Download de presentatie
De presentatie wordt gedownload. Even geduld aub

1
CVA 2008 Een Update Voor De Huisarts
Vincent Thijs Dienst Neurologie Stroke Unit UZ Gasthuisberg, Leuven

2
Een Update Voor De Huisarts
Primaire preventie van CVA Asymptomatische carotisstenose Voorkamerfibrillatie Secundaire preventie van CVA Behandeling van TIA en CVA

3
Risicofactoren Behandelbaar Niet behandelbaar Roken Leeftijd
Arteriële hypertensie Diabetes Hypercholesterolemie hsCRP Te weinig lichaamsbeweging Voorkamerfibrillatie Carotisstenose TIA Niet behandelbaar Leeftijd Geslacht Familiale voorgeschiedenis Diabetes

4
Primaire PREVENTIE

5
Hypertensie Verantwoordelijk voor tot 50% van alle CVA
Streefwaarde <140mmHg s en <90 mmHg d Ook systolisch Reductie eerste en tweede CVA tot 40% > AMI

6
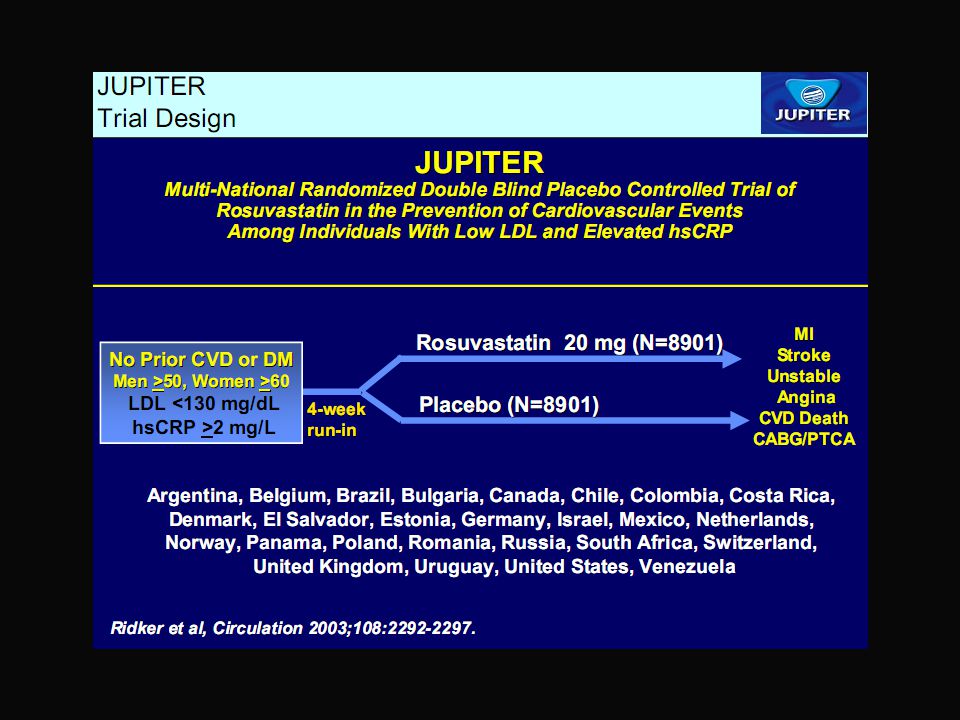
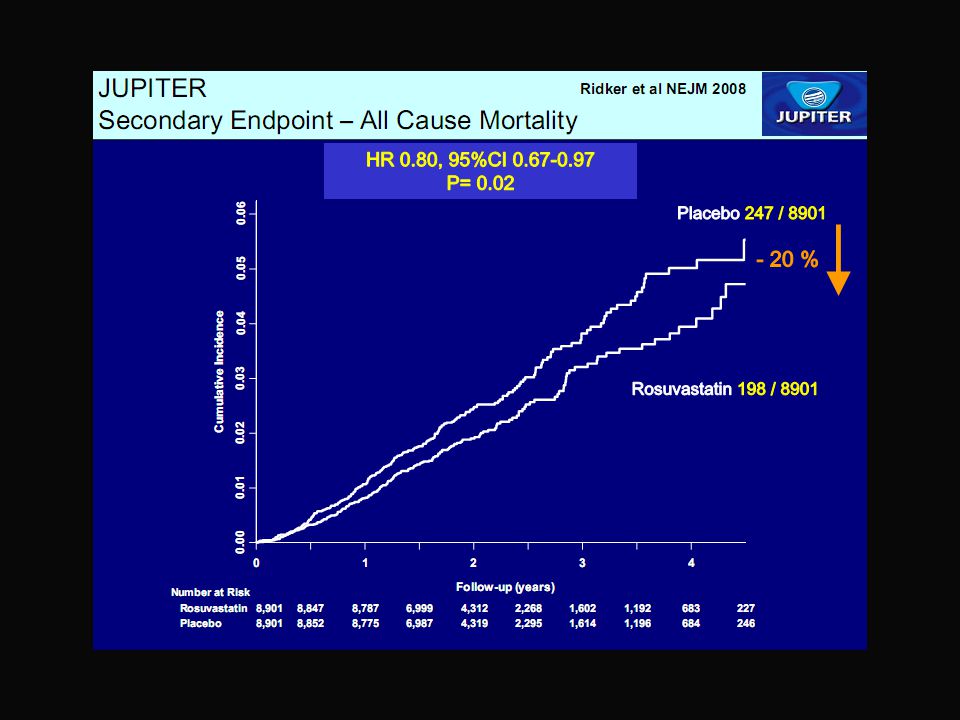
Beschermt cholesterolverlaging tegen CVA?
Bewezen bij AMI Diabetes Multipele risicofactoren hsCRP

7
Cholesterolverlaging

14
Patient 1 75 year old woman DM type II Arterial Hypertension Cholesterol 193 mg/dl Carotid duplex performed because of dizziness Left sided carotid stenosis of 80-99% Reversed flow in ophtalmic artery

15
Therapeutic options A. Conservative management B. Carotid surgery + A
Control of DM Control of HT <130/80 mmHg Statin treatment Aspirin B. Carotid surgery + A C. Carotid stenting + A

16
Asymptomatic Carotid Stenosis
ACST, Lancet 2004

17
10 year FU in ACST ? 6 7 8 9 10

18
Asymptomatische Carotisstenose Ingrijpen, Maar Niet Chirurgisch
Lange termijn risico laag op recidief (2% per jaar) Oorzaak van recidief in 50% niet toe te schrijven aan carotisstenose Hoog risico op AMI in toekomst Operatie enkel in geselecteerde gevallen en bij chirurg met veel ervaring Niet boven 75 jaar Minder duidelijk effect bij vrouwen
 Oorzaak van recidief in 50% niet toe te schrijven aan carotisstenose. Hoog risico op AMI in toekomst. Operatie enkel in geselecteerde gevallen en bij chirurg met veel ervaring. Niet boven 75 jaar. Minder duidelijk effect bij vrouwen.")
19
Case history 65 year old patient with acute onset of weakness in left leg and confusion Smoker, controlled hypertension and diabetes Intermittent atrial fibrillation since 6 months Medication: β-blocker, aspirin, ACE-inhibitor

20
Doeltreffendheid van orale anticoagulatie versus controle
68% RRR No. of Events Patient- years Risk Reduction, % AFASAK BAATAF CAFA SPAF SPINAF Combined A stroke risk reduction of 69% attributable to warfarin was seen when the data from five studies were combined in the pooled analysis. All analyses represented for individual studies are done on an “intention-to-treat” basis. Note: Strokes represent all strokes regardless of suspected etiology. Transient ischemic attacks, systemic emboli and intracranial hemorrhages are not included. Control represents placebo in all studies except BAATAF where 46% of “control” patients received aspirin and 54% received no treatment.20 Warfarin Better Warfarin Worse Arch Int Med 1994;154:1449–1457

21
Doeltreffendheid van aspirine versus controle
21% RRR No. of Events Patient- years Risk Reduction (%) AFASAK SPAF EAFT Combined* The results of the three AF trials that directly compared aspirin to placebo are summarized. Although the AF trials all have wide confidence intervals, in aggregate they suggest an approximately 20% to 25% stroke risk reduction attributable to aspirin with no clear relationship to aspirin dose.22,23,27,30,31 Aspirin Better Aspirin Worse *Total risk reduction for all 3 studies combined is 21% Arch Int Med 1994;154:1449–1457
 AFASAK SPAF EAFT Combined* The results of the three AF trials that directly compared aspirin to placebo are summarized. Although the AF trials all have wide confidence intervals, in aggregate they suggest an approximately 20% to 25% stroke risk reduction attributable to aspirin with no clear relationship to aspirin dose.22,23,27,30, Aspirin Better. Aspirin Worse. *Total risk reduction for all 3 studies combined is 21% Arch Int Med 1994;154:1449–1457.")
22
Majeure Bloedingen Per jaar
Patienten met placebo of aspirine: 1.0% Patienten onder orale anticoagulatie: 1.3% Aspirine-behandelde patienten: 1.0% Major Bleeding: A bleeding episode is usually classified as major if meets at least one of the following criteria: • intracranial or retroperitoneal • led directly to death • resulted in hospitalization or transfusion Arch Int Med 1994;154:1453–1454

23
Optimale Intensiteit van ontstolling
15 INR Odds Ratio 10 Odds Ratio for Stroke 5 3 1 Recently, Hylek et al, evaluated the efficacy of different intensities of anticoagulation in a case-control study. They found that an intensity of anticoagulation below an INR of 2.0 was associated with a higher risk of stroke. 1.0 1.5 2.0 3.0 4.0 7.0 INR Hylek EM, et al. NEJM 1996;335:

24
Risico op Intracraniele Bloeding
11.2 18.2 10 8 6 Odds Ratio for ICH 4 2 Hylek, et al, studied the risk of intracranial hemorrhage in outpatients treated with warfarin. They determined that an intensity of anticoagulation expressed as a prothrombin time ratio (PTR) above 2.0* resulted in an increase in the risk of bleeding. * roughly corresponding to an INR of 3.7 to 4.3 1.4 1.6 1.8 2 2.3 2.7 Prothrombin Time Ratio Hylek EM, Singer DE. Ann Int Med 1994;120:
 above 2.0* resulted in an increase in the risk of bleeding. * roughly corresponding to an INR of 3.7 to Prothrombin Time Ratio. Hylek EM, Singer DE. Ann Int Med 1994;120:")
25
Aanbevolen grenzen voor ontstolling bij VKF
Doel: INR 2.5 Range: INR 2.0–3.0 Slide 13 The Fifth American College of Chest Physicians (ACCP) Consensus Conference on Antithrombotic Therapy recommended that an INR of 2.0 to 3.0 be used in patients with atrial fibrillation for the prevention of thromboembolic complications (including stroke). The Consensus Panel also recommended a target INR of 2.5. This is largely due to the data from numerous clinical trials, including the pooled analysis, and recent case-control studies showing the adverse consequences of exceeding or failing to achieve a therapeutic intensity of anticoagulation. Note: this slide replaces slide 51 in the program dated August 1997. CHEST 1998;114:579s-589s
 Consensus Conference on Antithrombotic Therapy recommended that an INR of 2.0 to 3.0 be used in patients with atrial fibrillation for the prevention of thromboembolic complications (including stroke). The Consensus Panel also recommended a target INR of 2.5. This is largely due to the data from numerous clinical trials, including the pooled analysis, and recent case-control studies showing the adverse consequences of exceeding or failing to achieve a therapeutic intensity of anticoagulation. Note: this slide replaces slide 51 in the program dated August CHEST 1998;114:579s-589s.")
26
Relationship Between CHADS2 Score and Annual Risk of Stroke
CHADS2 Stroke Risk Stratification Scheme for Patients With Nonvalvular AF CHADS2 Score Relationship Between CHADS2 Score and Annual Risk of Stroke Risk factors Score C Recent congestive heart failure 1 H Hypertension A Age ≥75 yrs D Diabetes mellitus S2 History of stroke/TIA 2 Stroke Rate (%) Based on study patients treated with aspirin c-statistic of 0.63 of CHADS score if stroke patients were removed C-statistic of 0.5 is coin toss C-statistic of 1 is perfect C-statistic of 0.6 has limited value CHADS2 Score Adapted from Hersi A and Wyse DG Curr Probl Cardiol;30:175–234.
 Based on study patients treated with aspirin. c-statistic of 0.63 of CHADS score if stroke patients were removed. C-statistic of 0.5 is coin toss. C-statistic of 1 is perfect. C-statistic of 0.6 has limited value. CHADS2 Score. Adapted from Hersi A and Wyse DG Curr Probl Cardiol;30:175–234.")
27
ACCP 2008 richtlijn OAC als 2 of meer risicofactoren
>75 VG van hypertensie DM Gestoorde LV functie of hartsdecompensatie OAC als 2 of meer risicofactoren 1 risico factor OAC > ASA 0 risico factor ASA CHADS score of 2 OAC CHADS score of 1 doubtful CHADS score of 0 aspirin

28
Paroxysmale/intermittente VKF
Zelfde indicaties voor OAC als persistente VKF OAC beter dan ASA Terug sinusaal + risicofactoren: blijven OAC geven !!!!!

29
Secundaire pREVENTIE

30
Hoe Kiezen Voor Het Beste Antitromboticum Na Een ischemisch CVA?

31
Secundaire Preventie met Plaatjesremmers
Kost en terugbetaling, nevenwerkingen, effectiviteit, voorgeschiedenis (?) Opties Aspirine <100 mg /dag ASA en DP (Aggrenox) Clopidogrel (Plavix) Ticlopidine (Ticlid) Oraal anticoagulans
 Opties. Aspirine <100 mg /dag. ASA en DP (Aggrenox) Clopidogrel (Plavix) Ticlopidine (Ticlid) Oraal anticoagulans.")
33
Aspirine <100 mg/dag Goedkoop
Effectiviteit versus placebo bewezen in multipele studies en bewezen effect bij AMI, vasculaire dood en CVA Nevenwerkingen aanvaardbaar in lage dosis Effect op recidief CVA RRR 13% (7% controle-6% ASA, NNT 100)
")
34
Ticlopidine (Ticlid) Duur Effectiviteit bewezen
Onaanvaardbare nevenwerkingen Krachtiger dan ASA (en clopidogrel?)
")
35
Clopidogrel (Plavix) Effectiviteit in 1 studie (CAPRIE) aangetoond
Veilig RRR in CVA patienten versus ASA 7.3% RRR in alle patienten versus ASA 8.7%

36
8.7%* Overall relative risk reduction (RRR)
CAPRIE (Myocardial Infarction, Ischaemic Stroke or Vascular Death) Aspirin 16 8.7%* Overall relative risk reduction (RRR) P = n = 19,185 12 Clopidogrel Cumulative event rate (%) 8 4 3 6 9 12 15 18 21 24 27 30 33 36 Months of follow-up * ITT analysis CAPRIE Steering Committee. Lancet 1996; 348 (9038): 1329–1339.
 Aspirin %* Overall relative risk reduction (RRR) P = n = 19, Clopidogrel. Cumulative event rate (%) Months of follow-up. * ITT analysis. CAPRIE Steering Committee. Lancet 1996; 348 (9038): 1329–1339.")
37
Aspirine + ER Dipyridamole
Effectiviteit in 1 grote studie (ESPS 2) aangetoond Veilig (hoofdpijn) RRR in CVA patiënten versus ASA 23% NNT 33
 aangetoond. Veilig (hoofdpijn) RRR in CVA patiënten versus ASA 23% NNT 33.")
38
ESPS 2: Efficacy of ER-DP + ASA
(n=3,299) ASA ER-DP + ASA Total # of events (2 yr follow-up) The results of ESPS 2 clearly show that the combination treatment of ER-DP + ASA is significantly superior to ASA alone (RRR 23%, p < 0.006) in the prevention of second stroke. Stroke MI 23% RRR* 13% RRR 49 events prevented 4 events prevented *Statistically significant Diener HC et al. J Neurol Sci. 1996; 143: 1-13.
 ASA. ER-DP + ASA. Total # of events (2 yr follow-up) The results of ESPS 2 clearly show that the combination treatment of ER-DP + ASA is significantly superior to ASA alone (RRR 23%, p < 0.006) in the prevention of second stroke. Stroke. MI. 23% RRR* 13% RRR. 49 events prevented 4 events prevented. *Statistically significant. Diener HC et al. J Neurol Sci. 1996; 143:")
39
® – trial design ER-DP + ASA (400 mg/50 mg) Clopidogrel* (75 mg)
2x2 factorial design involving 20,332 stroke patients ER-DP + ASA (400 mg/50 mg) Clopidogrel* (75 mg) ER-DP + ASA + Telmisartan (5,000 pts) Clopidogrel* + Telmisartan (5,000 pts) Telmisartan (80 mg) ER-DP + ASA + Placebo (5,000 pts) Clopidogrel + Placebo (5,000 pts) Patients participating in the trial were randomised, in double-blind fashion, to one of four treatment groups: ER-DP + ASA (25 mg/200 mg) bid; clopidogrel placebo qd; telmisartan (80 mg) qd Clopidogrel (75 mg) qd; ER-DP + ASA placebo bid; telmisartan (80 mg) qd telmisartan placebo qd Each treatment group will have 5,000 randomised patients assigned to it. Assuming no interaction between any of the combinations of treatments in the factorial design, the study is also capable of detecting a 25% stroke hazard reduction on telmisartan vs. placebo with >99% power at the 5% two-sided significance level. A 25% hazard reduction was observed in the LIFE trial for losartan compared to atenolol in hypertensive patients with LVH. In fact, to detect a 25% stroke hazard reduction on telmisartan vs. placebo with 90% power at the 5% two-sided significance level, only 4,000 patients (and 510 strokes) are required. Placebo Diener, Sacco, Yusuf. Cerebrovasc Dis 2007; 23: 368–380. 39 39 39
 Clopidogrel* (75 mg) ER-DP + ASA. + Telmisartan. (5,000 pts) Clopidogrel* + Telmisartan. (5,000 pts) Telmisartan. (80 mg) ER-DP + ASA. + Placebo. (5,000 pts) Clopidogrel. + Placebo. (5,000 pts) Patients participating in the trial were randomised, in double-blind fashion, to one of four treatment groups: ER-DP + ASA (25 mg/200 mg) bid; clopidogrel placebo qd; telmisartan (80 mg) qd. Clopidogrel (75 mg) qd; ER-DP + ASA placebo bid; telmisartan (80 mg) qd. telmisartan placebo qd. Each treatment group will have 5,000 randomised patients assigned to it. Assuming no interaction between any of the combinations of treatments in the factorial design, the study is also capable of detecting a 25% stroke hazard reduction on telmisartan vs. placebo with >99% power at the 5% two-sided significance level. A 25% hazard reduction was observed in the LIFE trial for losartan compared to atenolol in hypertensive patients with LVH. In fact, to detect a 25% stroke hazard reduction on telmisartan vs. placebo with 90% power at the 5% two-sided significance level, only 4,000 patients (and 510 strokes) are required. Placebo. Diener, Sacco, Yusuf. Cerebrovasc Dis 2007; 23: 368–")
40
Secondary Outcome: Stroke, MI, Vascular Death
ASA+ER-DP Clopidogrel HR 95% CI p-value 1333 (13.1%) 0.99 0.92, 1.07 0.829 * Covariates in cox model are age, baseline ACE-inhibitor use, Modified Rankin, and baseline diabetes status.
 , * Covariates in cox model are age, baseline ACE-inhibitor use, Modified Rankin, and baseline diabetes status.")
41
MATCH: Study Design (n=7599)
Aspirin 75 mg qd + Clopidogrel 75 mg qd Aspirin + Clopidogrel (~3800 patients) Recent TIA or IS (within 3 months) AND high risk of recurrent ischemic events* R Placebo + Clopidogrel (~3800 patients) Placebo + Clopidogrel 75 mg qd The Management of Atherothrombosis with Clopidogrel in High-Risk Patients with Recent Transient Ischaemic Attack or Ischaemic Stroke (MATCH) trial is an international, randomized, double-blind, parallel-group study designed to evaluate the benefits of aspirin plus clopidogrel versus placebo plus clopidogrel in high-risk patients with a recent history of transient ischemic attach (TIA) or ischemic stroke (IS). High-risk patients with recent TIA or IS who meet the inclusion/exclusion criteria will be randomized to receive either aspirin 75 mg once daily plus clopidogrel 75 mg once daily or placebo plus clopidogrel 75 mg once daily. The treatment period will continue for 18 months, and each patient will be followed at regular intervals unless the investigator decides to discontinue therapy or the patient withdraws from the study prematurely. The follow-up schedule consists of 6 visits, including the first visit on the day of randomization. After the first visit for randomization, follow-up will be at 1 month, 3 months, 6 months, 12 months, and 18 months. 18-Month Visit End of Study Period† 1-Month Visit 3-Month Visit 6-Month Visit 12-Month Visit Eligibility: Subject must be at high risk of recurrent ischemic events due to: previous IS, previous MI, angina pectoris, symptomatic PAD, or diabetes mellitus Diener H-C et al, on behalf of the MATCH Investigators. Cerebrovasc Dis. 2004;17: Reference Diener H-C, Bogousslavsky J, Brass LM, Cimminiello C, Csiba L, Kaste M et. al, on behalf of the MATCH Investigators. Management of atherothrombosis with clopidogrel in high-risk patients with recent transient ischaemic attack or ischaemic stroke: study design and baseline data. Cerebrovasc Dis. 2004;17:
 Recent. TIA or IS. (within 3 months) AND. high risk of recurrent ischemic events* R. Placebo + Clopidogrel. (~3800 patients) Placebo + Clopidogrel 75 mg qd. The Management of Atherothrombosis with Clopidogrel in High-Risk Patients with Recent Transient Ischaemic Attack or Ischaemic Stroke (MATCH) trial is an international, randomized, double-blind, parallel-group study designed to evaluate the benefits of aspirin plus clopidogrel versus placebo plus clopidogrel in high-risk patients with a recent history of transient ischemic attach (TIA) or ischemic stroke (IS). High-risk patients with recent TIA or IS who meet the inclusion/exclusion criteria will be randomized to receive either aspirin 75 mg once daily plus clopidogrel 75 mg once daily or placebo plus clopidogrel 75 mg once daily. The treatment period will continue for 18 months, and each patient will be followed at regular intervals unless the investigator decides to discontinue therapy or the patient withdraws from the study prematurely. The follow-up schedule consists of 6 visits, including the first visit on the day of randomization. After the first visit for randomization, follow-up will be at 1 month, 3 months, 6 months, 12 months, and 18 months. 18-Month Visit. End of Study Period† 1-Month Visit. 3-Month Visit. 6-Month Visit. 12-Month Visit. Eligibility: Subject must be at high risk of recurrent ischemic events due to: previous IS, previous MI, angina pectoris, symptomatic PAD, or diabetes mellitus. Diener H-C et al, on behalf of the MATCH Investigators. Cerebrovasc Dis. 2004;17: Reference. Diener H-C, Bogousslavsky J, Brass LM, Cimminiello C, Csiba L, Kaste M et. al, on behalf of the MATCH Investigators. Management of atherothrombosis with clopidogrel in high-risk patients with recent transient ischaemic attack or ischaemic stroke: study design and baseline data. Cerebrovasc Dis. 2004;17:")
42
MATCH: Primair Eindpunt
IS, MI, VD, rehospitalization for acute ischemic event 0.20 Placebo + Clopidogrel 0.16 ASA + Clopidogrel RRR: 6.4% (P=.244) 0.12 Cumulative event rate 0.08 NOTE: - Intention-to-treat analysis: RRR: 6.4% (P=.26) - On-treatment analysis: RRR: 9.5% (P=.101) The protocol assumptions were: - Efficacy: RRR = 14% for the primary end point, with 80% power (alpha=0.05, 2-sided) - No safety assumptions 0.04 0.00 3 6 9 12 15 18 Months of follow-up Diener, Lancet 2004 Reference: 1. Diener H-C. Antiplatelet therapy: results of the MATCH trial. Paper presented at: European Stroke Conference; May 13, 2004; Mannheim-Heidelberg, Germany.
 Cumulative event rate NOTE: - Intention-to-treat analysis: RRR: 6.4% (P=.26) - On-treatment analysis: RRR: 9.5% (P=.101) The protocol assumptions were: - Efficacy: RRR = 14% for the primary end point, with 80% power (alpha=0.05, 2-sided) - No safety assumptions Months of follow-up. Diener, Lancet Reference: 1. Diener H-C. Antiplatelet therapy: results of the MATCH trial. Paper presented at: European Stroke Conference; May 13, 2004; Mannheim-Heidelberg, Germany.")
43
% Absolute Difference (95% CI)
MATCH: Majeure Bloedingen Type of Bleeding Events* (%) Placebo + Clopidogrel (n=3781) ASA + Clopidogrel (n=3759) % Absolute Difference (95% CI) P value Defined as life-threatening events (%) 49 (1.3) 96 (2.6) 1.26 (0.64, 1.88) <.001 Gastrointestinal 21 (0.6) 51 (1.4) Intracranial 25 (0.7) 40 (1.1) Major bleeding events (%) 22 (0.6) 73 (1.9) 1.36 (0.86,1.86) <.001 Gastrointestinal 11 (0.3) 42 (1.1)
 Placebo. + Clopidogrel (n=3781) ASA + Clopidogrel. (n=3759) % Absolute Difference (95% CI) P value. Defined as life-threatening events (%) 49 (1.3) 96 (2.6) 1.26 (0.64, 1.88) <.001. Gastrointestinal. 21 (0.6) 51 (1.4) Intracranial. 25 (0.7) 40 (1.1) Major bleeding events (%) 22 (0.6) 73 (1.9) 1.36 (0.86,1.86) <.001. Gastrointestinal. 11 (0.3) 42 (1.1)")
44
CHARISMA: No. at Risk Clopidogrel 7802 7653 7510 7363 5299 2770
7.1% Relative risk reduction (95% CI: -4.5% , 17.5%) 8 Placebo + Aspirin Cumulative Incidence of the Primary Composite End Point (%) 6 Clopidogrel + Aspirin 4 2 6 12 18 24 30 Months No. at Risk Clopidogrel 7802 7653 7510 7363 5299 2770 Placebo 7801 7644 7482 7316 5212 2753 Bhatt et al. N Engl J Med 2006; 354.
 8. Placebo + Aspirin. Cumulative Incidence of the. Primary Composite. End Point (%) 6. Clopidogrel + Aspirin Months. No. at Risk. Clopidogrel Placebo Bhatt et al. N Engl J Med 2006; 354.")
45
Post-stroke statines

46
NNT5 = 46 for stroke 29 for major cardiovascular event 32 for revascularization

47
ACUTE BEHANDELING

48
NIHSS Excellent Recovery (%)
New England Journal, 1995 NINDS tPA Stroke Trial Hemorrhage p < .05 31 20 9 20 8 1 tPA Placebo tPA Placebo NIHSS Excellent Recovery (%) Total Death Rate (%)
 Total Death Rate (%)")
49
Trials of IV tPA: 0-3 Hr Time Window Number showing poor outcome
/ Number at follow up Odds ratio Study t-PA Control 0.1 0.2 1 5 10 Atlantis A / /12 Atlantis B / /26 ECASS / /36 ECASS / /77 NINDS Trial / /147 NINDS Trial / /165 Total / /465 Odds Ratio 0.56 ( ) P= I did the best I could on this one….but I had to “eye” most of it. Favors treatment Favors control Saver, et al Lancet 2002
 P= I did the best I could on this one….but I had to eye most of it. Favors. treatment. Favors. control. Saver, et al Lancet")
50
Large Randomized Trials of IV tPA for Treatment of Acute Stroke
Study N Dose Time Window ECASS I – 6 NINDS – 3 ECASS II – 6 ATLANTIS A – 6 ATLANTIS B – 5

51
Modified Rankin 0-1 at Day 90
Adjusted odds ratio (95% CI) by stroke onset to treatment time, ITT population (N=2776)
 by stroke onset. to treatment time, ITT population (N=2776)")
52
Endpoint is global outcome scale as used in the NINDS trials.
Study name Statistics for each study Odds ratio and 95% CI Odds Lower Upper ratio limit p-Value ECASS 3 1.28 1.00 1.65 0.048 IPD 1.34 1.04 1.72 0.023 1.31 1.10 1.56 0.003 0.5 1 2 Favours Placebo tPA Metaanalysis of tPA trials within 3 to 4hrs 30 minutes after symptom onset. (n=1622) Endpoint is global outcome scale as used in the NINDS trials.
 Endpoint is global outcome scale as used in the NINDS trials.")
53
Metaanalysis of tPA trials within 3 to 4hrs 30 metaanalysis
Study name Statistics for each study Odds ratio and 95% CI Odds Lower Upper ratio limit p-Value ECASS3 0.805 0.477 1.358 0.416 IPD 1.111 0.731 1.690 0.621 0.980 0.706 1.359 0.903 0.5 1 2 Metaanalysis of tPA trials within 3 to 4hrs 30 metaanalysis Endpoint is death

54
Large Randomized Trials of IV tPA for Treatment of Acute Stroke
Study N Dose Time Window ECASS I – 6 NINDS – 3 ECASS II – 6 ATLANTIS A – 6 ATLANTIS B – 5 ECASS

55
Waarom kan de huisarts dit niet reeds starten?
Helaas kan onderscheid tussen bloeding en ischemie niet gemaakt worden: CT nodig Wat kan de huisarts doen? Herkennen van CVA Zo snel mogelijk doorsturen naar ziekenhuis waar trombolyse gebeurt Niet starten met SC LMW heparines of aspirine

56
Wat is een stroke unit? Gelokalizeerde eenheid in hospitaal
Geleid door arts met ervaring in CVA Multidisciplinair team met ergotherapeut, logopedist, kine, sociaal assistent Snel begin van revalidatie Snel nadenken over oorzaak en pathogenese van het CVA en beschikbaarheid van onderzoeken

57
Terug naar thuissituatie

58
Effect op mortaliteit

59
Short-term Prognosis after Emergency Department Diagnosis of TIA
30.0% Outcome events Inclusion criteria: Objective: Outcome measures: Total events: TIA by ED physicians Short-term risk of stroke after ED diagnosis Risk of stroke and other events during the 90 days after index TIA 25.1% 25.0% 20.0% 15.0% 12.7% 10.5% 10.0% Within 90 days Talking Points This study investigated the short-term risk of stroke and other adverse events in 1, patients after emergency department diagnosis of TIA. During the 90 days after index TIA, a total of 428 patients (25.1%) experienced a stroke or other adverse events. (red bar) This included strokes (10.5%), recurrent TIAs (12.7%), cardiovascular events (2.6%) and deaths (2.6%).(15) (yellow bars) Background The study results indicate that the short-term risk of stroke, other adverse events and deaths among patients who present to an emergency department with a TIA is substantial.(15) Half of the strokes occurred within 2 days of the TIA. Short-term risks of cardiovascular events, death, and recurrent TIA were also high.(15) Currently available interventions for patients with TIA may not be cost-effective if used in all such patients. This study identified 5 independent risk factors for stroke within 90 days after TIA: age older than 60 years, diabetes mellitus, duration of episode greater than 10 minutes, and weakness and speech impairment with the episode. These risk factors may identify patients whose symptoms are more likely due to cerebral ischemia or may indicate pathophysiological conditions associated with greater risk.(15) 5.0% 5.3% 2.6% 2.6% Within 48 hr 0.0% Stroke Recurrent TIA CV event Death Johnston SC, et al. JAMA 2000;284:
 experienced a stroke or other adverse events. (red bar) This included strokes (10.5%), recurrent TIAs (12.7%), cardiovascular events (2.6%) and deaths (2.6%).(15) (yellow bars) Background. The study results indicate that the short-term risk of stroke, other adverse events and deaths among patients who present to an emergency department with a TIA is substantial.(15) Half of the strokes occurred within 2 days of the TIA. Short-term risks of cardiovascular events, death, and recurrent TIA were also high.(15) Currently available interventions for patients with TIA may not be cost-effective if used in all such patients. This study identified 5 independent risk factors for stroke within 90 days after TIA: age older than 60 years, diabetes mellitus, duration of episode greater than 10 minutes, and weakness and speech impairment with the episode. These risk factors may identify patients whose symptoms are more likely due to cerebral ischemia or may indicate pathophysiological conditions associated with greater risk.(15) 5.0% 5.3% 2.6% 2.6% Within 48 hr. 0.0% Stroke. Recurrent. TIA. CV event. Death. Johnston SC, et al. JAMA 2000;284:")
60
ABCD2 Score for Transient Ischemic Attack (TIA)
A (Age); 1 point for age >60 years, B (Blood pressure > 140/90 mmHg); 1 point for hypertension at the acute evaluation, C (Clinical features); 2 points for unilateral weakness, 1 for speech disturbance without weakness, and D (symptom Duration); 1 point for 10–59 minutes, 2 points for >60 minutes. D (Diabetes); 1 point Total scores ranged from 0 (lowest risk) to 7 (highest risk).
; 1 point for age >60 years, B (Blood pressure > 140/90 mmHg); 1 point for hypertension at the acute evaluation, C (Clinical features); 2 points for unilateral weakness, 1 for speech disturbance without weakness, and. D (symptom Duration); 1 point for 10–59 minutes, 2 points for >60 minutes. D (Diabetes); 1 point. Total scores ranged from 0 (lowest risk) to 7 (highest risk).")
61
Risico ifv ABCD2 score Laag risico 0-3 Matig risico=4-5
Risico binnen 48 u 1% Matig risico=4-5 Risico binnen 48u 4.1% Hoog risico >5 Risico binnen 48u 8%

62
CVA primaire preventie
JUPITER studie toont hsCRP als nieuwe risicofactor Asymptomatische carotisstenose: enkel in zeer geselecteerde gevallen Risicostratificatie bij VKF met CHADS2 score

63
CVA secundaire preventie
TIA’s zijn urgenties Plaatjesremmers: geen verschil tussen Plavix en Aggrenox Geen combinatie Plavix & Aspirine tenzij absolute indicatie (coronaire problematiek) Statines post-cva aangewezen Simvastatine Atorvastatine
 Statines post-cva aangewezen. Simvastatine. Atorvastatine.")
64
CVA Acute behandeling Elke minuut telt
Geen twijfel meer dat tPA doeltreffend is

Verwante presentaties








>")
>")











