAB treatment, of which bladder retraining is an important component. The goal of bladder retraining is to restore bladder control by increasing bladder capacity. The primary tool in this approach is a voiding diary. Patients are asked to gradually increase the interval between voids by practicing maneuvers designed to inhibit the micturition reflex. Patients use a voiding diary to keep track of their micturitions and progress. Lifestyle changes are also an important part of behavior modification, because such changes can directly impact treatment success. For example, caffeine and alcohol are irritants that trigger the need to void. Taking steps to increase bladder capacity without avoiding caffeine and alcohol is counterproductive. Likewise, patients are encouraged to decrease their fluid intake to reduce the need to void, especially fluid intake before bedtime. It also makes sense to help patients, particularly elderly patients, improve their mobility so it is easier for them to get to the toilet. It is also important to address other health issues, particularly those that may also impact bladder functioning. Wein AJ, Rovner ES. Int J Fertil. 1999;44:56-66. Chapple C., Pocket Reference to Overactive Bladder, 2007, Current Medicine Group Wein AJ, Rovner ES. The overactive bladder: an overview for primary care health providers. Int J Fertil. 1999;44:56-66.
 Behavior modification is the foundation of OAB treatment, of which bladder retraining is an important component. The goal of bladder retraining is to restore bladder control by increasing bladder capacity. The primary tool in this approach is a voiding diary. Patients are asked to gradually increase the interval between voids by practicing maneuvers designed to inhibit the micturition reflex. Patients use a voiding diary to keep track of their micturitions and progress. Lifestyle changes are also an important part of behavior modification, because such changes can directly impact treatment success. For example, caffeine and alcohol are irritants that trigger the need to void. Taking steps to increase bladder capacity without avoiding caffeine and alcohol is counterproductive. Likewise, patients are encouraged to decrease their fluid intake to reduce the need to void, especially fluid intake before bedtime. It also makes sense to help patients, particularly elderly patients, improve their mobility so it is easier for them to get to the toilet. It is also important to address other health issues, particularly those that may also impact bladder functioning. Wein AJ, Rovner ES. Int J Fertil. 1999;44: Chapple C., Pocket Reference to Overactive Bladder, 2007, Current Medicine Group. Wein AJ, Rovner ES. The overactive bladder: an overview for primary care health providers. Int J Fertil. 1999;44:")
54
TIPS VOOR DE PATIËNT Wat kan je zelf hieraan doen? Ga altijd naar je huisarts; je loopt steeds gevaar voor een infectie. Hou enkele dagen een plaskalender bij; noteer wanneer en hoeveel je plast. Noteer ook hoeveel je drinkt en wat de klachten zijn. Dit kan helpen om de oorzaak te vinden. Draag kleding die je snel kan losmaken, bijvoorbeeld sluitingen met velcro of een rits in plaats van knopen

55
TIPS VOOR DE PATIËNT Drink voldoende overdag (1,5 à 2 liter) en weinig's avonds; dan moet je 's nachts niet opstaan om te plassen. Ga regelmatig plassen, om de 2 à 3 uur. Ga vooral niet minder drinken, want hierdoor verhoogt de kans op een blaasontsteking. Weinig drinken is bij wijze van uitzondering handig als je ergens naartoe gaat waar je niet kan plassen (bvb theater, sporten, ...) Onthoud dat geconcentreerde urine meer prikkelt en irriteert!!! Alcohol, cola, koffie, thee en light-dranken met aspartaam irriteren de blaaswand waardoor je nog meer moet plassen. Water is de beste drank!!!
 en weinig s avonds; dan moet je s nachts niet opstaan om te plassen. Ga regelmatig plassen, om de 2 à 3 uur. Ga vooral niet minder drinken, want hierdoor verhoogt de kans op een blaasontsteking. Weinig drinken is bij wijze van uitzondering handig als je ergens naartoe gaat waar je niet kan plassen (bvb theater, sporten, ...) Onthoud dat geconcentreerde urine meer prikkelt en irriteert!!! Alcohol, cola, koffie, thee en light-dranken met aspartaam irriteren de blaaswand waardoor je nog meer moet plassen. Water is de beste drank!!!")
56
Stoelgangspatroon !

57
Beperkingen van gedragstherapie
Vereist motivatie van patiënt en dokter/begeleider Succes afhankelijk van de intensiteit van het programma Gedragstherapie wordt best steeds gecombineerd met farmacotherapie voor de beste resultaten

58
Medicatie Anticholinergica (antimuscarinica) Antispasmodica
Fesoterodine Tolterodine Oxybutynin Trospium Darifenacin Solifenacin Antispasmodica Flavoxate Tricyclic antidepressants (Selective Serotonin Reuptake Inhibitors) Cymbalta, Yentreve Estrogens DESMOPRESSINE ???
 Cymbalta, Yentreve. Estrogens. DESMOPRESSINE")
59
Leeftijdsgebonden veranderingen
Verminderde blaascontractie Toenemende instabiliteit Verminderd aandrangevoel Verlaging urethrale tonus Verlaging BBStonus TOENAME NACHTELIJKE URINEPRODUCTIE

60
Desmopressine

61
NYCTURIE – desmopressine
Bewezen vermindering nycturie, nachtelijke polyurie en verbetering QoL Risico hyponatriëmie: 7.6% (3-20%) - snelle follow-up! : bloedanalyse D3 en D7 - exclusie cardiale, renale co-morbiditeit - geen andere medicatie die hyponatriëmie kan veroorzaken The elderly adult takes an average of 5 medications (not including vitamins) One study found that 10 of the top 25 prescribed drugs in the elderly had some anticholinergic properties Possible drug effects to consider are those that may cause symptoms that mimic those of OAB, from medications including diuretics and the antihypertensives. Treatment schedules can be manipulated to minimize possible complications between OAB therapies and these medications that also effect filling and voiding Other considerations include: effects from the acetylcholinesterase inhibitors, that primarily act on M1 receptors within the brain, but their effects on the micturition axis are unknown. anticholinergic adverse effects of medications, eg, the antidepressants, antihistamines, antipsychotics, and over‑the‑counter sleep aids like Tylenol PM® (acetaminophen and diphenhydramine). These effects may be augmented by the addition of an antimuscarinic agent. Thus, regimen’s must be scrutinized for potential interactions. Weatherall M. J Neurourol Urodyn 2004;23:
 - snelle follow-up! : bloedanalyse D3 en D7. - exclusie cardiale, renale co-morbiditeit. - geen andere medicatie die hyponatriëmie kan veroorzaken. The elderly adult takes an average of 5 medications (not including vitamins) One study found that 10 of the top 25 prescribed drugs in the elderly had some anticholinergic properties. Possible drug effects to consider are those that may cause symptoms that mimic those of OAB, from medications including diuretics and the antihypertensives. Treatment schedules can be manipulated to minimize possible complications between OAB therapies and these medications that also effect filling and voiding. Other considerations include: effects from the acetylcholinesterase inhibitors, that primarily act on M1 receptors within the brain, but their effects on the micturition axis are unknown. anticholinergic adverse effects of medications, eg, the antidepressants, antihistamines, antipsychotics, and over‑the‑counter sleep aids like Tylenol PM® (acetaminophen and diphenhydramine). These effects may be augmented by the addition of an antimuscarinic agent. Thus, regimen’s must be scrutinized for potential interactions. Weatherall M. J Neurourol Urodyn 2004;23:")
62
“Understanding Muscarinic Receptors”

63
“Understanding Muscarinic Receptors”

64
Distribution of Muscarinic Receptors in Target Organs of the Parasympathetic Nervous System
Iris/Ciliary body CNS Lacrimal gland Salivary glands Heart Gallbladder Stomach The differences in receptor subtype distribution are particularly important when considering the efficacy and side effects associated with antimuscarinic agents. M1, M4, and M5 receptor subtypes are found primarily, though not exclusively, in the central nervous system; M2 and M3 receptors are also present in the brain. Of note, M3, but not M2, receptors are present in various glands, including salivary, throughout the body. Blockade of muscarinic receptors in organs other than the bladder may result in undesired side effects such as dry mouth (the most common side effect), constipation, and impaired visual accommodation. Agents that are selective for the bladder are preferable over agents that block receptors in other regions of the body. Colon Bijwerkingen: centrale bijwerkingen, accomodatie stoornissen, glaucoom, droge mond, caries, constipatie Bladder Chapple CR, et al. Urology. 2002;60(suppl 5A):82-89. Caulfield MP. Pharmacol Ther. 1993;58: Parkman HP, et al. Am J Physiol Gastrointest Liver Physiol. 1999;39:G1243-G1250. Chapple CR, Yamanishi T, Chess-Williams R. Muscarinic receptor subtypes and management of the overactive bladder. Urology. 2002;60(suppl 5A):82-89. Caulfield MP. Muscarinic receptors—characterization, coupling and function. Pharmacol Ther. 1993;58: Parkman HP, Pagano AP, Ryan JP. Subtypes of muscarinic receptors regulating gallbladder cholinergic contractions. Am J Physiol Gastrointest Liver Physiol. 1999;39:G1243-G1250.
, constipation, and impaired visual accommodation. Agents that are selective for the bladder are preferable over agents that block receptors in other regions of the body. Colon. Bijwerkingen: centrale bijwerkingen, accomodatie stoornissen, glaucoom, droge mond, caries, constipatie. Bladder. Chapple CR, et al. Urology. 2002;60(suppl 5A): Caulfield MP. Pharmacol Ther. 1993;58: Parkman HP, et al. Am J Physiol Gastrointest Liver Physiol. 1999;39:G1243-G1250. Chapple CR, Yamanishi T, Chess-Williams R. Muscarinic receptor subtypes and management of the overactive bladder. Urology. 2002;60(suppl 5A): Caulfield MP. Muscarinic receptors—characterization, coupling and function. Pharmacol Ther. 1993;58: Parkman HP, Pagano AP, Ryan JP. Subtypes of muscarinic receptors regulating gallbladder cholinergic contractions. Am J Physiol Gastrointest Liver Physiol. 1999;39:G1243-G1250.")
65
Cardiaal risico ??? Retrospectieve cohort analyse
patiënten met urge incontinentie 65 jaar: mediane leeftijd ~ 79j Resultaten: geen associatie tussen gebruik urinaire anticholinergica en verhoogd risico op ventriculaire arrythmie of plotse dood Wang PS et al. J Am Geriatr Soc. 2002;50:

66
Anticholinergica en cognitieve achteruitgang
Acetylcholine is belangrijke mediator voor korte termijn geheugen Ook andere medicatie kan cognitieve achteruitgang veroorzaken (antihistaminica, antispasmodica, anti-psychotica) Dubbel blind, placebo gecontroleerde crossover studie: placebo, oxybutynine 5 mg en 10 mg (n = 12 gezonde vrijwilligers, leeftijd 65–76) Pleidooi voor meer selectieve anticholinergica !!! QUID A.c. en R/ Alzheimer (Aricept, cholinesterase-I) Drachman DA, et al. Neurobiol Aging. 1980;1:39-43. Katz IR, et al. J Am Geriatr Soc.1998;46:8-13.
 Dubbel blind, placebo gecontroleerde crossover studie: placebo, oxybutynine 5 mg en 10 mg (n = 12 gezonde vrijwilligers, leeftijd 65–76) Pleidooi voor meer selectieve anticholinergica !!! QUID A.c. en R/ Alzheimer (Aricept, cholinesterase-I) Drachman DA, et al. Neurobiol Aging. 1980;1: Katz IR, et al. J Am Geriatr Soc.1998;46:8-13.")
67
Passieve diffusie door de BBB
Vasculature BBB CNS Lipofiel, diffusie lading/polariteit, binding aan waterstof, diffusie Moleculaire afmeting, diffusie - + Pardridge WM. J Neurochem. 1998;70: Habgood MD, et al. Cell Mol Neurobiol. 2000;20:

68
Passieve diffusie door de BBB
Vasculatuur BBB CNS High lipophilicity, neutral, relatively “small” molecular structure Oxybutynin Low lipophilicity, charged, relatively bulky molecular structure + Fesoteridine, Tolteridine/actieve metaboliet + + + + + + + + ((Trospium chloride)) Highly polar + + + + + + + + + + + + + + + Dimpfel W. J Urol 2000;163(4):226 abstract.
) Highly polar Dimpfel W. J Urol 2000;163(4):226 abstract.")
69
Anticholinergica Oxybutinine: Ditropan, Kentera (5mg)
Tolderodine: Detrusitol, Detr. Retard (2/4mg) Solifenacine: Vesicare (5/10mg) Darifenacine: Emselex (7,5/15mg) Fesoterodine: Toviaz (4/8mg) “ERTUSSENIN”
 Solifenacine: Vesicare (5/10mg) Darifenacine: Emselex (7,5/15mg) Fesoterodine: Toviaz (4/8mg) ERTUSSENIN")
70
“Er is geen enkel middel dat “beter” is”.
Anticholinergica “Er is geen enkel middel dat “beter” is”. Er zijn individuele verschillen in effectiviteit Middelen hebben een verschillend profiel mbt bijwerkingen Mogelijk ook verschil in de veiligheid Bij bepaalde patienten kunnen deze verschillen klinisch relevant zijn

71
Fesoterodine / Tolteridine
Note to speaker: This slide is a build. Fesoterodine is a new once-daily antimuscarinic for the treatment of overactive bladder. Fesoterodine and tolterodine are related, since both are converted to the same active metabolite, albeit via different pathways. In contrast to tolterodine ER, which has 1 dose, 2 dose levels of fesoterodine (4 mg and 8 mg) were developed and evaluated in 2 separate Phase 3 studies. [Tolterodine ER is also approved at a 2 mg once-daily dose for use in patients with impaired hepatic or renal function.] [According to the US PI, the 2 mg dose of tolterodine ER is also recommended for use in patients who are currently taking drugs that are potent inhibitors of CYP3A4.] [According to the SmPC, tolterodine ER should be avoided in patients taking potent CYP3A4 inhibitors. Full dosing recommendations can be found in the regulatory labels.] References Chapple C, Van Kerrebroeck P, Tubaro A, et al. Clinical efficacy, safety, and tolerability of once-daily fesoterodine in subjects with overactive bladder. Eur Urol. 2007;52: Detrol® LA (tolterodine tartrate) extended release capsules [prescribing information]. New York, NY: Pfizer Inc.; March 2008. Toviaz® prolonged-release tablets SmPC; 2008. fesoteridine 5- hydroxymethyl tolterodine 71 71 71
 were developed and evaluated in 2 separate Phase 3 studies. [Tolterodine ER is also approved at a 2 mg once-daily dose for use in patients with impaired hepatic or renal function.] [According to the US PI, the 2 mg dose of tolterodine ER is also recommended for use in patients who are currently taking drugs that are potent inhibitors of CYP3A4.] [According to the SmPC, tolterodine ER should be avoided in patients taking potent CYP3A4 inhibitors. Full dosing recommendations can be found in the regulatory labels.] References. Chapple C, Van Kerrebroeck P, Tubaro A, et al. Clinical efficacy, safety, and tolerability of once-daily fesoterodine in subjects with overactive bladder. Eur Urol. 2007;52: Detrol® LA (tolterodine tartrate) extended release capsules [prescribing information]. New York, NY: Pfizer Inc.; March Toviaz® prolonged-release tablets SmPC; fesoteridine. 5- hydroxymethyl tolterodine")
72
Voordelen van Esterasen
Esterasen zijn overal aanwezig en niet-specifiek in bloed, interstitiële ruimtes, dundarm, long, etc. Er zijn geen gekende Inter-individuele verschillen in esterase activiteit die genetisch bepaald zouden zijn Drug interacties gerelateerd aan esterase activiteit Esterases are abundant and ubiquitous, present throughout the body Importantly, they are consistent among individuals (based on genetics), and their activity is not affected by other drugs, eliminating the two main sources of variability in exposure to the drug among different patients. Fesoterodine was selected among other esters of 5-HMT because it possessed the best release/permeation properties and delivered the best PK profile of 5-HMT after hydrolysis by esterases. References: Dorland’s Pocket Medical Dictionary. 24th ed. Philadelphia: WB Saunders, 1989. Beers R, Camporesi E. CNS Drugs 2004;18: Imai T. Drug Metab Pharmacokinet 2006;21: Dorland’s Pocket Medical Dictionary. 24th ed. Philadelphia: WB Saunders, Beers R, Camporesi E. CNS Drugs 2004;18: Imai T. Drug Metab Pharmacokinet 2006;21: PK = pharmacokinetics. 72
, and their activity is not affected by other drugs, eliminating the two main sources of variability in exposure to the drug among different patients. Fesoterodine was selected among other esters of 5-HMT because it possessed the best release/permeation properties and delivered the best PK profile of 5-HMT after hydrolysis by esterases. References: Dorland’s Pocket Medical Dictionary. 24th ed. Philadelphia: WB Saunders, Beers R, Camporesi E. CNS Drugs 2004;18: Imai T. Drug Metab Pharmacokinet 2006;21: Dorland’s Pocket Medical Dictionary. 24th ed. Philadelphia: WB Saunders, Beers R, Camporesi E. CNS Drugs 2004;18: Imai T. Drug Metab Pharmacokinet 2006;21: PK = pharmacokinetics. 72.")
73
Fesoterodine Conversie naar 5-HMT Is Simpel en Voorspelbaar
Esterases 5-HMT Fesoterodine Ubiquitous Tolterodine Metabolisme Is Complexer en Minder Voorspelbaar Tolt Tolt Tolt + + CYP2D6 The conversion of fesoterodine to its active metabolite, 5-HMT, is simple and predictable: it is rapid and extensive and is mediated by ubiquitous esterases. The metabolism of tolterodine is more complex: it undergoes oxidation via CYP2D6 primarily in the liver, and the efficiency with which individuals perform this oxidation varies across the population. Overall, CYP2D6 metaboliser status can be broken down into extensive, intermediate, and poor metabolisers (EMs, IMs, and PMs). EMs (~78% to 83% of the population) oxidise tolterodine efficiently, metabolising approximately half of it into 5-HMT. IMs are less efficient, resulting in a smaller proportion of 5-HMT. In PMs (~2% to 7% of the population), who are devoid of CYP2D6, no 5-HMT is formed at all. It is this variability in metabolic status, as well as variability arising from drug interactions, that leads to variable ratios of tolterodine and 5-HMT in different patients. Area of EM circles = 3.14 mm radius each = 6.28 mm total area. Area of IM circles = 4.52 mm radius and 1.76 mm radius = 6.28 mm total area. Area of PM circle = mm radius = 6.28 mm total area. References Sachse R, Cawello W, Haag C, Horstmann R. Dose-proportional pharmacokinetics of the new antimuscarinic fesoterodine. Naunyn-Schmiedebergs Arch Pharmacol. 2003;367(suppl 1):446. Brynne N, Dalen P, Alvan G, Bertilsson L, Gabrielsson J. Influence of CYP2D6 polymorphism on the pharmacokinetics and pharmacodynamic of tolterodine. Clin Pharmacol Ther. 1998;63: Zanger UM et al. Cytochrome P450 2D6: overview and update on pharmacology, genetics, biochemistry. Naunyn-Schmiedebergs Arch Pharmacol. 2004;369:23-27. Bradford LD, Kirlin WG. Polymorphism of CYP2D6 in black populations: implications for psychopharmacology. Int J Neuropsychopharmacol. 1998;1: Tolterodine 5-HMT Liver, Gut 5-HMT Extensive Metabolisers 78% Intermediate Metabolisers Poor Metabolisers 7% Prevalence of extensive and poor metabolisers in white European populations. PK = pharmacokinetics; Tolt = tolterodine. Sachse R et al. Naunyn-Schmiedebergs Arch Pharmacol. 2003;367(suppl 1):446. Brynne N et al. Clin Pharmacol Ther. 1998;63: Zanger UM et al. Naunyn-Schmiedebergs Arch Pharmacol. 2004;369:23-27. Bradford LD et al. Int J Neuropsychopharmacol. 1998;1: 73 73 73
. EMs (~78% to 83% of the population) oxidise tolterodine efficiently, metabolising approximately half of it into 5-HMT. IMs are less efficient, resulting in a smaller proportion of 5-HMT. In PMs (~2% to 7% of the population), who are devoid of CYP2D6, no 5-HMT is formed at all. It is this variability in metabolic status, as well as variability arising from drug interactions, that leads to variable ratios of tolterodine and 5-HMT in different patients. Area of EM circles = 3.14 mm radius each = 6.28 mm total area. Area of IM circles = 4.52 mm radius and 1.76 mm radius = 6.28 mm total area. Area of PM circle = mm radius = 6.28 mm total area. References. Sachse R, Cawello W, Haag C, Horstmann R. Dose-proportional pharmacokinetics of the new antimuscarinic fesoterodine. Naunyn-Schmiedebergs Arch Pharmacol. 2003;367(suppl 1):446. Brynne N, Dalen P, Alvan G, Bertilsson L, Gabrielsson J. Influence of CYP2D6 polymorphism on the pharmacokinetics and pharmacodynamic of tolterodine. Clin Pharmacol Ther. 1998;63: Zanger UM et al. Cytochrome P450 2D6: overview and update on pharmacology, genetics, biochemistry. Naunyn-Schmiedebergs Arch Pharmacol. 2004;369: Bradford LD, Kirlin WG. Polymorphism of CYP2D6 in black populations: implications for psychopharmacology. Int J Neuropsychopharmacol. 1998;1: Tolterodine. 5-HMT. Liver, Gut. 5-HMT. Extensive Metabolisers. 78% Intermediate. Metabolisers. Poor Metabolisers. 7% Prevalence of extensive and poor metabolisers in white European populations. PK = pharmacokinetics; Tolt = tolterodine. Sachse R et al. Naunyn-Schmiedebergs Arch Pharmacol. 2003;367(suppl 1):446. Brynne N et al. Clin Pharmacol Ther. 1998;63: Zanger UM et al. Naunyn-Schmiedebergs Arch Pharmacol. 2004;369: Bradford LD et al. Int J Neuropsychopharmacol. 1998;1:")
74
5-HMT Is Minder Lipofiel dan Tolterodine
Lipophilicity is an important predictor of the ability of a drug to cross the blood-brain barrier 5-HMT tolterodine solifenacin oxybutynin trospium -2 -1 1 2 3 4 logD (octanol/water ratio) darifenacin* A smaller logD indicates less lipophilicity. The clinical relevance of these findings is unknown; however, for the triptan class of antimigraine drugs, a correlation was found between reduced lipophilicity and lower CNS adverse event rates. As you will see later, the incidence of CNS adverse events in fesoterodine clinical trials was similar to placebo. CNS adverse effects are particularly relevant in elderly patients who may be taking various concomitant medications. The logD value for darifenacin was not obtained in the same study as the other agents. NOTE TO SPEAKER: THE INFORMATION BELOW SHOULD ONLY BE ADDRESSED IF A QUESTION IS ASKED ABOUT DARIFENACIN [There is a general understanding that darifenacin does not penetrate CNS as no effects on cognitive function have been observed. Showing a high logD value of darifenacin may raise questions, at which point a discussion of P-glycoprotein (PgP) transport and selectivity would be necessary.] Reference Malhotra B, Wood N, Sachse R, Gandelman K. Lipophilicity of 5-hydroxymethyl tolterodine, the active metabolite of fesoterodine. Poster presented at Winter Meeting of the British Pharmacological Society; December 17–20, 2007; Brighton, UK. Chapple C. Darifenacin, A Novel M3 Muscarinic Selective Receptor Antagonist for the Treatment of Overactive Bladder. Expert Opin Investig Drugs. 2004;13: *Darifenacin was not included in the same study as the other agents. The lipophilicity was obtained from a separate trial done on darifenacin alone. Malhotra B et al. Presented at Br Pharmacol Soc Winter Meeting Chapple C. Expert Opin Investig Drugs. 2004;13: 74 74 74
 darifenacin* A smaller logD indicates less lipophilicity. The clinical relevance of these findings is unknown; however, for the triptan class of antimigraine drugs, a correlation was found between reduced lipophilicity and lower CNS adverse event rates. As you will see later, the incidence of CNS adverse events in fesoterodine clinical trials was similar to placebo. CNS adverse effects are particularly relevant in elderly patients who may be taking various concomitant medications. The logD value for darifenacin was not obtained in the same study as the other agents. NOTE TO SPEAKER: THE INFORMATION BELOW SHOULD ONLY BE ADDRESSED IF A QUESTION IS ASKED ABOUT DARIFENACIN. [There is a general understanding that darifenacin does not penetrate CNS as no effects on cognitive function have been observed. Showing a high logD value of darifenacin may raise questions, at which point a discussion of P-glycoprotein (PgP) transport and selectivity would be necessary.] Reference. Malhotra B, Wood N, Sachse R, Gandelman K. Lipophilicity of 5-hydroxymethyl tolterodine, the active metabolite of fesoterodine. Poster presented at Winter Meeting of the British Pharmacological Society; December 17–20, 2007; Brighton, UK. Chapple C. Darifenacin, A Novel M3 Muscarinic Selective Receptor Antagonist for the Treatment of Overactive Bladder. Expert Opin Investig Drugs. 2004;13: *Darifenacin was not included in the same study as the other agents. The lipophilicity was obtained from a separate trial done on darifenacin alone. Malhotra B et al. Presented at Br Pharmacol Soc Winter Meeting Chapple C. Expert Opin Investig Drugs. 2004;13:")
75
Behandeling met Fesoterodine reduceert de Plasfrequentie
Trial SP584: Percent Change in Number of Micturitions per 24 Hours at Week 12 Median % Change from Baseline in Number of Micturitions/24 h * Placebo N=266 Feso 4 mg N=267 Feso 8 mg BL=12.2 BL=12.9 BL=12.0 In this study, treatment with either dose of fesoterodine produced statistically significant reductions from baseline in the number of micturitions per 24 hours, compared with placebo. Average baseline values were similar across groups (12.2, 12.9, and 12.0 for placebo, 4 mg fesoterodine, and 8 mg fesoterodine, respectively). The median percent reduction in number of micturitions per 24 hours from baseline to end of treatment (last observation carried forward [LOCF]) was 14.9% in the 4-mg group, and 16.0% in the 8-mg group, compared to 6.9% for subjects in the placebo group (P<0.001 for either dose vs. placebo). Additional analysis did not reveal significant differences between the two active treatments. References: Nitti VW et al. J Urol 2007;178: Data on file. Pfizer Inc. * P<0.001 vs. placebo. BL = mean at baseline. Nitti VW et al. J Urol 2007;178: 75
. The median percent reduction in number of micturitions per 24 hours from baseline to end of treatment (last observation carried forward [LOCF]) was 14.9% in the 4-mg group, and 16.0% in the 8-mg group, compared to 6.9% for subjects in the placebo group (P<0.001 for either dose vs. placebo). Additional analysis did not reveal significant differences between the two active treatments. References: Nitti VW et al. J Urol 2007;178: Data on file. Pfizer Inc. * P<0.001 vs. placebo. BL = mean at baseline. Nitti VW et al. J Urol 2007;178:")
76
Behandeling met Fesoteridine reduceert de Urge/Urge-incontinentie
Trial SP584: Percent Change in Number of UUI Episodes per 24 Hours at Week 12 Placebo N=205 Feso 4 mg N=228 Feso 8 mg N=218 Median % Change from Baseline in UUI episodes per 24h * † BL=3.9 BL=3.7 P=0.018 In this study, treatment with either 4 mg or 8 mg of fesoterodine produced statistically significant reductions from baseline in the number of UUI episodes per 24 hours, compared with placebo. Average baseline values were similar across groups (3.7, 3.9, and 3.9 for placebo, 4 mg fesoterodine, and 8 mg fesoterodine, respectively). The analysis included only subjects with 1 or more UUI episodes at baseline. The median percent reduction in number of UUI episodes per 24 hours from baseline to end of treatment (last observation carried forward [LOCF]) was 67% on 4 mg of fesoterodine and 82% on 8 mg, compared with 40% in the placebo group (P<0.001 for either dose vs. placebo). In an additional analysis, the difference between 8 mg fesoterodine and 4 mg fesoterodine on this endpoint was shown to be statistically significant (P=0.018), indicating a dose-response relationship on this important OAB endpoint. References: Data on file. Pfizer Inc. Nitti VW et al. J Urol 2007;178: Analysis includes only subjects with UUI at baseline. * P<0.001 vs. placebo. † P=0.018 vs. feso 4 mg (additional analysis). BL = mean at baseline; UUI = urgency urinary incontinence. Nitti VW et al. J Urol 2007;178: Data on file. Pfizer Inc. 76
. The analysis included only subjects with 1 or more UUI episodes at baseline. The median percent reduction in number of UUI episodes per 24 hours from baseline to end of treatment (last observation carried forward [LOCF]) was 67% on 4 mg of fesoterodine and 82% on 8 mg, compared with 40% in the placebo group (P<0.001 for either dose vs. placebo). In an additional analysis, the difference between 8 mg fesoterodine and 4 mg fesoterodine on this endpoint was shown to be statistically significant (P=0.018), indicating a dose-response relationship on this important OAB endpoint. References: Data on file. Pfizer Inc. Nitti VW et al. J Urol 2007;178: Analysis includes only subjects with UUI at baseline. * P<0.001 vs. placebo. † P=0.018 vs. feso 4 mg (additional analysis). BL = mean at baseline; UUI = urgency urinary incontinence. Nitti VW et al. J Urol 2007;178: Data on file. Pfizer Inc. 76.")
77
Fesoterodine tolerantie
The safety of fesoterodine was evaluated in placebo-controlled clinical studies in a total of 2859 patients with overactive bladder, of which 780 received placebo(11) The safety profile of fesoterodine is the one expected for an antimuscarinic drug(16) Dry mouth, the only very common event, occurred with a frequency of 28.8% in the fesoterodine group compared to 8.5% in the placebo group(11) References 11. TOVIAZ® Summary of Product Characteristics 16. TOVIAZ® EMEA Scientific discussion 25. Khullar V, Rovner E, Dmochowski R, Nitti V, Wang J, Guan Z. Fesoterodine dose response in subjects with overactive bladder syndrome. In press. Vergeleken met andere antimuscarine stoffen, was de incidentie van constipatie bij fesoterodine relatief laag(25) (11) Summary of Product Characteristics. (16) EMEA Scientific discussion. (25) Khullar V et al 77 77 77
 The safety profile of fesoterodine is the one expected for an antimuscarinic drug(16) Dry mouth, the only very common event, occurred with a frequency of 28.8% in the fesoterodine group compared to 8.5% in the placebo group(11) References. 11. TOVIAZ® Summary of Product Characteristics. 16. TOVIAZ® EMEA Scientific discussion. 25. Khullar V, Rovner E, Dmochowski R, Nitti V, Wang J, Guan Z. Fesoterodine dose response in subjects with overactive bladder syndrome. In press. Vergeleken met andere antimuscarine stoffen, was de incidentie van constipatie bij fesoterodine. relatief laag(25) (11) Summary of Product Characteristics. (16) EMEA Scientific discussion. (25) Khullar V et al")
78
R/ - Key messages 1st line physicians are in the right position to diagnose and treat OAB Patients may not initiate discussion about OAB Physicians can elicit information through appropriate questions An integrated treatment approach should be emphasized Behavioral therapy Physiotherapy Pharmacotherapy Once identified and diagnosed, most patients can be effectively treated for their symptoms of OAB. Physicians should also emphasize to patients the importance of an integrated treatment approach that includes pharmacotherapy in addition to behavioral therapy, including fluid management and physiotherapy, such as pelvic floor exercises. Antimuscarinic agents are the gold standard of OAB pharmacotherapy, the goal of which is to maximize the efficacy of treatment as well as tolerability and improved Quality of Life. Agents, such as Detrusitol® SR, that have balanced M2 and M3 muscarinic-receptor affinity, offer physicians the best combination of efficacy, tolerability, and improved patient outcomes. Chapple C.R.. Pocket Reference to Overactive Bladder, Current Medicine Group 2007

79
R/ - Key messages (2) The goal of OAB pharmacotherapy is to maximize efficacy, tolerability, and patients’ Quality of Life Antimuscarinic agents are the first-line pharmaco-therapies for OAB, based on the pathophysiology of the syndrome i.e., the presence of a parasympathetic muscarinic component of the common pathway for normal voiding as well as an involuntary bladder contraction Once identified and diagnosed, most patients can be effectively treated for their symptoms of OAB. Physicians should also emphasize to patients the importance of an integrated treatment approach that includes pharmacotherapy in addition to behavioral therapy, including fluid management and physiotherapy, such as pelvic floor exercises. Antimuscarinic agents are the gold standard of OAB pharmacotherapy, the goal of which is to maximize the efficacy of treatment as well as tolerability and improved Quality of Life. Agents, such as Detrusitol® SR, that have balanced M2 and M3 muscarinic-receptor affinity, offer physicians the best combination of efficacy, tolerability, and improved patient outcomes. Chapple C.R.. Pocket Reference to Overactive Bladder, Current Medicine Group 2007

80
R/ - Key messages (3) Evaluate progress of therapy Voiding diary
Patient perception Rate bladder problems (none, very minor, minor, moderate, severe, many severe) Rate ability to finish tasks without leaking (usually, if go immediately afterward, usually not) Reduction in symptoms so patients can get back to doing things they used to do OAB treatment is effective in the majority of patients Once identified and diagnosed, most patients can be effectively treated for their symptoms of OAB. Physicians should also emphasize to patients the importance of an integrated treatment approach that includes pharmacotherapy in addition to behavioral therapy, including fluid management and physiotherapy, such as pelvic floor exercises. Antimuscarinic agents are the gold standard of OAB pharmacotherapy, the goal of which is to maximize the efficacy of treatment as well as tolerability and improved Quality of Life. Agents, such as Detrusitol® SR, that have balanced M2 and M3 muscarinic-receptor affinity, offer physicians the best combination of efficacy, tolerability, and improved patient outcomes. Chapple C.R.. Pocket Reference to Overactive Bladder, Current Medicine Group 2007
 Rate ability to finish tasks without leaking (usually, if go immediately afterward, usually not) Reduction in symptoms so patients can get back to doing things they used to do. OAB treatment is effective in the majority of patients. Once identified and diagnosed, most patients can be effectively treated for their symptoms of OAB. Physicians should also emphasize to patients the importance of an integrated treatment approach that includes pharmacotherapy in addition to behavioral therapy, including fluid management and physiotherapy, such as pelvic floor exercises. Antimuscarinic agents are the gold standard of OAB pharmacotherapy, the goal of which is to maximize the efficacy of treatment as well as tolerability and improved Quality of Life. Agents, such as Detrusitol® SR, that have balanced M2 and M3 muscarinic-receptor affinity, offer physicians the best combination of efficacy, tolerability, and improved patient outcomes. Chapple C.R.. Pocket Reference to Overactive Bladder, Current Medicine Group")
Verwante presentaties



>")





![Deltion College Engels C1 Gesprekken voeren [Edu/002]/ subvaardigheid lezen thema: Order, order…. can-do : kan een bijeenkomst voorzitten © Anne Beeker.](/8/2048322/big_thumb.jpg "Deltion College Engels C1 Gesprekken voeren [Edu/002]/ subvaardigheid lezen thema: Order, order…. can-do : kan een bijeenkomst voorzitten © Anne Beeker.>")










