Download de presentatie
De presentatie wordt gedownload. Even geduld aub

1
Infectieuze verwikkelingen bij HIV infectie
E. Van Wijngaerden Aidsreferentiecentrum UZ-KULeuven

3
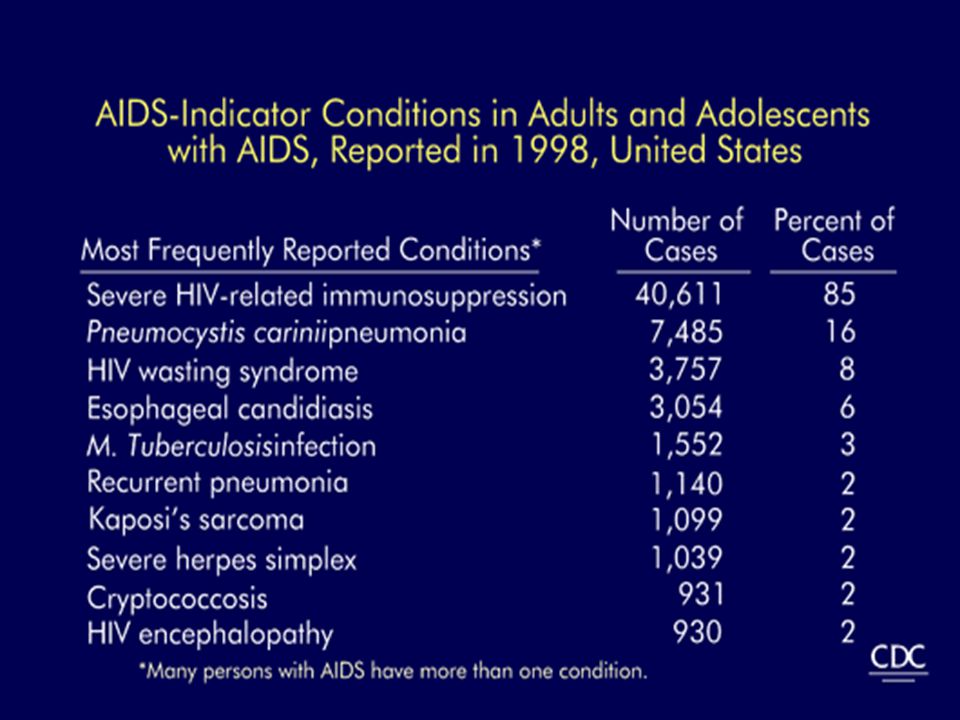
“Opportunistische” infecties
Sommige veel frequenter zo immuundef.: zona, orale Candida, bact. pneumonie Andere alleen zo immuundef.: Pneumocystis, diss.MAC, cereb. toxo Naast infecties ook tumoren: Kaposi’s sarcoma, B-cel non-Hodgkin’s lymfoma

4
Opportunistische infecties
Viraal: VZV, HSV, CMV, PML, (EBV-NHL, HHV8-KS)... Bacterieel: Mycobacterium (MTB, MAC), Salmonella, Bartonella... Fungi: Pneumocystis jiroveci, Cryptococcus, Candida, Aspergillus, Histoplasma, Penicillium... Protozoa: Toxoplasma, Cryptosporidium, Isospora, Leishmania...
... Bacterieel: Mycobacterium (MTB, MAC), Salmonella, Bartonella... Fungi: Pneumocystis jiroveci, Cryptococcus, Candida, Aspergillus, Histoplasma, Penicillium... Protozoa: Toxoplasma, Cryptosporidium, Isospora, Leishmania...")
6
Preventie: primaire profylaxe
Pneumocystis Toxoplasma Tuberculose Cryptococcose Mycobacterium avium complex (MAC) Breedspectrum? ART...
 Breedspectrum ART...")
7
Wat heeft patient: basisvragen
Welk klinisch beeld? Huidig CD4 cel aantal? Van waar komt hij? Krijgt hij profylaxe? Werd ART opgestart, en wanneer?

8
Welk klinisch beeld? Denk in syndromen:
Longaantasting (PCP, TB, bact,…) Hersenaantasting (toxo, crypto, PML,…) Abdominale symptomen (Mycobact, NHL,…) Huidafwijkingen (KS, VZV, Penicill., BA…) Klieren/milt/lever: RES: (Mycobact, NHL…) ...
 Hersenaantasting (toxo, crypto, PML,…) Abdominale symptomen (Mycobact, NHL,…) Huidafwijkingen (KS, VZV, Penicill., BA…) Klieren/milt/lever: RES: (Mycobact, NHL…) ...")
9
Huidig CD4 cel aantal? Alles wordt frequenter naarmate het CD4 cel aantal verder zakt

10
Ziekte over 3j ifv CD4 en VL

12
Huidig CD4 cel aantal? Alles wordt frequenter naarmate het CD4 cel aantal verder zakt Voor vele OI soort cut-off: Geen: NHL, KS, TBC, zona <200: PCP, orale candida, hairy leukoplakie <100: toxo, oesof.candida, crypto, PML <50: MAC, CMV, PBL

13
Rates of AIDS events stratified by CD4 cell count at the start of 2 periods after initiating highly active antiretroviral therapy (HAART) The Antiretroviral Therapy Cohort Collaboration*, Arch Intern Med 2005;165: Copyright restrictions may apply.

14
Van waar komt de patient?
Westen versus Afrika/Azie A: TB, nog eens TB, dan de rest Thailand: penicilliose US versus Europa: US: meer MAC, ook histoplasmose, coccidioidomycose Zuid-Europa vs onze streken Z: meer TB, leishmaniase

15
Krijgt hij profylaxe? PCP profylaxe zo CD4 < 200 (<14%):
Zo cotrimoxazole langer en goed genomen: PCP (en toxo) bijna onbestaande Geldt minder voor pentamidine aerosol
 bijna onbestaande. Geldt minder voor pentamidine aerosol.")
16
Werd ART opgestart, en wanneer?
Risico op OI daalt dramatisch na opstarten ART Succesvolle ART = onderdrukte VL sedert maanden: minder OI voor zelfde CD4

17
AIDS incidence (the blue bars), mortality (in red), and AIDS prevalence (in pink) are represented on this graph: The prevalence curve may be divided in three parts according to inflexion points: - the first part –up to is mostly driven by the increasing incidence of aids cases, - the second part – from 1992 until is a leveling - where the mortality nearly reached the AIDS incidence, - and the third part –after 1996-, -with an increasing slope-, mostly driven by the impact of highly active antiretroviral treatments on AIDS mortality. The evolution of the AIDS prevalence has obvious implications for medical care organisation and surveillance of resistance. Decreasing mortality has also implications for prevention: the lower infectivity related to decreased viral load induced by treatments may be counterbalanced by a prolonged survival if more protective behaviours are not promoted. (1 min) (413 lost follow up during the whole period)
 (413 lost follow up during the whole period)")
18
Incidences of 15 AIDS-defining events in 5 time periods after initiation of highly active antiretroviral therapy (HAART) The Antiretroviral Therapy Cohort Collaboration*, Arch Intern Med 2005;165: Copyright restrictions may apply.

19
Werd ART opgestart, en wanneer?
Risico op OI daalt dramatisch na opstarten ART Succesvolle ART = onderdrukte VL sedert maanden: minder OI voor zelfde CD4 Maar eerste weken-maanden: IRIS

20
IRIS Immuunreconstitutiesyndroom
Weken, zelden maanden na opstarten ART Vaak al voor belangrijke recuperatie CD4 Hoe lager CD4, hoe meer Kan waarschijnlijk bij alle OI

21
IRIS Ziek blijven Ziek worden Opnieuw ziek worden Diff diagnose:
OI reageert niet Nieuwe OI IRIS Nevenwerking geneesmiddelen

22
Capita selecta OI Pneumocystis jiroveci pneumonie
Mycobacteriële infecties Cryptococcose Mucosale candidiase Cerebrale toxoplasmose Cytomegalovirus infectie Non-hodgkin’s lymfoma Kaposi’s sarcoma NB: hepatitis B en C

23
Pneumocystis jiroveci pneumonie
Fungus, vroeger P. carinii, “PCP” Acute infectie of reactivatie Bijna altijd longaantasting, subacuut beeld: Droge hoest Koorts dyspnee CD4 < 200, soms iets hoger en hoe lager hoe frequenter

24
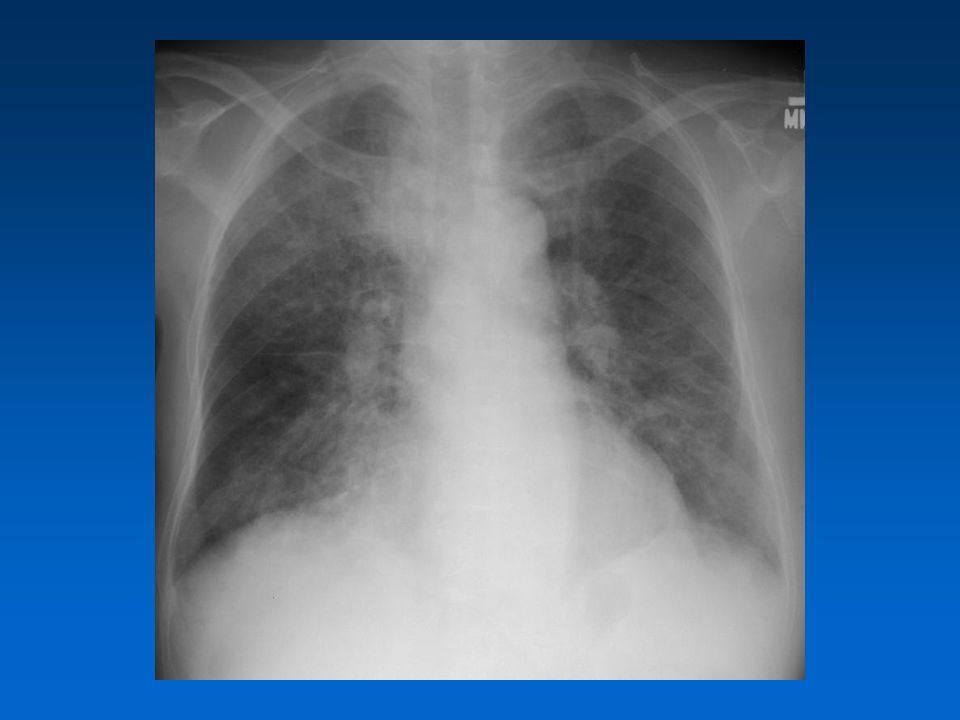
Pneumocystis jiroveci pneumonie
Labo niet specifiek: LDH stijging, bloedgassen evtl desaturatie RX extreem variabel

26
Pneumocystis jiroveci pneumonie
Labo niet specifiek: LDH stijging, bloedgassen evtl desaturatie RX extreem variabel Diagnose: Kliniek, RX Uitsluiten andere bronchoalveolaire lavage (zilverkleuring, IF, PCR)
")
27
Pneumocystis jiroveci pneumonie
Behandeling: cotrimoxazole 3 weken, vaak initieel met corticoiden ART starten na volledige behandeling Immuunreconstitutie niet zeldzaam Secundaire profylaxe tot CD4 > 200 >3m Primaire profylaxe zo CD4 < 200

28
Mycobacteriële infectie
Tuberculose meest frequent, besmettelijk en snelst dodend: prioriteit Mycobacterium avium complex Hele horde andere, zeldzaam

29
Tuberculose Mycobacterium tuberculosis, kan ook gezonden besmetten
Ziekte primair of reactivatie Klassiek longaantasting, bij AIDS frequent gedissemineerd: zeer variabele beelden, maar vaak met longaantasting Alle CD4 waarden, meer en atypischer zo lager

30
Tuberculose Denk aan epidemiologie: frequenter in Afrika en Azië
Intradermo pos of neg: helpt niet veel Labo aspecifiek inflammatoir, vaak ook leverfunctiestoornissen (cholestase) Imaging: RX, CT Diagnose: specifieke kleuringen op sputum, BAL of “diep” materiaal, specifieke kweek, gevoeligheidsbepaling
 Imaging: RX, CT. Diagnose: specifieke kleuringen op sputum, BAL of diep materiaal, specifieke kweek, gevoeligheidsbepaling.")
31
Tuberculose

32
Tuberculose: behandeling
Als bij niet-hiv patient 3-ledig 4-ledig zo allochtoon 6(-9) maanden, eerste 2 intensief IRIS frequent probleem: wachten met ART >2-4 weken zo <50 >2 maanden zo >200
 maanden, eerste 2 intensief. IRIS frequent probleem: wachten met ART. >2-4 weken zo <50. >2 maanden zo >200.")
33
Tuberculose: behandeling
Nevenwerkingen zeer frequent en problematisch: vooral lever, koorts, rash Geneesmiddeleninteracties en overlappende toxiciteit vermijden Gebruik PI problematisch Meestal 2 NRTI plus efavirenz D4t, ddI, ddC: cave neurotoxiciteit Abacavir: cave dd HSS

34
Tuberculose: preventie
Blootstelling mijden… Primaire profylaxe (“behandeling van latente TB”) Intradermo pos en geen actieve TB Contacten actieve, zelf geen actieve TB Isoniazide 9 maanden Geen secundaire profylaxe
 Intradermo pos en geen actieve TB. Contacten actieve, zelf geen actieve TB. Isoniazide 9 maanden. Geen secundaire profylaxe.")
35
Mycobacterium avium complex
Kiem uit omgeving: niet overdraagbaar Variabel, niet-acuut beeld van infectie van het RES: vaak zeer vaag Koorts Hepatosplenomegalie, cholestase, anemie Klieren, darmaantasting Weinig longaantasting CD4 < 50: gevorderde immuundeficiëntie

36
Mycobacterium avium complex
Imaging aspecifiek Kleuring/kweek aspiraat, bloed, beenmerg, biopsie... in functie van beeld Behandeling: clarythromycine plus ethambutol minstens 6 maanden én 3 maanden CD4 >100 IRIS zéér frequent probleem

37
Mycobacterium avium complex
Primaire profylaxe werd aanbevolen zo CD4 <50, syst in US, minder in EU Nu geen prioriteit: start ART

38
Cryptococcose Uit omgeving: niet overdraagbaar
Meestal subacute hersenvliesontsteking; Hoofdpijn, tekens van overdruk Meestal weinig tekens van meningitis Meestal koorts CD4 < 100; meer in Afrika CT meestal geen massa, LP met drukmeting Bloedkweek en antigeentest CSV lymfo (maar weinig), kleuring, kweek en antigeentest
, kleuring, kweek en antigeentest.")
39
Cryptococcose Amfotericine B plus flucytosine 2 weken, daarna fluconazole HD tot 8 weken Herhaalde LP zo intracran. overdruk HAART na eerste weken IRIS niet zeldzaam Sec profylaxe fluconazole tot 6 m > 100(200) Prim. preventie fluco? liever ART
 Prim. preventie fluco liever ART.")
40
Mucosale candidiase Normale commensaal
Orale, oesofageale, vaginale, peniele... Diagnose: op zicht (evtl oesofagoscopie)
")
41
Mucosale candidiase Behandeling: fluconazole
Vaak indicatie opstarten HAART, zeker zo recidiverend Sec profylaxe meestal niet nodig

42
Cerebrale toxoplasmose
Reactivatie: toxo IgG pos = at risk Beeld van RIP in hersenen Focale uitval Epilepsie Hoofdpijn, koorts CD4 < 100(200)
")
43
Cerebrale toxoplasmose
Imaging: CT, MRI Multipele ring-contrastcapterende letsels, oedeem

44
Cerebrale toxoplasmose
DD vooral lymfoma, bij twijfel LP met PCR of zelfs biopsie Meestal “empirische” therapie: pyrimethamine + sulfadiazine + folinezuur ged 6 weken ART te starten aansluitend, soms IRIS Daarna sec profylaxe, idem (of cotrim) tot > 6 m > 200
 tot > 6 m > 200.")
45
Cytomegalovirus Reactivatie, meest IgG positief
Extreem variabele beelden: retina, colon, long, koortssyndroom, neurologisch... CD4 < 50, zelden eerste event: zeer zeldzaam geworden sinds ART Levensbedreigende beelden bij extreem zieke patienten

46
Cytomegalovirus Diagnose moeilijk:
Biopsie, fundoscopie Stijgende CMV DNA PCR bij compatiebel beeld Behandeling: ganciclovir, foscarnet, cidofovir ART vrij dringend zo haalbaar IRIS niet zeldzaam

47
Non Hodgkin’s lymfoma B-cel maligniteit, meestal EBV gerelateerd
Beeld van “ruimte innemend proces”, in klieren, maar vaak daarbuiten Kan bij hogere CD4 cellen Diagnose: biopsie

48
Non Hodgkin’s lymfoma Chemotherapie
ART opstarten zo snel mogelijk, altijd PCP profylaxe Cave overlappende toxiciteit met chemo

49
Kaposi’s sarcoma KSHV of HHV8 geassocieerd
Meestal zichtbare letsels op huid en slijmvlies, soms oedeem, soms visceraal Alle CD4, vaker zo laag

50
Kaposi’s sarcoma Diagnose biopsie, maar vaak op zicht duidelijk
Zo viscerale aantasting of zeer uitgebreid chemotherapie (na biopsie) Zo enkele letsels, niet bedreigend: enkel start ART Soms IRIS, gevolgd door afvlakken letsels
 Zo enkele letsels, niet bedreigend: enkel start ART. Soms IRIS, gevolgd door afvlakken letsels.")
51
Hepatitis B en C Geen “klassieke” opportunistische inf.
Overdracht: SOA en bloedcontact Chroniciteit: verwikkelingen Cirrhose Hepatocellulair carcinoma Belangrijke oorzaak van mortaliteit geworden sedert ART

52
Hepatitis B en C Behandelbaar:
B: nucleosiden (3TC, TDF, entecavir, adefovir) C: peg-interferon plus ribavirine Steeds screenen naar hepatitis co-infectie Vaccinatie voor B (en A), niet mogelijk voor C
 C: peg-interferon plus ribavirine. Steeds screenen naar hepatitis co-infectie. Vaccinatie voor B (en A), niet mogelijk voor C.")
53
Online beschikbare bronnen
en Knowledge Base of .pdf in MMWR 17 dec 2004

Verwante presentaties








>")






>")




