Download de presentatie
De presentatie wordt gedownload. Even geduld aub

1
Neuropathische pijn bij Syringomyelie
David Kopsky, arts Behandelcentrum voor Neuropathische Pijn

2
Inleiding Anatomie Neuropathische pijn Behandelingen

3
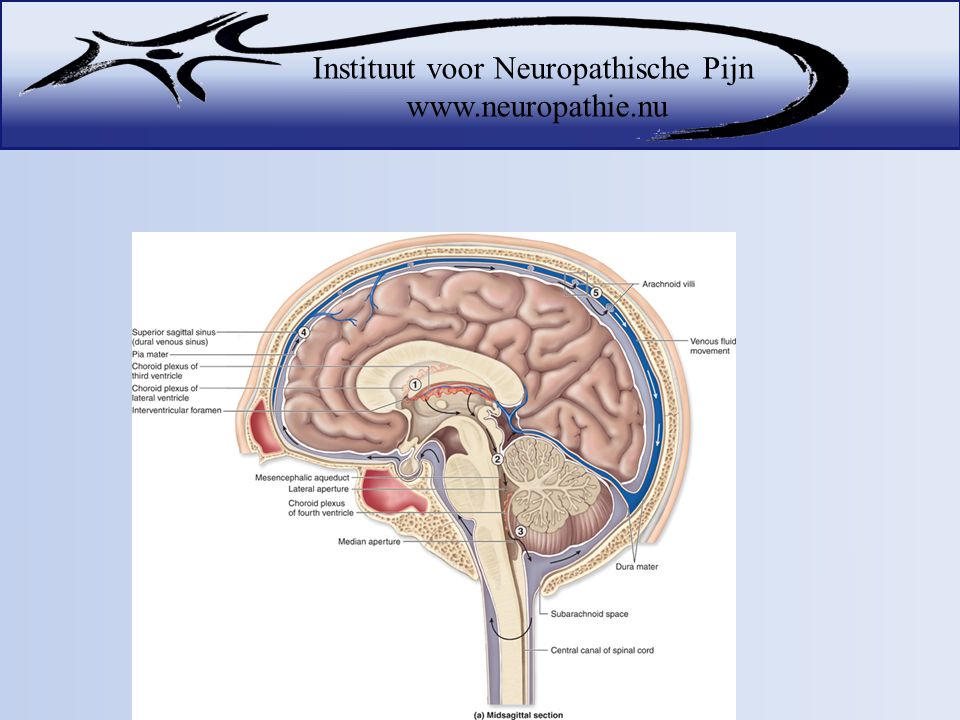
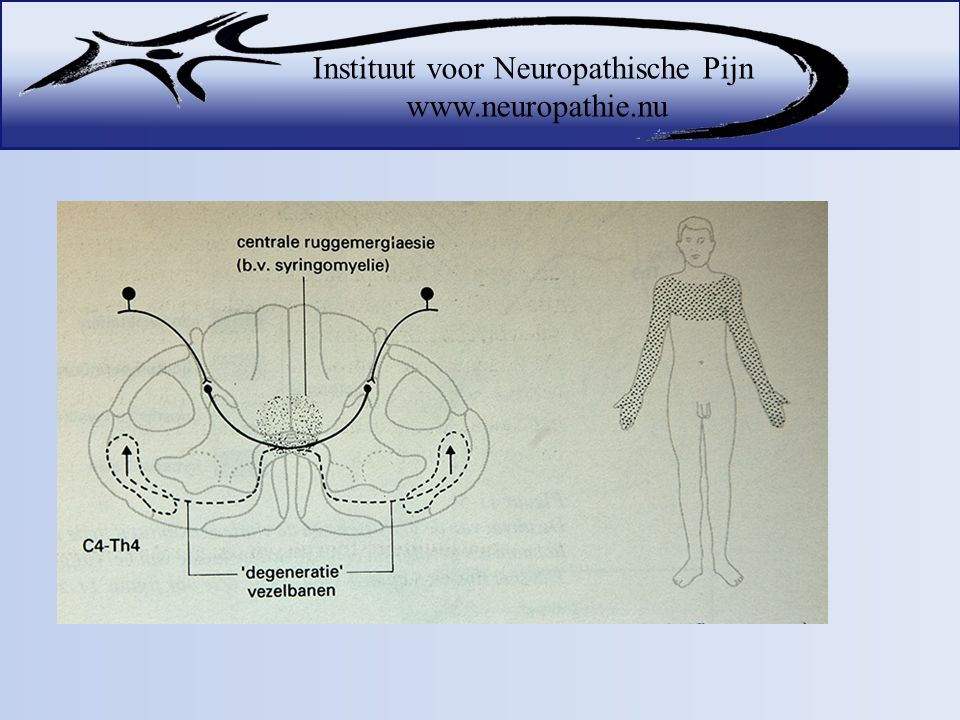
Inleiding Syringomyelie is verwijding van het centrale kanaal in het ruggenmerg

6
90% syringomyeliepatiënten is geassocieerd met Chiari malformatie
Chiari type 0 malformation: characterized by an alteration in Cerebro Spinal Fluid (CSF) hydrodynamics at the level of the foramen magnum. Patients with this subtype have syringomyelia either without tonsil herniation or with only mild tonsil herniation-associated findings. Chiari type I malformation: caudal herniation of the cerebellar tonsils exceeding 5 mm below the foramen magnum. This malformation is typically associated with hydrosyringomyelia. It is not usually accompanied by descent of the brain stem or IV ventricle, nor associated with the presence of hydrocephalus. Chiari type II malformation: caudal herniation of the cerebellar vermis, brain stem, and IV ventricle through the foramen magnum. It is associated with myelomeningocele, hydrocephalus, and, less frequently, hydrosyringomyelia. Other types of intracranial defects (hypoplastic tentorium cerebelli, cranial lacunae, anomalies of the Sylvius aqueduct) may exist. Chiari type III malformation: consists of occipital encephalocoele, with some of the intracranial defects associated with Chiari II malformation. Chiari type IV malformation: cerebellar aplasia or hypoplasia, associated with aplasia of the tentorium cerebelli. made by Chiari in 1891. Fernández AA, et al. Malformations of the craniocervical junction (Chiari type I and syringomyelia: classification, diagnosis and treatment). BMC Musculoskelet Disord. 2009
 hydrodynamics at the level. of the foramen magnum. Patients with this subtype have. syringomyelia either without tonsil herniation or with. only mild tonsil herniation-associated findings. Chiari type I malformation: caudal herniation of the cerebellar. tonsils exceeding 5 mm below the foramen magnum. This malformation is typically associated with. hydrosyringomyelia. It is not usually accompanied by. descent of the brain stem or IV ventricle, nor associated. with the presence of hydrocephalus. Chiari type II malformation: caudal herniation of the cerebellar. vermis, brain stem, and IV ventricle through the. foramen magnum. It is associated with myelomeningocele, hydrocephalus, and, less frequently, hydrosyringomyelia. Other types of intracranial defects (hypoplastic. tentorium cerebelli, cranial lacunae, anomalies of the Sylvius. aqueduct) may exist. Chiari type III malformation: consists of occipital encephalocoele, with some of the intracranial defects associated. with Chiari II malformation. Chiari type IV malformation: cerebellar aplasia or hypoplasia, associated with aplasia of the tentorium cerebelli. made by Chiari in Fernández AA, et al. Malformations of the craniocervical junction (Chiari type I and syringomyelia: classification, diagnosis and treatment). BMC Musculoskelet Disord")
7
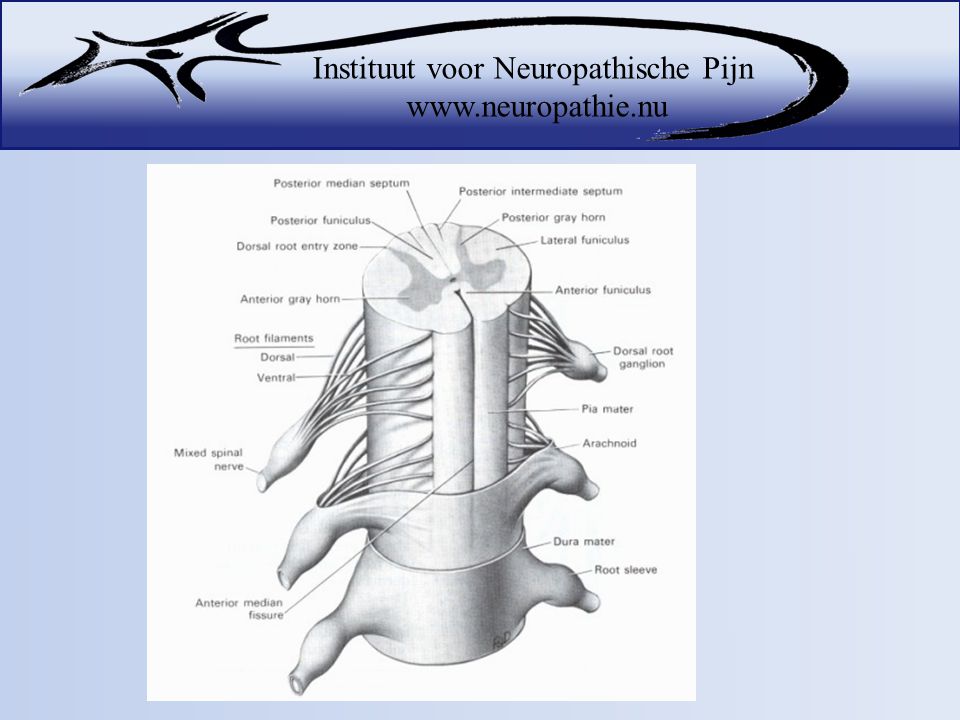
Anatomie van de zenuwen

10
Verschillende soorten zenuwen
A-alpha nerve fibers carry information related to proprioception (muscle sense). A-beta nerve fibers carry information related to touch. A-delta nerve fibers carry information related to pain and temperature. C-nerve fibers carry information related to pain, temperature and itch.
. A-beta nerve fibers carry information related to touch. A-delta nerve fibers carry information related to pain and temperature. C-nerve fibers carry information related to pain, temperature and itch.")
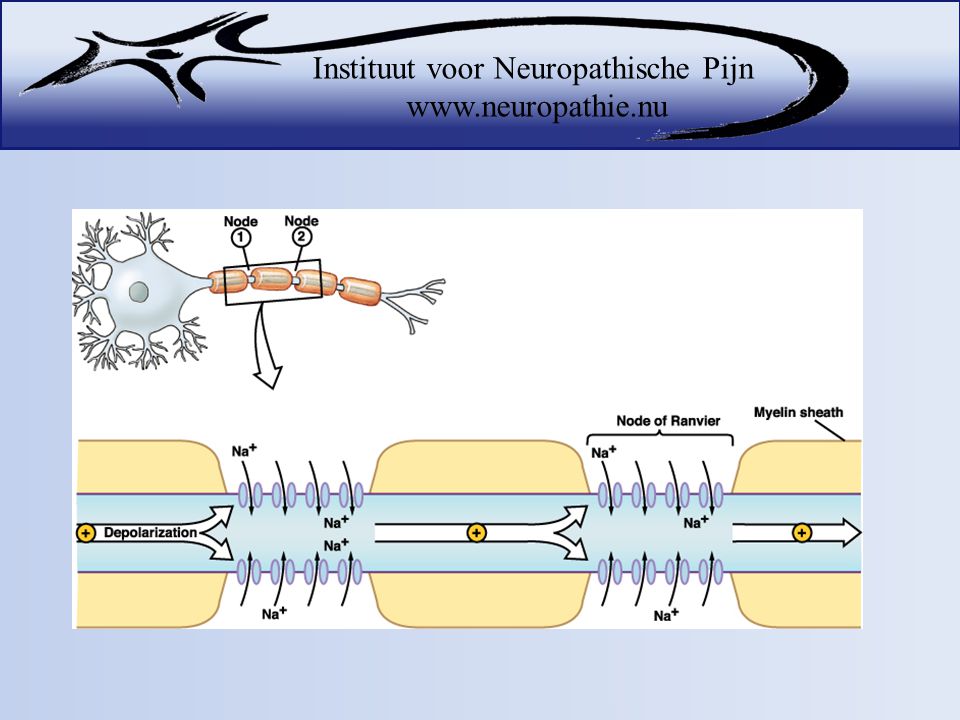
11
Snelheid van zenuwen A-alpha nerve fibers carry information related to proprioception (muscle sense). A-beta nerve fibers carry information related to touch. A-delta nerve fibers carry information related to pain and temperature. C-nerve fibers carry information related to pain, temperature and itch.

12
Schakeling op een andere zenuw

13
Verloop pijnprikkel

14
Verloop van pijnprikkel

17
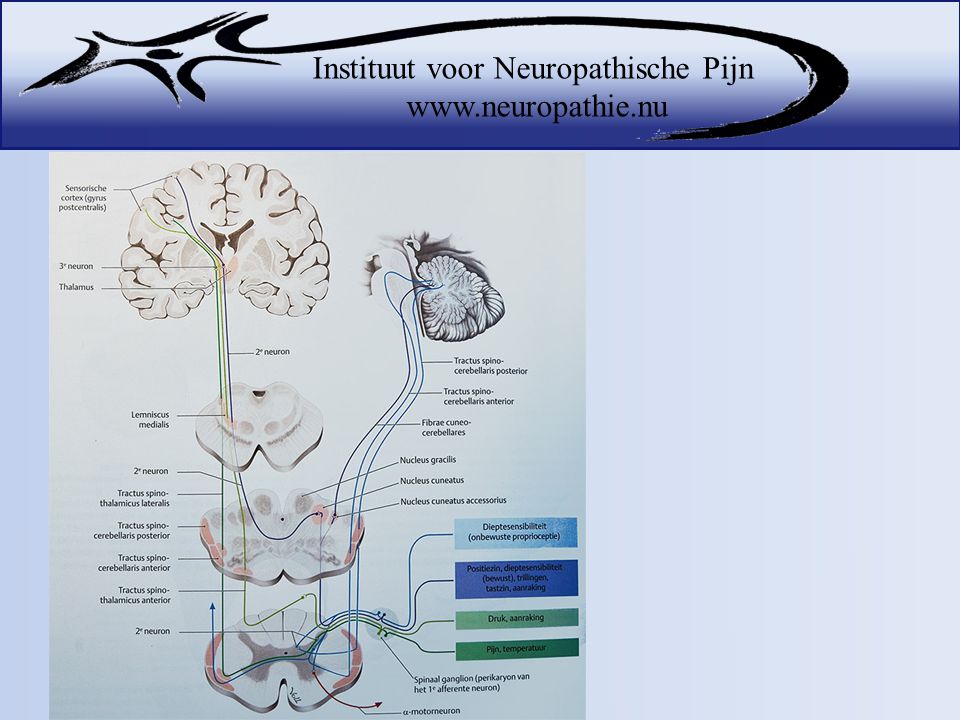
Propriocepsis (spier- en peesreceptoren)
Gracilis & Cuteanus Fijne tast Aanraking Propriocepsis (spier- en peesreceptoren) Tot Th3 bestaat cuneatus, daarna alleen gracilis. 1ste neuron stijgt zonder te kruisen naar de medulla oblongata naar de kernen N. gracilis en N. cuneatus. Vandaar kruist 2de neuron.
 Tot Th3 bestaat cuneatus, daarna alleen gracilis. 1ste neuron stijgt zonder te kruisen naar de medulla oblongata naar de kernen N. gracilis en N. cuneatus. Vandaar kruist 2de neuron.")
18
TST Anterior: Grove tast Aanraking TST Lateralis: Pijn Temperatuur
Tractus spinothalamicus ANTERIOR: grove tast- en aanrakingsprikkels (15 segm naar boven en 2 segm naar beneden, dan overschakelen en dan kruisen.) rondom haarfolicels Tractus spinothalamicus LATERALIS: pijn en temperatuurszin (directe segmentale oversteek van 2de neuron.) vrije zenuwuiteinden. Achterstrengbanen: Fasciculus Gracilis: fijne tast en aanrakingsprikkels (vater-pachinilichaampjes) en spier en peesreceptoren Fasciculus cuneatus: fijne tast en aanrakingsprikkels (vater-pachinilichaampjes) en spier en peesreceptoren
 rondom haarfolicels. Tractus spinothalamicus LATERALIS: pijn en temperatuurszin (directe segmentale oversteek van 2de neuron.) vrije zenuwuiteinden. Achterstrengbanen: Fasciculus Gracilis: fijne tast en aanrakingsprikkels (vater-pachinilichaampjes) en spier en peesreceptoren. Fasciculus cuneatus: fijne tast en aanrakingsprikkels (vater-pachinilichaampjes) en spier en peesreceptoren.")
20
Wat is neuropathische pijn?
Pijn door beschadiging van de zenuwen

21
Diagnose stellen van Neuropathische pijn
Leeds Assessment of Neuropathic Symptoms and Signs (LANSS) Neuropathic PainQuestionnaire (NPQ) painDETECT ID-Pain Douleur Neuropathique en 4 questions (DN4)
 Neuropathic PainQuestionnaire (NPQ) painDETECT. ID-Pain. Douleur Neuropathique en 4 questions (DN4)")
22
DN-4 Gaat de pijn gepaard met de volgende symptomen in hetzelfde gebied? Branderig JA NEE Pijnlijk koude gevoel Elektrische schokken Heeft de pijn één of meer van de volgende kenmerken Tintelingen JA NEE Prikken JA NEE Doof gevoel Jeuk

23
Ja ≥ 4 neuropathische pijn
Is er in het pijgebied een verminderd gevoel bij Aanraking JA NEE Prikken (cocktailprikker) Wordt de pijn verergerd door Wrijven JA NEE Ja ≥ 4 neuropathische pijn
 Wordt de pijn verergerd door. Wrijven. JA NEE. Ja ≥ 4 neuropathische pijn.")
24
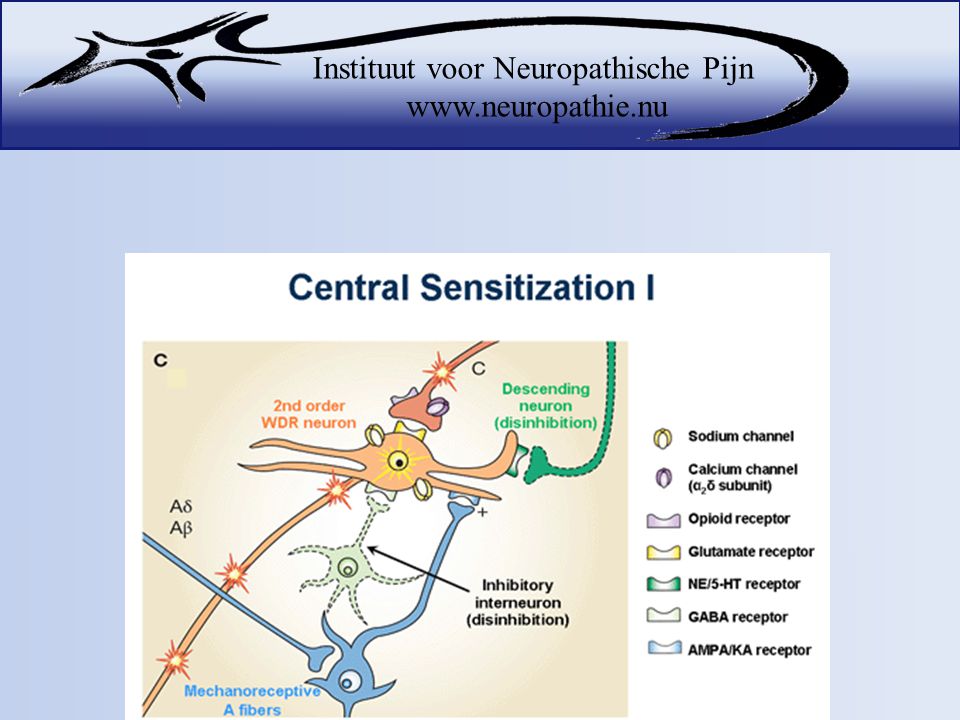
Centrale Neuropathische pijn
75% van syringomyeliepatiënten Klachten: overgevoeligheid voor pijnlijke prikkels (hyperalgesie) gevoeligheid voor niet-pijnlijke prikkels (allodynie) Branden, prikken, tintelen, doof gevoel, electrische schokken Type I: syringomyelia with obstruction of the foramen magnum and dilation of the central spinal canal: A) Associated to Chiari type I malformation. B) Associated with other obstructive lesions of the foramen magnum Type II: syringomyelia without obstruction of the foramen magnum, or idiopathic. Type III: syringomyelia with other diseases of the spinal cord. A) Spinal cord tumours (usually intraspinal) B) Traumatic myelopathy C) Spinal arachnoiditis and pachymeningitis D) Myelomalacia due to compression of the spinal cord (tumour, spondylosis) Neck pain is frequent and characterized by the absence of radicular distribution. It is associated to continuous, burning, deep-seated discomfort in the shoulders, nape, chest, and upper limbs. Neck pain usually increases with Valsalva manoeuvres. Prof. dr. K.C.P. Vissers Neuropathische pijn: een complexe pathologie Bijblijven 2006
 gevoeligheid voor niet-pijnlijke prikkels (allodynie) Branden, prikken, tintelen, doof gevoel, electrische schokken. Type I: syringomyelia with obstruction of the foramen. magnum and dilation of the central spinal canal: A) Associated. to Chiari type I malformation. B) Associated with. other obstructive lesions of the foramen magnum. Type II: syringomyelia without obstruction of the foramen. magnum, or idiopathic. Type III: syringomyelia with other diseases of the spinal. cord. A) Spinal cord tumours (usually intraspinal) B) Traumatic myelopathy C) Spinal arachnoiditis and pachymeningitis. D) Myelomalacia due to compression of the. spinal cord (tumour, spondylosis) Neck pain is frequent and characterized by the absence of. radicular distribution. It is associated to continuous, burning, deep-seated discomfort in the shoulders, nape, chest, and upper limbs. Neck pain usually increases with. Valsalva manoeuvres. Prof. dr. K.C.P. Vissers Neuropathische pijn: een complexe pathologie Bijblijven")
26
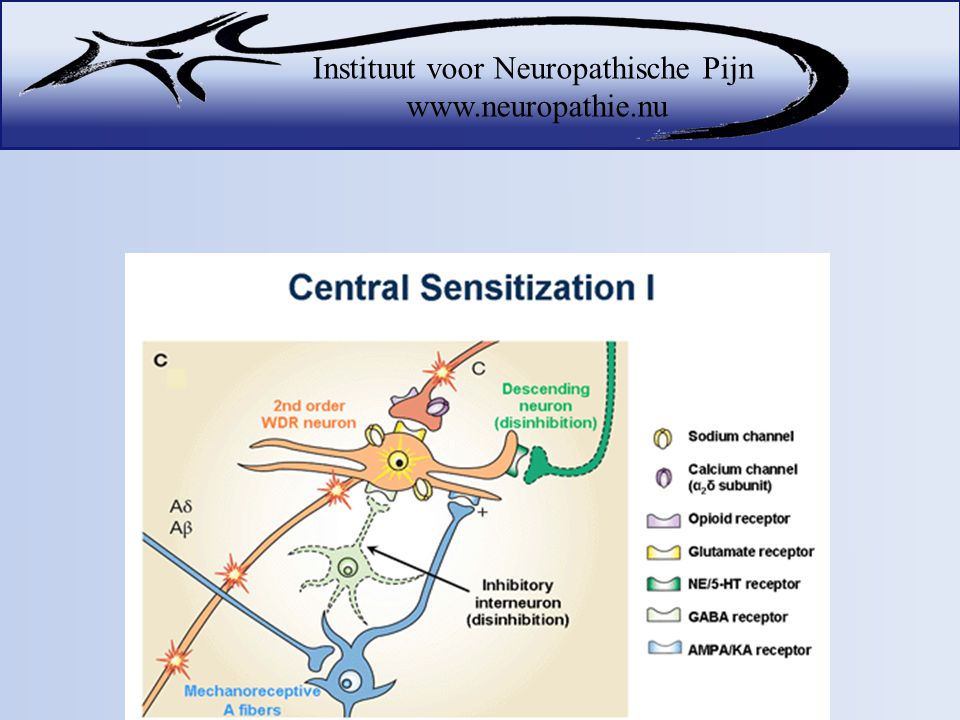
Zenuwstelsel op tilt A massive release of glutamate at the SCI lesion
epicenter triggers upregulation of the chemokine CCL21 both at the site of injury and in cell bodies of STT neurons whose axons have beenexposed to high concentrations of glutamate. CCL21 is then released at remote sites from the injury activating microglia, that contribute to neuronal hyperexcitability in the spinal cord dorsal horn and thalamus. Abnormal amplification and generation of nociceptive signals at these levels contributes to chronic pain after injury.

27
Behandeling Dempen van het zenuwstelsel met: Orale medicatie
Medicatie in crèmes Neuromodulatie (TENS, acupunctuur, SCS) Psychologische interventies Operatie
 Psychologische interventies. Operatie.")
28
Orale medicatie Gabapentine Pregabaline Amitriptyline Tramadol

30
1 medicijn vaak niet voldoende
In 30% van patiënten 50% verlichting met monotherapie Siddall PJ. Management of neuropathic pain following spinal cord injury: now and in the future. Spinal Cord. 2009;47:352-9.

31
Bijwerkingen

32
Bijwerkingen

33
Bijwerkingen

34
Cremes

35
Alleen 2 casus beschreven
Lidocaine 5% pleisters Wasner G, et al. A role for peripheral afferents in the pathophysiology and treatment of at-level neuropathic pain in spinal cord injury? A case report. Pain 2007. Hans GH et al. Treatment of an acute severe central neuropathic pain syndrome by topical application of lidocaine 5% patch: a case report. Spinal Cord

36
Neuromodulatie

37
Neuromodulatie: acupunctuur

38
4 studies bij centrale pijn: enigzins positieve effecten
Rapson LM et al. Acupuncture as a promising treatment for below-level central neuropathic pain: a retrospective study. J Spinal Cord Med 2003 Rapson LM et al. Acupuncture Treatment of Pain in SCI. J Spin Cord Med 1995. Wong JY et al. Acupuncture in the management of pain of musculoskeletal and neurologic origin. Phys Med Rehabil Clin N Am 1999. Nayak S et al. Is acupuncture effective in treating chronic pain after spinal cord injury? Arch Phys Med Rehabil 2001. Wen HL. Acute central cervical spinal cord syndrome treated by acupuncture and electrical stimulation (AES). Comp Med East West 1978.
. Comp Med East West")
39
Neuromodulatie: TENS

40
Neuromodulatie: SCS

41
Psychologische interventies
Cognitieve gedragstherapie Ondersteunend coachen Relaxatie Meditatie Biofeedback Hypnose Operant conditioning is based on the principles of reinforcement, with the emphasis on modifying responses to maladaptive behaviors and, in the case of chronic pain, behaviors that consist of overt expressions of pain, distress, and suffering………. These observable behaviors elicit responses from others and clinicians, responses that can serve to reinforce and thereby maintain the behaviors. Conversely, failure to positively reward the behaviors can extinguish them Cognitive-Behavioral Therapy Treatments based on operant conditioning within the CBT perspective do not focus on eliminating pain but rather on improving physical and emotional functioning despite pain. 37. Evans S, Fishman B, Spielman L, et al. Randomized trial of cognitive behavior therapy versus supportive psychotherapy for HIV-related peripheral neuropathic pain. Psychosomatics. 2003;44(1):44-50. 38. Jensen MP, Barber J, Romano JM, et al. A comparison of self-hypnosis versus progressive muscle relaxation in patients with multiple sclerosis and chronic pain. Int J Clin Exp Hypn. 2009;57(2): 39. Jensen MP, Hanley MA, Engel JM, et al. Hypnotic analgesia for chronic pain in persons with disabilities: a case series. Int J Clin Exp Hypn. 2005; 53(2): Turk DC et al. Assessment and treatment of psychosocial comorbidities in patients with neuropathic pain. Mayo Clin Proc
: Jensen MP, Barber J, Romano JM, et al. A comparison of self-hypnosis. versus progressive muscle relaxation in patients with multiple sclerosis and. chronic pain. Int J Clin Exp Hypn. 2009;57(2): Jensen MP, Hanley MA, Engel JM, et al. Hypnotic analgesia for chronic. pain in persons with disabilities: a case series. Int J Clin Exp Hypn. 2005; 53(2): Turk DC et al. Assessment and treatment of psychosocial comorbidities in patients with neuropathic pain. Mayo Clin Proc")
42
Operatie Operatie bij 25 patiënten: Bij 50% pijnvermindering
10% verergering van pijn Nakamura M et al Retrospective study of surgery-related outcomes in patients with syringomyelia associated with Chiari I malformation: clinical significance of changes in the size and localization of syrinx on pain relief. J Neurosurg 2004.

43
Nog weinig onderzoek gedaan naar centrale neuropathische pijn Elk individu is anders en reageert verschillend op een therapie Multimodale aanpak

44
The two enemies of human happiness are PAIN and BOREDOM
The two enemies of human happiness are PAIN and BOREDOM. Arthur Schopenhauer

Verwante presentaties