Download de presentatie
De presentatie wordt gedownload. Even geduld aub

1
Christophe George Gastro-enteroloog AZ Groeninge Kortrijk
Malabsorptie Christophe George Gastro-enteroloog AZ Groeninge Kortrijk

2
Malabsorptie Primair: congenitale defecten in het membraan transport thv het dunne darm epitheel Secundair: verworven Kan ook ontstaan doordat de voedingsstoffen slecht verteerd worden in het lumen van de dundarm

3
Malabsorptie 3 factoren noodzakelijk voor absorptie van voedingsstoffen 1. Vertering in het lumen van de dunne darm 2. Absorptie door de intestinale mucosa 3. Transport van de opgenomen stoffen naar de circulatie

4
Malabsorptie Klinische presentatie is heel wisselend en afhankelijk van de graad van malabsorptie: - partieel : vb preferentieel element vb:Vit B 12 - totaal: vb. atrofie dundarmmucosa vb: gluten enteropathie Meest voorkomende symptomen: - vermagering - intestinale ongemakken : winderigheid, darmrommelingen - diarree, steatorree

5
malabsorptie Vitamine B12 deficiëntie Glutenenteropathie
Bacteriële overgroei Giardia Lamblia Bariatrische heelkunde

6
Vit B12 deficiëntie

7
Vit B12 deficiëntie Adequate opname van vit B12 berust op 3 factoren
- aanwezigheid in voeding - pepsine: bevrijdt het B12 van de bindingseiwitten - pancreatische proteasen - intrinsic factor: opname complex B12 en IF thv terminale ileum

8
Vitamine B12 deficiëntie
megaloblastische anemie rode tong neuropathie Oorzaken: atrofische gastritis en achlorhydrie, ileale resectie, bacteriële Overgroei,… Behandeling : substitutie

9
Coeliaki Epidemiologie/Prevalentie Pathosfysiologie Kliniek
Geassocieerde pathologie en complicaties Diagnostiek Therapie

10
Epidemiologie en prevalentie
Blanken en vooral Noord-Europeanen Van 1: uiteindelijk naar 1:200 naar 1%?

11
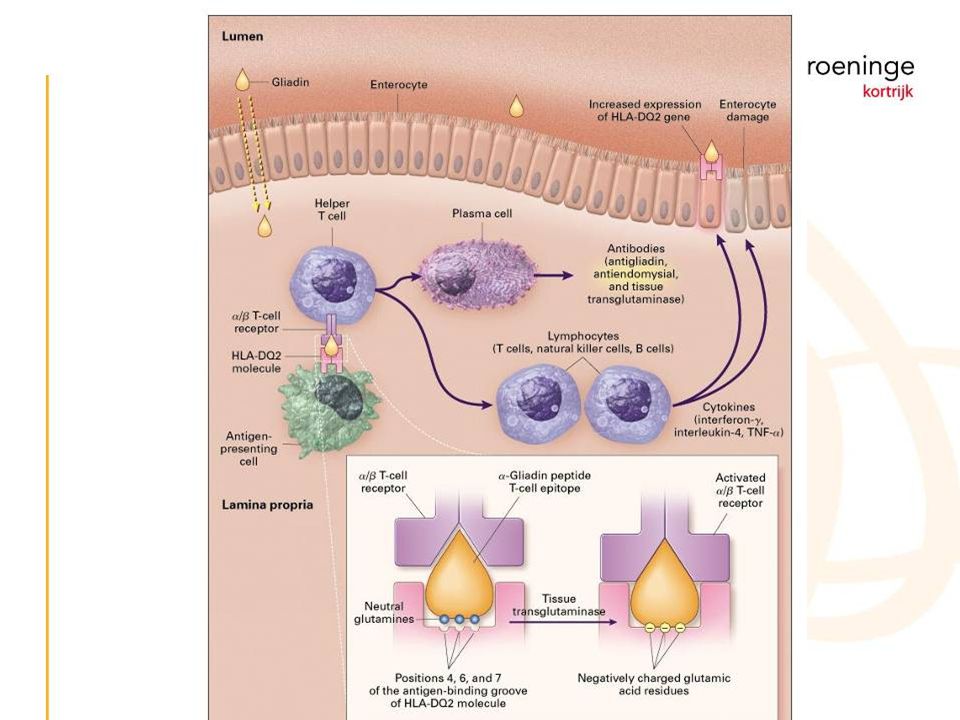
2. Pathofysiologie Genetische predispositie:
eerste graads verwanten 1:22 HLA-DQ2/HLA-DQ8/? Omgevingsfactor: gluten (tarwe-rogge-gerst) Immunologische interactie:
 Immunologische interactie:")
13
3. Kliniek Diarree, steatorree, flatulentie en meteorisme.
Malabsorptie geassocieerde symptomen: - groeiachterstand, gewichtsverlies - anemie, ijzerdeficiëntie - neurologische afwijkingen - botafwijkingen op Vit D- en Ca-tekort - fertiliteitsstoornissen Subklinisch verloop

14
4. Geassocieerde pathologie en complicaties
Verhoogd risico op maligniteit ?: -(Tcel)Lymfomen (30 tot 100x) -Orofaryngeale tumoren -Dundarm en coloncarcinoom -Hepatocellulair carcinoom (Verlaagd risico op borst-en longcarcinoom)
Lymfomen (30 tot 100x) -Orofaryngeale tumoren. -Dundarm en coloncarcinoom. -Hepatocellulair carcinoom. (Verlaagd risico op borst-en longcarcinoom)")
15
Associatie met: - Dermatitis herpetiformis - Type I Diabetes mellitus (3-8%) - Downsyndroom - Leverpathologie - Schildklierpathologie - Ig A deficiëntie - Infertiliteit - Cardiomyopathie en myocarditis

17
5. Diagnose Hoe testen? 1.Klinisch-anamnestisch vermoeden 2.Biochemie:
- vitaminedosages… - levertesten

18
-immunofluorescentie test
3. Serologie: *IgA Endomisium Ab -immunofluorescentie test -specificiteit (97-100%) sensitiviteit (85-98%) -moeilijk te kwantificeren en vrij duur *IgA t-Transglutaminase Ab -ELISA -specificiteit (95-97%) sensitiviteit (90-98%) -therapiemonitoring *IgA en IGG Anti-gliadine antistoffen -specificiteit (82-95%) sensitiviteit (75-90%)
 sensitiviteit (85-98%) -moeilijk te kwantificeren en vrij duur. *IgA t-Transglutaminase Ab. -ELISA. -specificiteit (95-97%) sensitiviteit (90-98%) -therapiemonitoring. *IgA en IGG Anti-gliadine antistoffen. -specificiteit (82-95%) sensitiviteit (75-90%)")
19
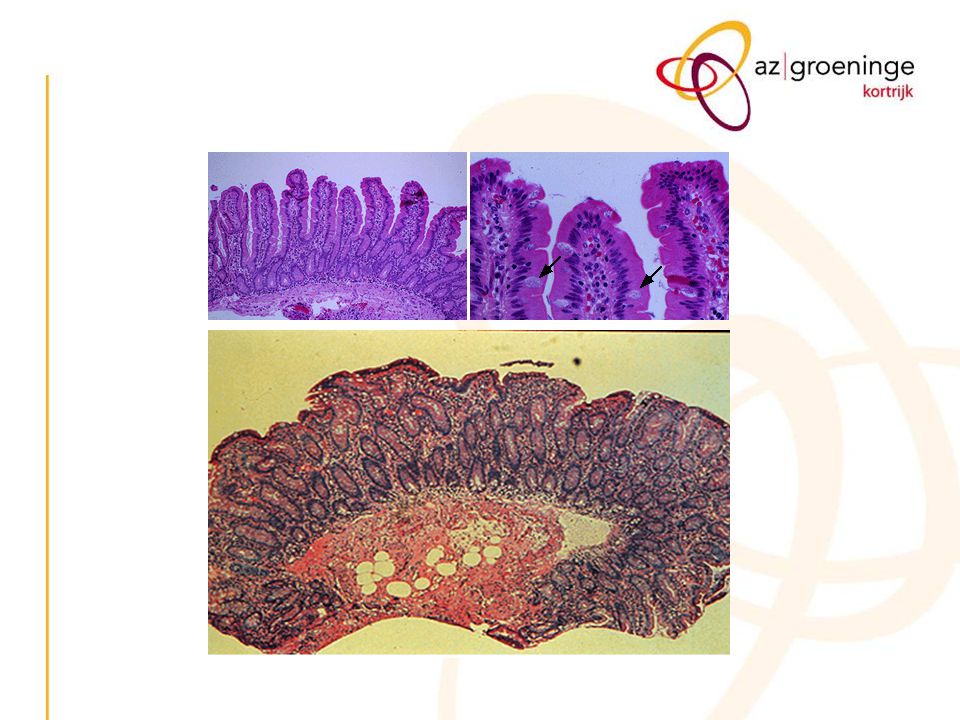
- intraepitheliale lymfocytose 5.In kaart brengen van complicaties
4.Duodenumbiopten: - villusatrofie - crypthyperplasie - intraepitheliale lymfocytose 5.In kaart brengen van complicaties 6.Opsporen HLA DQ2 en DQ8 -indien reeds onder een glutenvrij-dieet zonder echte diagnose sensitiviteit 90-95%. -screening bij familieleden? -bij onduidelijke diagnose

21
Wie testen? Screening? -voordelen: moeilijk in te schatten bij asymptomatische patiënt -nadeel: weinig dieetcompliance bij asymptomatische patiënt. gezonde patiënt ziek verklaren.

22
6. Therapie Glutenvrij dieet: vrij van tarwe,rogge,herst oats?
Nutritionele te korten bijsturen Pneumococcenvaccinatie ikv hyposplenisme effectmonitoring mbv serologietesten

23
Flora of small intestine is crucial to proper bowel function
Bv medicatie opname Differentiatie tussen commensale en pathogene bacterieën Flora of small intestine is crucial to proper bowel function – normal immune function – normal digestion of nutrients If the flora of the small bowel is altered, inflammation or altered digestion can occur, leading to symptoms. 23

24
24

25
Mechanisms protecting against bacterial overgrowth
Antegrade peristalsis (MMC) prevents attachment of ingested microorganisms Gastric acid and bile destroy many MO before they leave the stomach Digestion by proteolytic enzymes helps destroy bacteria in the small intestine Intestinal mucus layer traps bacteria Intact ileocecal valve inhibits retrograde translocation of bacteria from the colon to the small bowel Immune system ? (cfr high prevalence in pt with immunodeficiency) Secretory IgA aids in preventing bacterial proliferation 25
 prevents attachment of ingested microorganisms. Gastric acid and bile destroy many MO before they leave the stomach. Digestion by proteolytic enzymes helps destroy bacteria in the small intestine. Intestinal mucus layer traps bacteria. Intact ileocecal valve inhibits retrograde translocation of bacteria from the colon to the small bowel. Immune system (cfr high prevalence in pt with immunodeficiency) Secretory IgA aids in preventing bacterial proliferation. 25.")
26
Risc Factors and causes
disordered motility or movement of the small bowel or anatomical changes (idiopathic or iatrogenous) that lead to stasis (2) disorders in the immune system (3) conditions that cause more bacteria from the colon to enter the small bowel 26
 that lead to stasis. (2) disorders in the immune system. (3) conditions that cause more bacteria. from the colon to enter the small bowel. 26.")
27
Small intestinal stasis
Abnormal small intestinal motility Diabetes mellitus Scleroderma Idiopathic intestinal pseudoobstruction Radiation enteritis Crohn's disease Anatomic abnormalities Small intestinal diverticulosis Surgically created blind loops (end-to-side anastomosis) Strictures (Crohn's disease, radiation, surgery) Resectie van dundarm: “ adaptatie respons” => diepere cryptes, langere villi => grotere absorptie – oppervlakte Neiging voor dilatatie van dundarm => vertraging van de transit: om nutritionele absorptie te verhogen ! Blind loop syndrome ! Abnormal communication between the proximal and distal gastrointestinal tract Gastrocolic or jejunocolic fistula Barriatric surgery Resection of the ileocecal valve 27
 Strictures. (Crohn s disease, radiation, surgery) Resectie van dundarm: adaptatie respons => diepere cryptes, langere villi => grotere absorptie – oppervlakte. Neiging voor dilatatie van dundarm. => vertraging van de transit: om nutritionele absorptie te verhogen ! Blind loop syndrome ! Abnormal communication between the proximal and distal gastrointestinal tract. Gastrocolic or jejunocolic fistula. Barriatric surgery. Resection of the ileocecal valve. 27.")
28
Pathogenesis Inflammation Vit B12 absorption Cell injury
Enteric Bacteria Deconjugation of bile acids Degradation of carohydrate Anaeroben: productie van enterotoxine en directe adherence met injury Aeroben: enzyme en metabole producten waardoor inducing epithelial cell injury Anaeroben absorpberen competitive Vit B12 Degradation of proteins 28

29
Short chain fatty acids
Enteric Bacteria Degradation of carbohydrate Short chain fatty acids CO2, Hydrogen, methane Malabsorption of carbohydrate Acidic stools, abdominal distension, flatulence 29

30
Encephalopathy, protein loosing enteropathy
Enteric Bacteria Cell injury Degradation of proteins Urea Ammonia Malabsoption of proteins Encephalopathy, protein loosing enteropathy 30

31
Fat soluble vitamin deficiency & steatorrhea
Enteric Bacteria Deconjugation of bile acids Deconjugatie van bile acids: reabsorptie in jejunum waardoor te kleine concentraties voor opname Fat malabsorption Free bile acids Fat soluble vitamin deficiency & steatorrhea 31

32
Fat soluble vitamin deficiency & steatorrhea
Enteric Bacteria Deconjugation of bile acids Deconjugatie van bile acids: reabsorptie in jejunum waardoor te kleine concentraties voor opname Fat malabsorption Free bile acids Fat soluble vitamin deficiency & steatorrhea 32

33
Clinical presentation
Non specific Nausea, dyspepsia, bloating , flatulence, abdominal pain, watery diarrhea Weight loss, failure to gain weight in children Malabsorption: Steatorrhee, Fatigue Tetany– Night blindness – Dermatitis – arthritis – hepatic injury Fatigue door anemie, tetany door hypocalciemie Artritis door overagrgressive respons op absorbed bacterila antigenen, dat leidt tot immune dysregulatie !! 33

34
Jejunal aspiration “Gold Standard” - Quantitative detection of excessive bacterial concentration in jenunal aspirate ( < endoscopy or fluoroscopy with jejunal intubation) - > 105 bacteria per ml intestinal fluid (nl < 104 bacteria/ml) includes gram postive flora (< upper respiratory flora) > colonic bacteria ! Limitations: - not all species can be identified. ( > 500 sp) / not always representative - Fals positive results due to contamination of oropharyngeal flora - Fals negative results due to patchy / difficult to access localisation (predisposing abnormality) 34
 - > 105 bacteria per ml intestinal fluid (nl < 104 bacteria/ml) includes gram postive flora (< upper respiratory flora) > 105 colonic bacteria ! Limitations: - not all species can be identified. ( > 500 sp) / not always representative. - Fals positive results due to contamination of oropharyngeal flora. - Fals negative results due to patchy / difficult to access localisation. (predisposing abnormality) 34.")
35
Principle of breath tests
Sugers exposed to bacteria in the bowel substrate metabolised tot H2 and absorbed an expired 35

36
Bile acid breath test 14C-Glycochol zuur
Original test for diagnosing SIBO Based on ability of many types of bacteria to deconjugate bile acids Can’t differ bile acid malabsorption and SIBO 36

37
Bile acid breath test Ademstalen per 30’ gedurende 6 u
Lage dosis radioactiviteit: niet bij kinderen en zwangere vrouwen Normaalwaarde : Cum% 6u < 3% 37

38
Lactulose breath test Passes unabsorbed through small bowel into colon. (orocaecal transit) Superior for detection of ileal bacterial overgrowth? “positive” test: - early H2 peak (>20 ppm) min 15’ before prolonged peak (colon) - rise in H2 within 90 ‘ CAVE Lactulosis accelerates small bowel transit No 2e peak with rapid transit 2 distingueshable peaks (caecum / colon) 38
 min 15’ before prolonged peak (colon) - rise in H2 within 90 ‘ CAVE. Lactulosis accelerates small bowel transit. No 2e peak with rapid transit. 2 distingueshable peaks (caecum / colon) 38.")
39
Glucose Lactulose Lactulose test: early biek due to small bowel bact: later due passage of remaining laculose into the colon M Simre´n, P-O Stotzer Use and abuse of Hydrogen breath tests Gut 2006;55:297–303 39

40
Antibiotics Proposal: 10 days each 3 months Vibratab 50mg
Tetracyclines Amoxicillin-clavulanate plus metronidazole A combination of a cephalosporin, such as cefalosporin or trimethoprim-sulfamethoxazole with metronidazole Norfloxacin Oral gentamicin and metronidazole. Rifaximin improves also IBS symptoms Proposal: 10 days each 3 months Vibratab 50mg Flagyl 250 2*/D Tarivid 200mg 1*/D 40

41
Probiotica Probiotica are bacterial preparations
that alter the bacterial flora in the bowel => role in bacterial overgrowth is somewhat uncertain 41

42
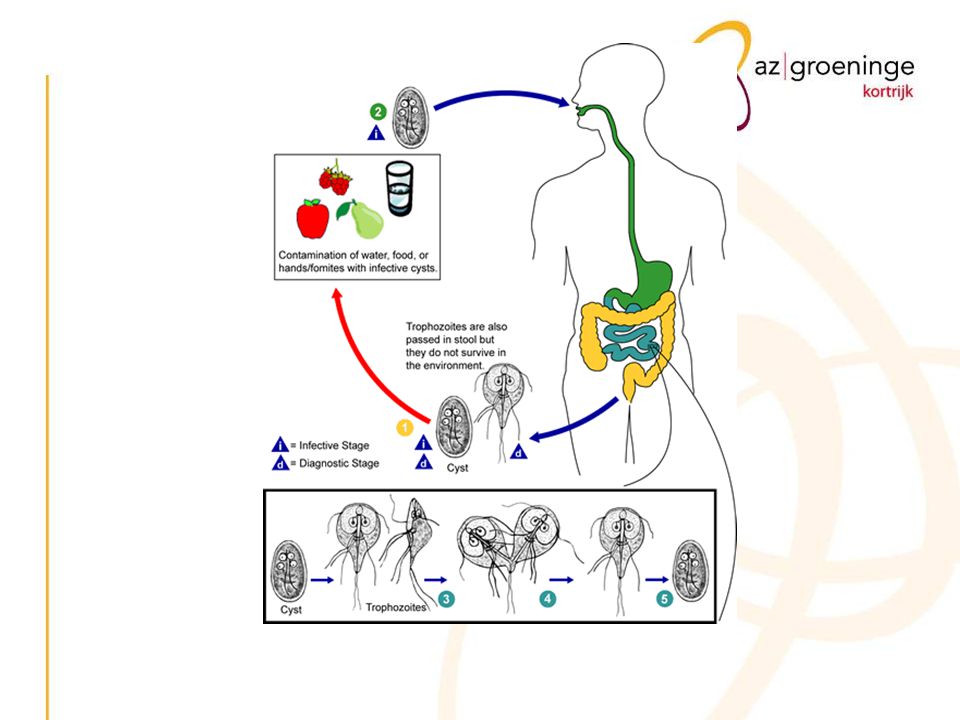
Giardiase Giardia Lamblia ontwikkelingslanden kids, reizigers,
immuungecompromitteerden Frequente oorzaak van reizigersdiarree ged > 2w. Ingestie van oocysts is voldoende hypochlorhydrie Transmissie: faeco-oraal (mens-mens, besmet water, besmet voedsel)
")
44
Giardiase Kliniek Asymptomatisch +/- 60% Acute Giardiase < 50%
Chronische Giardiase Up to Date

45
Giardiase Acute Giardiase < 50% diarree (90%) malaise (85%)
steatorree (70%) flatulentie (75%) nausea (70%) vermagering (65%) braken (30%) meestal na incubatie periode van 1-2w symptomen duren ong. 2-4w
 flatulentie (75%) nausea (70%) vermagering (65%) braken (30%) meestal na incubatie periode van 1-2w. symptomen duren ong. 2-4w.")
46
Giardiase Chronische Giardiase
plattere stoelgang, gewoonlijk geen diarree steatorree ernstig gewichtsverlies malabsorptie vb- verworven lactose intolerantie malaise, vermoeidheid en depressie krampen, bloating en flatulentie meestal op- en afgaand ged. maanden

47
Giardiase Diagnose obv microscopisch onderzoek van de stoelgang
Ag detectie in de stoelgang duodenum biopsies: villusatrofie en crypthyperplasie duodenumaspiraat

48
Giardiase Therapie Tinidazole (Fasigyn): éénmalig 2g
efficiëntie van 90% ! Igv refractair of vroegtijdig recidief; ALTIJD eerst nieuwe cultuur ! meestal tgv lactose intolerantie, eerder dan tgv recidief infectie Tinidazole (Fasigyn): 2g dd. ged. 3d Metronidazole (Flagyl): 500mg 3xdd. ged 14d + Quinacrine (…): 100mg 3xdd. ged 14d
: 2g dd. ged. 3d. Metronidazole (Flagyl): 500mg 3xdd. ged 14d. + Quinacrine (…): 100mg 3xdd. ged 14d.")
49
Bariatrische heelkunde

52
Procedures 2 principes Restrictie voedselinname ↓
Malabsorptie voedselopname ↓ Maagvolume reduceren en zo verplichten voedselinname verminderen en te fractioneren Door derivatietechnieken het gastrointestinale oppervlakte reduceren 52

53
Laparoscopisc adjustable gastric banding “Maagring” LapBand®
Siliconebandje rond bovenste deel maag (cardia) → “zandlopereffect” Reservoir 15 à 20 cc Aanpasbaar door onderhuidse inspuiting Omkeerbaar Laparoscopisch Relatief goedkoop Meest frequent in Europa Sinds jaren ’90 in Europa en Australië, slechts sinds 2001 goedgekeurd in USA 2000 € Bv aanpassen tijdens zwangerschap 53
 → zandlopereffect Reservoir 15 à 20 cc. Aanpasbaar door onderhuidse inspuiting. Omkeerbaar. Laparoscopisch. Relatief goedkoop. Meest frequent in Europa. Sinds jaren ’90 in Europa en Australië, slechts sinds 2001 goedgekeurd in USA € Bv aanpassen tijdens zwangerschap. 53.")
54
Vertical Banded Gastroplasty “Mason”
Bovenste gedeelte maag geniet of doorgehaald (“Mac Lean”) over 6 cm om maagreservoir te vormen Ring aan uiteinde maagreservoir om maaglediging te vertragen
 over 6 cm om maagreservoir te vormen. Ring aan uiteinde maagreservoir om maaglediging te vertragen.")
55
Laparoscopic Sleeve Gastrectomy
Partiële gastrectomie met verwijdering grootste deel grote curvatuur Creatie kleine starre tubulaire maag Nieuwe techniek!!! Veilig!!! “sleeve” engels: mouw Kleine maag, resistent aan stretching gezien afwezigheid van fundus, vermindering hormoonproductie ~ regulatie voedselinname 55

56
“Maagballon” Endoscopisch geplaatste siliconeballon thv de maag, cc fysiologisch/lucht Tijdelijk: maximaal 6 maanden ter plaatse!!! Bij matige obesitas: ondersteuning bij aanleren betere voedingsgewoonten Effectiviteit 25% Complicaties: oesophagitis R/PPI Restrictie en verzadiging Na 6 maanden verwijderen of vervangen In principe evacuatie via maagdarmkanaal mogelijk zo leeg, meestal endoscopisch verwijderd Bij ernstige obesitas met hoog operatief risico, om eerst wat gewichtsreductie te bekomen voor uitgebreidere chirurgie (bewezen nut) Zelden comlicaties: Kapotgaan < aanvreten door “maagzuur” Wel misselijkheid en braken na plaatsing (eerste week) 56
 Zelden comlicaties: Kapotgaan < aanvreten door maagzuur Wel misselijkheid en braken na plaatsing (eerste week) 56.")
57
Bileopancreatic Diversion “Scopinaro”
Partiële gastrectomie 1/3 tot 2/3 Sectie darm op 250cm van caecum enterische arm 200cm → gastro-ileostomie (Roux-en-Y) biliopancreatische arm 250cm → implantatie op 50cm van caecum gemeenschappelijke arm 50cm Meestal ook: Cholecystectomie Appendectomie
 biliopancreatische arm 250cm. → implantatie op 50cm van caecum. gemeenschappelijke arm 50cm. Meestal ook: Cholecystectomie. Appendectomie.")
58
Roux-en-Y Gastric Bypass “Maag bypass”
Klein maagreservoir geniet of doorgehaald Sectie darm thv begin jejunum enterische arm 75cm – 150cm → gastro-jejunostomie (Roux-en-Y) biliopancreatische arm → implantatie thv jejunum Meest frequent in Amerika
 biliopancreatische arm. → implantatie thv jejunum. Meest frequent in Amerika.")
59
Metabole complicaties
Fe-deficiëntie 50% → microcytaire anemie < ↓ aanbod uit voeding < ↓ maagzuur en ↓ uptake in maag en duodenum Risicogroep: menstruerende vrouwen → preventief ijzerinname R/Fe oraal 640mg/d meestal voldoende Gegevens voor RYGB Fe: betere opname in combinatie met vitamine C DD GI bloeding Halverson JD et al. Am Surg 1986; 52:594. 59

60
Metabole complicaties
Vit B12-deficiëntie % → macrocytaire anemie → pancytopenie, glossitis, PNP < ↓ aanbod uit voeding < ↓ maagzuur en ↓ IF productie R/ Vit B12 oraal 350 µg/d Vit B12 IM 1mg/3maanden Halverson JD et al. Am Surg 1986; 52:594.

61
Metabole complicaties
Foliumzuurdeficiëntie 0,03-38% → ~ vit B12 deficiëntie < ↓ aanbod uit voeding < ↓ uptake duodenum R/ Fz oraal 0,4mg/d !!!CAVE zwangere vrouwen: hogere dosis preventie neurale buisdefecten Halverson JD et al. Am Surg 1986; 52:594.

62
Metabole complicaties
Thiaminedeficiëntie → Wernicke-Korsakoff syndroom nystagmus, oftalmoplegie, ∆mentaal < ↓ aanbod uit voeding < ↓ uptake jejunum en ileum Vooral bij persisterend braken R/ Vit B1 oraal 50mg/d !!! CAVE acute Wernicke R/Thiamine 100mg IV Vitamine B1 Nooit glucose voor thiamine kan Wernicke provoceren of verergeren Singh S et al. Neurology 2007; 68:807. 62

63
Metabole complicaties
Eiwitmalabsorptie zelden bij RYGB → oedemen, ascites, pleuravocht < ↓ aanbod uit voeding < ↓ opname R/ voldoende orale eiwitinname TPN Vooral bij jejunale bypass 63

64
Metabole complicaties
Ca en Vit D deficiëntie → secundaire hyperparathyroidie → botaantasting en osteopenie < ↓ aanbod Vit D uit voeding < ↓ uptake Ca in duodenum R/ Vit D oraal 800 IU/d Ca oraal mg/d De Prisco C et al. Am J Med Sci 2005; 329:57.

65
Metabole complicaties
Vit A deficiëntie → nachtblindheid, xeroftalmie Enkel bij BPD : 52% na 1j R/Rovignon® (vit A en Vit E) Vit K deficiëntie vaak gedaalde PT, zelden complicaties Zink deficiëntie vaak gedaald → haaruitval
 Vit K deficiëntie. vaak gedaalde PT, zelden complicaties. Zink deficiëntie. vaak gedaald → haaruitval.")
Verwante presentaties




 SEPSIS>")



>")







to watch throughout the month of August,>")






