Download de presentatie
De presentatie wordt gedownload. Even geduld aub

1
Nieuwigheden in de Medische oncologie
Jeroen Mebis Medisch Oncoloog Limburgs Oncologisch Centrum Jessaziekenhuis Lommel 20/11/2010

2
19% Increase Projected U.S. Cancer Prevalence All Sites (2000 – 2015)
Het slechte nieuws 11.3 Million 9.5 Million 19% Increase

3
Geprojecteerde incidentie van kanker Limburg

4
Het goede nieuws

5
Traditioneel kanker concept (20e eeuw):
Cancer (or not) Genes Environment Diet Traditioneel kanker concept (20e eeuw):
 Genes. Environment. Diet. Traditioneel kanker concept. (20e eeuw):")
6
Huidig kanker concept:
Cancer (of not) Genes Environment factors Diet Huidig kanker concept:
 Genes. Environment factors. Diet. Huidig kanker concept:")
7
The Black Box

8
What’s new , Doc ?

10
850 anti-kanker molecules in ontwikkeling: 70% toename 2007-2010
FDA approvals sedert 2000 15 targeted therapies (Mabs and MIbS) 5 nieuwe chemotherapeutica 850 anti-kanker molecules in ontwikkeling: 70% toename
 5 nieuwe chemotherapeutica. 850 anti-kanker molecules in ontwikkeling: 70% toename")
11
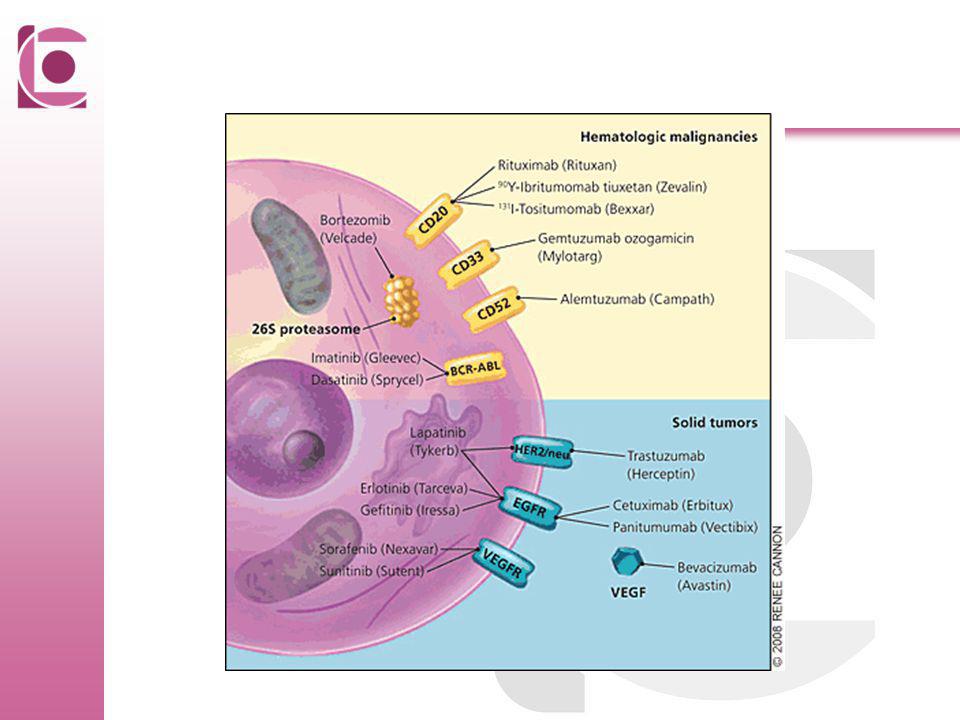
Table 1. Cancer Therapies That Target Oncogenic Proteins.
Croce C. N Engl J Med 2008;358:

12
Volgende decades: Nieuwe concepten Gebaseerd op fundamentale research
Genetische research Betere inzichten in tumorbiologie en tumor-immunologie Tumorcontrole ipv destructie Direct designer molecules

13
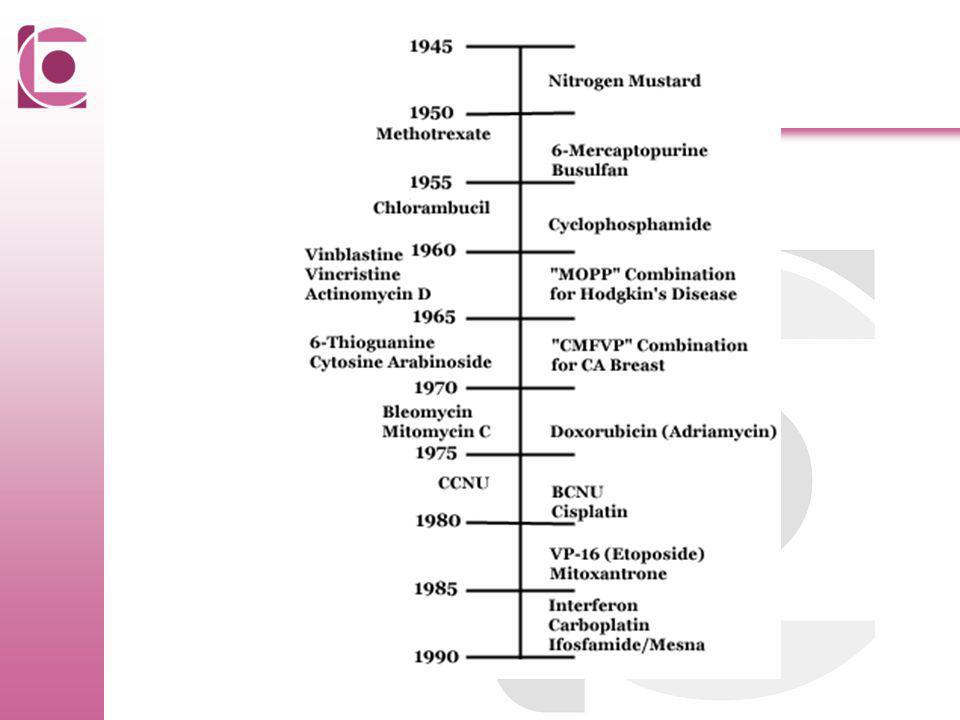
Oude molecules in nieuw kleedje
Liposomale doxorubicine en daunorubicine : Caelyx (TLC D-99) Daunoxome Minder lever clearance, langer half-leven, hogere AUC, hogere tumor concentratie Minder cardiale - en hematotoxiteit Minder GI- en haartoxiciteit Andere toxiciteit : hand-voet syndroom Zelfde efficiëntie
 Daunoxome. Minder lever clearance, langer half-leven, hogere AUC, hogere tumor concentratie. Minder cardiale - en hematotoxiteit. Minder GI- en haartoxiciteit. Andere toxiciteit : hand-voet syndroom. Zelfde efficiëntie.")
14
Nieuwe molecules Eribulin: synthetisch analoog van HalichondrinB
Nab-paclitaxel Cabazitaxel Ixabepilone Trabectedin

15
Wat is Targeted Therapie?
A “smart” bomb versus a “cluster” bomb. Dr. Nevin Murray

16
klassieke chemotherapie vs doelgerichte kankertherapiën
Klassieke chemotherapeutica → cytotoxisch effect op alle snelprolifererende cellen in het lichaam niet enkel selectief op maligne cellen, effect ook op gezonde sneldelende cellen (haarfollikels, darmepitheel, hematopoëtische cellen …) → belangrijke hematologische en niet-hematologische bijwerkingen bijwerkingen zijn limiterende factor bij de behandeling met chemotherapie van kankerpatiënten. doelgerichte kankertherapiën (“targeted therapy”): door hoog selectieve farmacologische manipulatie worden intracellulaire signaaltransductiewegen met een belangrijke rol spelen in de celproliferatie, migratie, differentiatie, maturatie, angiogenese en geprogrammeerde celdood, therapeutisch beïnvloed. DeVita VT et al: Cancer: Principles and practice of Oncology. 7th edition, 2004 Kay P Sem Oncol Nurs 2006;22(1):1-4
 → belangrijke hematologische en niet-hematologische bijwerkingen. bijwerkingen zijn limiterende factor bij de behandeling met chemotherapie van kankerpatiënten. doelgerichte kankertherapiën ( targeted therapy ): door hoog selectieve farmacologische manipulatie worden intracellulaire signaaltransductiewegen met een belangrijke rol spelen in de celproliferatie, migratie, differentiatie, maturatie, angiogenese en geprogrammeerde celdood, therapeutisch beïnvloed. DeVita VT et al: Cancer: Principles and practice of Oncology. 7th edition, Kay P Sem Oncol Nurs 2006;22(1):1-4.")
17
Targeted therapie “A form of treatment that is designed to specifically inhibit molecules that provide advantegeous growth signals to cancer cells.” (G. Sledge, JCO, 2005) Mogelijkheden Receptor tyrosine kinases VEGFR inhibitors EGFR inhibitors Endothelin receptors KIT BCR/ABL PDGFR
 Mogelijkheden. Receptor tyrosine kinases. VEGFR inhibitors. EGFR inhibitors. Endothelin receptors. KIT. BCR/ABL. PDGFR.")
18
Transcriptie factoren
Groei factoren VEGF Oestrogeen Androgeen Transcriptie factoren

20
Human Epidermal Growth Factor Receptor Family
No specific ligands - often acts as dimer partner NRG2 NRG3 Heregulins β-cellulin EGF, TGFa , b Cellulin Amphiregulin, HB-EGF Heregulins TK TK TK erbB1 HER1 EGFR erbB2 HER2 neu erbB3 HER3 erbB4 HER4

21
Cell Cycle Progression
EGFR Function in Normal Cell TK TK ATP ATP + Gene Transcription Cell Cycle Progression Antiapoptosis Cell Proliferation Angiogenesis

22
EGFR signal transduction in tumour cells
TK TK PI3-K GRB2 pY pY SOS pY STAT3 RAS RAF PTEN AKT MEK Gene transcription MAPK G1 M S Proliferation/ maturation Survival (anti-apoptosis) G2 Chemotherapy / radiotherapy resistance Metastasis Angiogenesis
 G2. Chemotherapy / radiotherapy resistance. Metastasis. Angiogenesis.")
23
- - - - Strategies to inhibit EGFR signaling Anti-ligand mAbs
EGFR tyrosine kinase inhibitors Bispecific Abs Immune effector cell Anti-EGFR mAbs TK TK TK TK ATP - - - -

24
Her-2/neu: amplificatie en overexpressie bij borstkanker
Detectiemethode Controle gen Fluorescentie in situ hybridizatie (FISH) DNA-probe Her-2/neu gen Immuunhistochemie gemerkt antilichaam
 DNA-probe. Her-2/neu gen. Immuunhistochemie. gemerkt antilichaam.")
25
IHC FISH negatief 1+ 2+ 3+ medium

26
Her-2/neu en borstkanker
amplificatie in 25-30% sterke associatie met: lage differentiatiegraad afwezigheid van hormoonreceptorexpressie DNA aneuploidie / snelle delingsactiviteit sterke correlatie met: ziekterecidief uitzaaiingen korte overleving = kenmerk van agressiviteit!

27
Overlevingscurve voor de voorspelling van ziekte-gebonden
sterfte bij pTxN0 borstkanker t.g.v. amplificatie van Her-2/neu

28
Interactie tussen trastuzumab en HER2

29
Trastuzumab: gehumanizeerd muize-antilichaam
Werking = cytostatisch: minder groei door receptorblokkade = cytotoxisch: - activatie Ab-Ag cellulaire cytotoxiciteit - potentiëring van chemotherapie

30
Overleving zonder ziekteprogressie +/- Herceptine bij
gemetastaseerde patiënten (2001) Sterfte na 1j: 22% vs 33%
 Sterfte na 1j: 22% vs 33%")
31
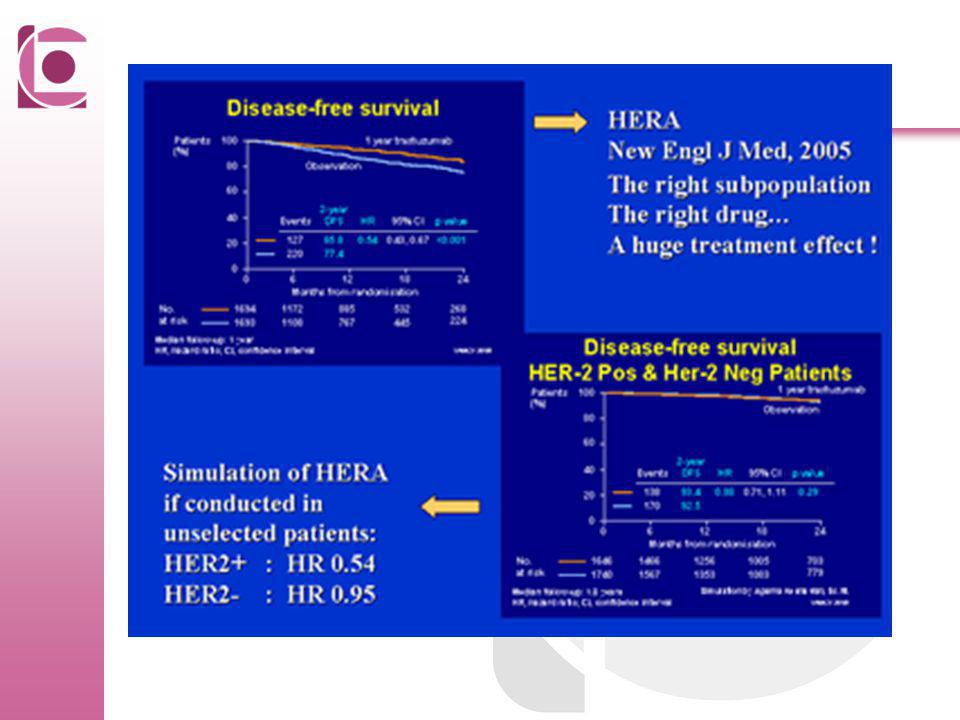
Months from randomization
DFS: HERA Trial Trastuzumab 1 yr % alive and disease free 100 90 80 70 Observation 60 50 2-yr DFS % 40 Events HR [95% CI] p value 30 20 127 85.8 0.54 [0.43, 0.67] <0.0001 The HERA trial like the B31 and N9831 trials showed a striking improvement in DFS, reducing the risk of relapse and mortality events by about 50%. This result is statistically significant. The difference in outcome is also large in absolute terms with about an 8% advantage at 2 years of follow-up. This result is more positive than the sequential chemotherapy trastuzumab arm of N9831. The reason for this difference in results is unclear. 10 220 77.4 5 10 15 20 25 No. at risk Months from randomization 1694 1472 1067 629 303 102 1693 1428 994 580 280 87

32
Herceptine mét chemotherapie (3350ptn)
Ziektevrije overleving Totale overleving + 12% na 3j. + 2.5% na 3j.

34
New drugs targeting HER2 or alternative pathways
Bevacizumab Ertumaxomab Pertuzumab VEGF Trastuzumab ErbB3 ErbB2 IGF-IR ErbB2 VEGFR ErbB1 PDGFR Vascular endothelial cell membrane Pazopanib Sunitinib Let’s now look in more detail at Tyverb, which is the first oral, small molecule, dual targeted agent that acts intracellularly and is licensed in ErbB2-positive breast cancer. Lapatinib PI3K Tanespimycin Alvespimycin Akt HSP90 HDAC Vorinostat Panobinostat mTOR Temsirolimus Everolimus HDAC=histone deacetylase

35
EGFR expression in human tumors
Type of tumor Tumors with EGFR expression Head and neck 90–100% Colon 75–89% Pancreas Up to 95% Breast Up to 91% Renal Up to 90% NSCLC Up to 80% Ovary Up to 77% Bladder Up to 72% Glioma Up to 63% Head and neck Lung (NSCLC) Colorectal EGFR expression is also linked to reduced response, a poorer outcome, and/or increased resistance to chemotherapy and RT 05/2008 P/ERB/002/ slidekit mode of action version of May 2008
 Colorectal. EGFR expression is also linked to reduced response, a poorer outcome, and/or increased resistance to chemotherapy and RT. 05/2008 P/ERB/002/ slidekit mode of action version of May")
36
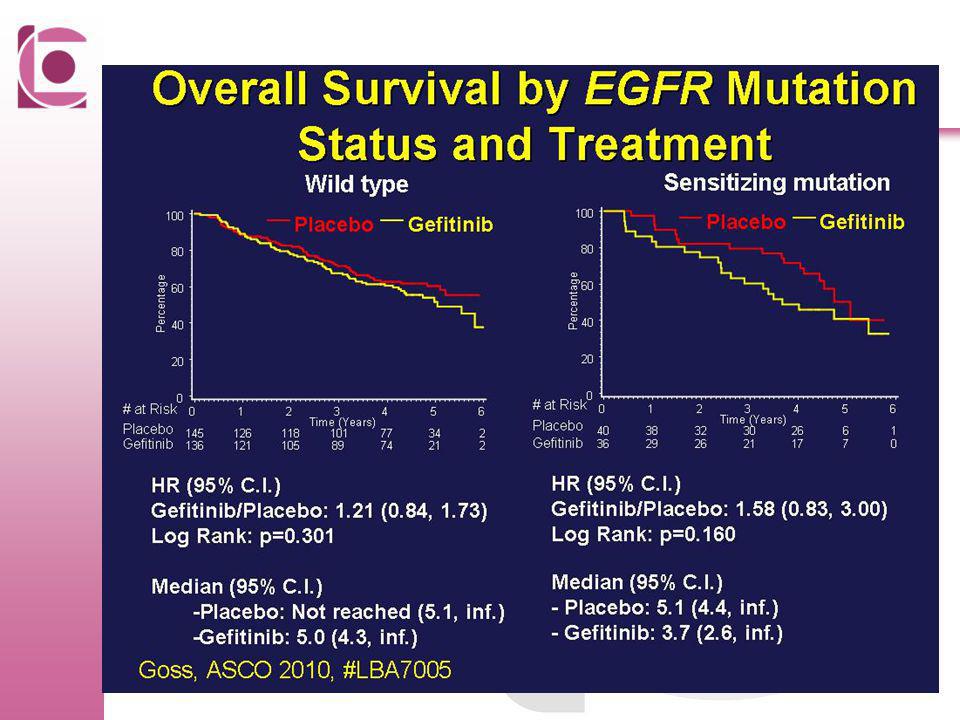
EGFR inhibitie en erlotinib in long kanker
Erlotinib inhibeert phosphorylatie van EGFR en blokkeert downstream signaling Screening for EGFR mutations jn lung cancer EGFR mutations: RR 70.6%; OS 27 months

37
Pivotal trial BR.21: survival
Tarceva significantly prolongs overall survival1,2 1.SmPC Tarceva®, Tarceva® (erlotinib) full prescribing information, OSI Pharmaceuticals, Inc., 2005
 full prescribing information, OSI Pharmaceuticals, Inc.,")
39
The angiogenic switch in tumour development
Larger tumour vascular metastatic potential Small tumour (1–2mm diameter) avascular dormant Angiogenic switch Results in overexpression of pro-angiogenic signals, such as VEGF It is generally accepted that no solid tumour can grow beyond a critical size of 1–2mm in diameter, or about 106 cells, without an adequate vascular supply. The ‘angiogenic switch’ is reviewed in Bergers et al.1 Tumour-associated angiogenesis can be thought to go through two phases, which are separated by the ‘angiogenic switch’. The first is an ‘avascular’ phase, in which tumours are not more than 1–2mm in diameter. These tumours remain dormant, as they are in a steady state between cell proliferation and apoptosis. Some of these small tumours will switch to the second – vascular – phase, in which the tumour grows exponentially. A classic model of the angiogenic switch is that of a pair of scales laden with pro-angiogenic molecules on one side and anti-angiogenic molecules on the other side. An imbalance of these pro- and anti-angiogenic factors triggers the ‘switch’. The onset of angiogenesis or the ‘angiogenic switch’ is a discrete step that can occur at any stage of tumour progression, dependent upon the type of tumour and its micro-environment. Induction of the ‘switch’ is dependent upon the balance tipping in favour of the pro-angiogenic molecules. Bergers G, Benjamin LE. Tumorigenesis and the angiogenic switch. Nat Rev Cancer 2003;3:401–10. Adapted from Bergers G, et al. Nat Rev Cancer 2002;3:401–10
 avascular. dormant. Angiogenic switch. Results in overexpression of pro-angiogenic signals, such as VEGF. It is generally accepted that no solid tumour can grow beyond a critical size of 1–2mm in diameter, or about 106 cells, without an adequate vascular supply. The ‘angiogenic switch’ is reviewed in Bergers et al.1. Tumour-associated angiogenesis can be thought to go through two phases, which are separated by the ‘angiogenic switch’. The first is an ‘avascular’ phase, in which tumours are not more than 1–2mm in diameter. These tumours remain dormant, as they are in a steady state between cell proliferation and apoptosis. Some of these small tumours will switch to the second – vascular – phase, in which the tumour grows exponentially. A classic model of the angiogenic switch is that of a pair of scales laden with pro-angiogenic molecules on one side and anti-angiogenic molecules on the other side. An imbalance of these pro- and anti-angiogenic factors triggers the ‘switch’. The onset of angiogenesis or the ‘angiogenic switch’ is a discrete step that can occur at any stage of tumour progression, dependent upon the type of tumour and its micro-environment. Induction of the ‘switch’ is dependent upon the balance tipping in favour of the pro-angiogenic molecules. Bergers G, Benjamin LE. Tumorigenesis and the angiogenic switch. Nat Rev Cancer 2003;3:401–10. Adapted from Bergers G, et al. Nat Rev Cancer 2002;3:401–10.")
40
What is VEGF? Key mediator of angiogenesis
Stimulates growth of endothelial cells Also known as VEGF-A Related molecules are VEGF-B, C and D, placental growth factor (PlGF) Homodimeric glycoprotein Molecular weight: 45,000Da Binds VEGF receptor-2 and heparin Four molecular species VEGF121 VEGF165* VEGF189 VEGF206 Native VEGF (or VEGF-A) is a basic, heparin-binding, homodimeric glycoprotein of 45,000Da.1 This means that it is made up of two identical units. Differential expression of the human VEGF gene results in the generation of four different molecular species having 121, 165, 189 and 206 amino acids, respectively. VEGF165 is the predominant molecular species produced by a variety of normal and transformed cells. VEGF is a potent mitogen for vascular endothelial cells derived from arteries, veins and lymphatics, but has no mitogenic activity for other cell types. Ferrara N, Davis-Smyth T. The biology of vascular endothelial growth factor. Endocr Rev 1997;18:4–25. *Predominant molecular species Ferrara N, et al. Endocr Rev 1997;18:4–25
 Homodimeric glycoprotein. Molecular weight: 45,000Da. Binds VEGF receptor-2 and heparin. Four molecular species. VEGF121. VEGF165* VEGF189. VEGF206. Native VEGF (or VEGF-A) is a basic, heparin-binding, homodimeric glycoprotein of 45,000Da.1 This means that it is made up of two identical units. Differential expression of the human VEGF gene results in the generation of four different molecular species having 121, 165, 189 and 206 amino acids, respectively. VEGF165 is the predominant molecular species produced by a variety of normal and transformed cells. VEGF is a potent mitogen for vascular endothelial cells derived from arteries, veins and lymphatics, but has no mitogenic activity for other cell types. Ferrara N, Davis-Smyth T. The biology of vascular endothelial growth factor. Endocr Rev 1997;18:4–25. *Predominant molecular species. Ferrara N, et al. Endocr Rev 1997;18:4–25.")
41
The VEGF family and its receptors
VEGF-A VEGF-B PlGF VEGF-A VEGF-C VEGF-D VEGF receptor-2 VEGF receptor-1 VEGF receptor-3 P– – P – P P– – P P– P– – P P– – P P– – P Several molecules have been identified that are structurally related to VEGF: VEGF-B, VEGF-C, VEGF-D, VEGF-E and PlGF. This structural similarity suggests that they also may play a role in angiogenesis regulation.1,2 The VEGF ligands bind to several VEGF receptors comprising seven immunoglobulin (Ig)-like domains in the extracellular domain (ECD). VEGF binds to VEGF receptor-1 (also called Flt-1) and VEGF receptor-2 (also called Flk-1 or KDR) to modulate angiogenesis and maintain immature vasculature. Mature vasculature does not require VEGF or other growth factors for survival.1 PlGF and VEGF-B bind primarily to VEGF receptor-1. PlGF modulates angiogenesis and may also play a role in the inflammatory response.1 VEGF-C and VEGF-D bind primarily to VEGF receptor-3 and stimulate lymphangiogenesis (growth of new lymphatic vessels) rather than angiogenesis.2 VEGF regulates haematopoiesis in the bone marrow independently of neo-angiogenesis. VEGF is thought to control haematopoietic stem cell survival and repopulation by means of an internal autocrine loop.3 Mouse studies suggest that although VEGF receptor-2 is essential for development of haematopoietic stem cells during embryonic development, it may be redundant for haematopoietic stem cells in adulthood. Studies in mice also show that VEGF receptor-1 has a role in haematopoietic stem cell survival during haematopoietic repopulation in adults.3 Ferrara N, Davis-Smyth T. The biology of vascular endothelial growth factor. Endocr Rev 1997;18:4–25. Griffioen AW, Molema G. Angiogenesis: potentials for pharmacologic intervention in the treatment of cancer, cardiovascular diseases, and chronic inflammation. Pharmacol Rev 2000;52:237–68. Gerber H-P, Ferrara N. The role of VEGF in normal and neoplastic hematopoiesis. J Mol Med 2003;81:20–31. Migration, permeability, DNA synthesis, survival Angiogenesis Lymphangiogenesis Adapted from Ferrara N. Nat Med 2003;9:669–76
-like domains in the extracellular domain (ECD). VEGF binds to VEGF receptor-1 (also called Flt-1) and VEGF receptor-2 (also called Flk-1 or KDR) to modulate angiogenesis and maintain immature vasculature. Mature vasculature does not require VEGF or other growth factors for survival.1. PlGF and VEGF-B bind primarily to VEGF receptor-1. PlGF modulates angiogenesis and may also play a role in the inflammatory response.1 VEGF-C and VEGF-D bind primarily to VEGF receptor-3 and stimulate lymphangiogenesis (growth of new lymphatic vessels) rather than angiogenesis.2. VEGF regulates haematopoiesis in the bone marrow independently of neo-angiogenesis. VEGF is thought to control haematopoietic stem cell survival and repopulation by means of an internal autocrine loop.3 Mouse studies suggest that although VEGF receptor-2 is essential for development of haematopoietic stem cells during embryonic development, it may be redundant for haematopoietic stem cells in adulthood. Studies in mice also show that VEGF receptor-1 has a role in haematopoietic stem cell survival during haematopoietic repopulation in adults.3. Ferrara N, Davis-Smyth T. The biology of vascular endothelial growth factor. Endocr Rev 1997;18:4–25. Griffioen AW, Molema G. Angiogenesis: potentials for pharmacologic intervention in the treatment of cancer, cardiovascular diseases, and chronic inflammation. Pharmacol Rev 2000;52:237–68. Gerber H-P, Ferrara N. The role of VEGF in normal and neoplastic hematopoiesis. J Mol Med 2003;81:20–31. Migration, permeability, DNA synthesis, survival. Angiogenesis. Lymphangiogenesis. Adapted from Ferrara N. Nat Med 2003;9:669–76.")
42
Agents targeting the VEGF pathway
Antibodies inhibiting VEGF receptors Soluble VEGF receptors (VEGF-TRAP) Antibodies inhibiting VEGF (e.g. AvastinTM) Permeability VEGF Cation channel VEGF receptor-2 Small-molecules inhibiting VEGF receptors (TKIs) (e.g. PTK-787) P– – P – P P– – P P– – P P– P– Overexpression of VEGF by tumour cells can be targeted by antibodies against VEGF antibodies against VEGF receptors soluble VEGF receptors that bind circulating VEGF small molecule inhibitors of VEGF receptors catalytic RNA molecules (ribozymes), which cleave VEGF receptor mRNA. P– – P – P Migration, permeability, DNA synthesis, survival Ribozymes (Angiozyme) Angiogenesis Lymphangiogenesis
 Antibodies inhibiting VEGF (e.g. AvastinTM) Permeability. VEGF. Cation channel. VEGF receptor-2. Small-molecules inhibiting VEGF receptors (TKIs) (e.g. PTK-787) P– – P. – P. P– – P. P– – P. P– P– Overexpression of VEGF by tumour cells can be targeted by. antibodies against VEGF. antibodies against VEGF receptors. soluble VEGF receptors that bind circulating VEGF. small molecule inhibitors of VEGF receptors. catalytic RNA molecules (ribozymes), which cleave VEGF receptor mRNA. P– – P. – P. Migration, permeability, DNA synthesis, survival. Ribozymes. (Angiozyme) Angiogenesis. Lymphangiogenesis.")
44
The other side Resistentie Selectiviteit
Eg: trastuzumab: dual EGFR and Her2 inhibition: lapatinib/Pertuzumab Downstream mTor inhibitie? Selectiviteit Cardiale toxiciteit Huid toxiciteit

45
Sunitinib-geïnduceerde hypothyreoïdie
Prospective analysis of 59 GIST and RCC patients treated with Sunitinib Cohort RCC (n = 42) GIST (n = 17) RCC + GIST (n = 59) No biochemical thyroid abnormalities, n (%) 11 (26) 9 (53) 20 (34) Median time to abnormal TSH, wks (range) 4 (2–22) 9 (4–46) 4 (2–46) At least one TSH (no treatment required), n (%) 14 (33) 6 (35) (Sub)clinical hypothyroidism (treatment required), n (%) 2 (12) 16 (27) At least one TSH (no treatment required), n (%) 3 (7) 3 (5) (Sub)clinical hyperthyroidism (treatment required), n (%) TPOAb – positive patients 2a 0b 2 Wolter P et al submitted a TPOAb measurements available in 38 of 42 patients with RCC. b TPOAb measurements available in 11 of 17 patients with GIST.
 GIST. (n = 17) RCC + GIST. (n = 59) No biochemical thyroid abnormalities, n (%) 11 (26) 9 (53) 20 (34) Median time to abnormal TSH, wks (range) 4 (2–22) 9 (4–46) 4 (2–46) At least one TSH (no treatment required), n (%) 14 (33) 6 (35) (Sub)clinical hypothyroidism (treatment required), n (%) 2 (12) 16 (27) At least one TSH (no treatment required), n (%) 3 (7) 3 (5) (Sub)clinical hyperthyroidism (treatment required), n (%) TPOAb – positive patients. 2a. 0b. 2. Wolter P et al submitted. a TPOAb measurements available in 38 of 42 patients with RCC. b TPOAb measurements available in 11 of 17 patients with GIST.")
46
Verloop van TSH (mIU/l) in 4 RCC pts onder therapie met sunitinib
This figure gives you an overview about TSH levels in the total population of patients treated with Sunitinib over time of treatment. On the right side of the graph you can see that most of the patients treated with Sunitinib for a long period of time develop increased TSH levels, and in most cases very high levels. That means, the longer the treatment with Sunitinib, the higher the risk of developping thyroid dysfunction. But one the other hand you can see also in the left corner that some patients developped elevated TSH levels already very early in the course of treatment. Wolter P et al submitted

47
Ongewone bijwerkingen van targeted agents
Ernstige hypomagnesemie en hypocalcemie onder therapie met cetuximab en panitumumab (graad 3/4 in 4% resp. 6-17%) → monitoring noodzakelijk en substitutie zo nodig! hypofosfatemie onder therapie met dasatinib, nilotinib, sorafenib, sunitinib, imatinib. Temsirolimus geeft aanleiding tot hyperglycemie (ev. insuline of orale antidiabetische medicatie aanpassen!) en hyperlipidemie. Interstitieel longlijden wordt gerapporteerd onder cetuximab (0,3%), ook onder erlotinib (0,6%), dus voorzicht bij patiënten met voorgeschiedenis van longlijden. Pleuravochtuitstortingen worden onder dasatinib beschreven (22 %, graad 3/4 in 5%), waarschijnlijk kaderend in gegeneraliseerde oedemen (ook pericard vochtuitstorting, ascites, …) Toxicity: Hypophosphatemia Drug Incidence (%) all gr. 3/4 Bevacizumab n.s. 4,5 Sunitinib 9-36 5 Sorafenib 35-45 11-13 Imatinib 53 Dasatinib 6-20 Nilotinib 10 Temsirolimus 49 18 Tejpar S et al Lancet Oncol 2007; 8:387-94 Fitter S et al Blood 2008;111(5):
 → monitoring noodzakelijk en substitutie zo nodig! hypofosfatemie onder therapie met dasatinib, nilotinib, sorafenib, sunitinib, imatinib. Temsirolimus geeft aanleiding tot hyperglycemie (ev. insuline of orale antidiabetische medicatie aanpassen!) en hyperlipidemie. Interstitieel longlijden wordt gerapporteerd onder cetuximab (0,3%), ook onder erlotinib (0,6%), dus voorzicht bij patiënten met voorgeschiedenis van longlijden. Pleuravochtuitstortingen worden onder dasatinib beschreven (22 %, graad 3/4 in 5%), waarschijnlijk kaderend in gegeneraliseerde oedemen (ook pericard vochtuitstorting, ascites, …) Toxicity: Hypophosphatemia. Drug. Incidence (%) all gr. 3/4. Bevacizumab. n.s. 4,5. Sunitinib Sorafenib Imatinib. 53. Dasatinib Nilotinib. 10. Temsirolimus Tejpar S et al Lancet Oncol 2007; 8: Fitter S et al Blood 2008;111(5):")
48
Ongewone bijwerkingen van targeted agents
Hypertensie = meest belangrijke bijwerking van VEGFR-inhibitoren, meestal vroeg na starten van de therapie (~ 3 weken bij sunitinib / sorafenib) → monitoring absoluut noodzakelijk, ev opstarten antihypertensieve therapie, best met vasodilaterende antihypertensiva zoals ACE-inhibitoren ofwel calcium antagonisten. Proteinurie = bij % van patiënten onder bevacizumab, meestal asymptomatisch, follow-up van proteinurie zinvol (standaard dipstick, 24-uur urine analyse). “reversible posterior leukencephalopathy syndrome (RPLS)” onder VEGF-inhibitoren, vnl. bij patienten met hypertensie, oorzaak niet duidelijk (neuroprotectief effect van VEGF?) Oculaire afwijkingen (conjunctivitis, trichomegaly, …) in 15-30% van patiënten onder EGFR-inhibitoren Toxicity: Hypertension Drug Incidence (%) all gr. 3/4 Bevacizumab 23-67 8-18 Sunitinib 15-30 4-10 Sorafenib 9-17 3-4 Temsirolimus 7 - Eskens F et al EJC 2006;42: Basti S Cancer Nursing 2007;30(4S),S10-16 Glusker P et al NEJM 2006;354(9),980-1
 → monitoring absoluut noodzakelijk, ev opstarten antihypertensieve therapie, best met vasodilaterende antihypertensiva zoals ACE-inhibitoren ofwel calcium antagonisten. Proteinurie = bij % van patiënten onder bevacizumab, meestal asymptomatisch, follow-up van proteinurie zinvol (standaard dipstick, 24-uur urine analyse). reversible posterior leukencephalopathy syndrome (RPLS) onder VEGF-inhibitoren, vnl. bij patienten met hypertensie, oorzaak niet duidelijk (neuroprotectief effect van VEGF ) Oculaire afwijkingen (conjunctivitis, trichomegaly, …) in 15-30% van patiënten onder EGFR-inhibitoren. Toxicity: Hypertension. Drug. Incidence (%) all gr. 3/4. Bevacizumab Sunitinib Sorafenib Temsirolimus Eskens F et al EJC 2006;42: Basti S Cancer Nursing 2007;30(4S),S Glusker P et al NEJM 2006;354(9),")
49
Bloedingen en perforaties:
Verhoogd bloedingsrisico onder bevacizumab, kan gaan van epistaxis en subcutane bloedingen tot fatale longbloedingen bij patiënten met NSCLC (centraal gelegen, geëxcaveerde letsels). CAVE: patiënten met hersenmetastasen en onder volledige dosis anticoagulantia. Duidelijk vertraagde wondheling/post-operatieve problemen (10-20%) bij patiënten die majeure heelkunde moeten ondergaan onder therapie met bevacizumab → voor electieve heelkunde best minimum 28 dagen wachten. Bij SCLC patienten onder therapie met bevacizumab, chemotherapie en radiotherapie verhoogd risico op tracheo-esofagale fistels. Wordt ook gezien onder suntinib/sorafenib maar de halfwaardetijd voor –nibs is korter EGFR, m-TOR inhibition en wondheling? Half-life elimination Bevacizumab ~ 20 d (11-50) Sunitinib ~ h Sorafenib ~ h Imatinib ~ 18 h Dasatinib ~ 0,5 - 6 h Nilotinib ~ h Cetuximab ~4,5 d (2,5 -9) Panitumumab ~ 7,5 d (4-11) Erlotinib ~ h Trastuzumab ~ 6 d (w), ~ 16 d (3w) Lapatinib ~ 24 h Temsirolimus ~ 17 h Eskens F et al EJC 2006;42:
. CAVE: patiënten met hersenmetastasen en onder volledige dosis anticoagulantia. Duidelijk vertraagde wondheling/post-operatieve problemen (10-20%) bij patiënten die majeure heelkunde moeten ondergaan onder therapie met bevacizumab → voor electieve heelkunde best minimum 28 dagen wachten. Bij SCLC patienten onder therapie met bevacizumab, chemotherapie en radiotherapie verhoogd risico op tracheo-esofagale fistels. Wordt ook gezien onder suntinib/sorafenib maar de halfwaardetijd voor –nibs is korter. EGFR, m-TOR inhibition en wondheling Half-life elimination. Bevacizumab. ~ 20 d (11-50) Sunitinib. ~ h. Sorafenib. ~ h. Imatinib. ~ 18 h. Dasatinib. ~ 0,5 - 6 h. Nilotinib. ~ h. Cetuximab. ~4,5 d (2,5 -9) Panitumumab. ~ 7,5 d (4-11) Erlotinib. ~ h. Trastuzumab. ~ 6 d (w), ~ 16 d (3w) Lapatinib. ~ 24 h. Temsirolimus. ~ 17 h. Eskens F et al EJC 2006;42:")
50
Huidtoxiciteit Belangrijke bijwerking onder EGFR- en VEGFR-inhibitoren
Bij patienten onder erlotinib/cetuximab associatie tussen graad van de huidtoxiciteit en effectiviteit van de therapie. Huidrash meestal zeer vroeg in de behandeling (eerste 1-2 weken). Onder Sunitinib is een gele huidskleur en haardepigmentatie beschreven. Toxicity: Rash Drug Incidence (%) all gr. 3/4 Bevacizumab n.s. Sunitinib 14-27 2 Sorafenib 19-40 ≤ 1 Imatinib 21-26 3-5 Dasatinib 22 Nilotinib 28-33 Cetuximab 80 15 Panitumumab 90 16 Erlotinib 50-88 9 Trastuzumab 4-18 Lapatinib 28 Temsirolimus 47 4
. Onder Sunitinib is een gele huidskleur en haardepigmentatie beschreven. Toxicity: Rash. Drug. Incidence (%) all gr. 3/4. Bevacizumab. n.s. Sunitinib Sorafenib ≤ 1. Imatinib Dasatinib. 22. Nilotinib Cetuximab Panitumumab Erlotinib Trastuzumab Lapatinib. 28. Temsirolimus")
54
The other side Gelimiteerde efficiëntie in een multifactoriële ziekte
Combinatie therapie en multitargeted agents

55
Targeted agents in ontwikkeling:
Anti-IGF Aurora kinase inhibitors Anti-CTL4 Polo-like kinase inhibitors AZD1142 MK0457 PF BI-2536 BI-6727 Anti-HDAC IMC-A12 Anti-HSP90 PHA Anti-proteasome IPI-504 Anti-Her-1/-2 Tremelimumab PS-341 LHB589 MS-275 FK228 Anti-mTOR Vorinostat RAD001 AP23573 Bortezomib HKI-272 Lapatinib Trastuzumab Temsirolimus Cetuximab Panitumumab Erlotinib Gefitinib Imatinib Zalitumumab Nilotinib Anti-bcr/abl and c-kit Anti-EGFR Sunitinib Dasatinib Sorafenib Bevacizumab Aflibercept Bosutinib EKB-569 Approved Vandetanib Pazopanib Vatalanib Cediranib Phase III Axitinibb CHIR-268 Anti-PDGFR AMG706 AEE788 MLN518 BMS XL999 Phase II PD AZD6244 BIBF1120 XL880 BAY Phase I PKC-412 Anti-MEK Anti-VEGFR

56
Targeted Therapy en klinische resultaten: waar staan we?
Relatief lage toxiciteit Antilichamen met schitterende resultaten Klinische efficiëntie in combinatie met cytotoxische drugs Target identificatie bij individuele patiënt is extreem belangrijk

57
Conclusie Nieuw tijdperk in medische oncologie
“Personalised medicine”: patient selectie ! Klinisch effect in combinatie met cytostatica Ongekende toxiciteiten en resistentie Financiële toxiciteit!

58
Dank voor Uw aandacht !

59
The target - mTOR complexes
Soulard et al, Cell 129, April 20, 2007 59

60
TOR controls cell and organism size
Message in a picture TOR controls cell and organism size tor mutant Wild type T. Neufeld

61
mTor (mammalian target of rapamycin)... two complexes
Raptor 4EBP S6K mRNA/Protein translation G1 S TORC 1 Proliferation Torisel / FKBP-12 Rad001 AP23573 Rapamycin -p P- GbL Riktor Akt –S473 Survival TORC 2 mSIN-1 Cytoskeleton PKCz 2549 aa heat repeats FRB kinase FAT domain domain Intracellular complex is very stable and confers an extraordinarily long lasting PD effect Allosteric site of action confers specificity and distinguishes Torisel MOA from that of Sutent and Nexavar

62
Phase III trial of IFL ± Avastin in metastatic CRC (AVF2107g): survival
Median survival (months) IFL + placebo: 15.6 (95% CI: 14.3–17.0) vs IFL + Avastin: 20.3 (95% CI: 18.5–24.2) HR=0.66 (95% CI: 0.54–0.81) p<0.001 1.0 0.8 0.6 0.4 0.2 IFL + Avastin IFL + placebo Probability of survival Trial AVF2107g was a blinded, randomised, placebo-controlled phase III trial of IFL with or without Avastin 5mg/kg every 2 weeks as first-line treatment of metastatic CRC. Survival, the primary endpoint, was significantly increased by 30% in the IFL plus Avastin arm compared with the IFL plus placebo arm (20.3 [95% CI 18.5–24.2] vs 15.6 [95% CI 14.3–17.0] months, respectively; p<0.001).1 The HR of death for IFL plus Avastin relative to IFL plus placebo was estimated to be 0.66 (95% CI 0.54–0.81). This corresponds to a reduction of 34% in the risk of death in the IFL plus Avastin arm. Hurwitz H, Fehrenbacher L, Novotny W, et al. Bevacizumab plus irinotecan, fluorouracil, and leucovorin for the treatment of metastatic colorectal cancer. N Engl J Med 2004;350:2335–42. 15.6 20.3 Survival (months) CI = confidence interval HR = hazard ratio Hurwitz H, et al. N Engl J Med 2004;350:2335–42
 IFL + placebo: 15.6 (95% CI: 14.3–17.0) vs. IFL + Avastin: 20.3 (95% CI: 18.5–24.2) HR=0.66 (95% CI: 0.54–0.81) p< IFL + Avastin. IFL + placebo. Probability of survival. Trial AVF2107g was a blinded, randomised, placebo-controlled phase III trial of IFL with or without Avastin 5mg/kg every 2 weeks as first-line treatment of metastatic CRC. Survival, the primary endpoint, was significantly increased by 30% in the IFL plus Avastin arm compared with the IFL plus placebo arm (20.3 [95% CI 18.5–24.2] vs 15.6 [95% CI 14.3–17.0] months, respectively; p<0.001).1. The HR of death for IFL plus Avastin relative to IFL plus placebo was estimated to be 0.66 (95% CI 0.54–0.81). This corresponds to a reduction of 34% in the risk of death in the IFL plus Avastin arm. Hurwitz H, Fehrenbacher L, Novotny W, et al. Bevacizumab plus irinotecan, fluorouracil, and leucovorin for the treatment of metastatic colorectal cancer. N Engl J Med 2004;350:2335– Survival (months) CI = confidence interval HR = hazard ratio. Hurwitz H, et al. N Engl J Med 2004;350:2335–42.")
Verwante presentaties








 medische zorg>")


morgen>")









 DIAGNOSTIEK MONITORING ICD’S EN BIVENTRICULAIRE PACING PLOTSE DOOD.>")
